

삼출성 나이관련황반변성은 고령 인구에서 발생하는 실명의 주요 원인으로서,1 국민건강보험공단 자료에 따르면 2017년부터 2021년까지 5년간 국내 황반변성 환자 수는 약 130% 증가하였으며, 이에 따라 황반변성 관련 건강보험 총 진료비도 같은 기간 약 190% 증가하였다. 삼출성 나이관련 황반변성의 예후는 항혈관내피성장인자 유리체 내 주사제의 출현 이후 이전에 비해 크게 호전되었으며, 이는 현재 표준 치료법으로 사용되고 있다.2-4 하지만 항혈관내피성장인자 유리체 내 주사제의 치료 효과를 유지하기 위해서는 수개월 이내의 간격으로 반복적인 주입이 필요한 경우가 많으며,5 이로 인한 빈번한 병원 방문은 환자들에게 큰 경제적 부담이 된다.6,7 또한 반복적인 유리체 내 주사는 유리체출혈, 망막박리, 안내염 등 주사 관련 합병증의 위험을 증가시킨다.8 이러한 단점을 보완하고자, 유리체 내 주사 횟수를 줄이고 비용을 절감할 수 있는 치료법에 대한 연구가 지속되고 있다.9
삼출성 나이관련황반변성은 전형적인 염증성 질환은 아니지만, 질병 병태생리에서 염증 반응은 중요한 기전 중 하나로 여겨지고 있다.10,11 따라서 이 질환에서 증가되어 있는 특정 염증 물질들을 표적으로 하는 다양한 항염증 치료들이 시도되고 있다.10,12 그중 하나가 비스테로이드성 항염증제(nonsteroidal anti-inflammatory drugs, NSAIDs)로, 이는 cyclooxygenase (COX)를 억제하여 prostaglandin의 합성을 막음으로써 염증 반응을 저해하는 효과를 나타낸다.13 브롬페낙은 NSAID 점안제 중에서도 유리체 내 침투력이 높으며, 당뇨황반부종, 포도막염에 의한 황반부종 등 망막 질환에서 브롬페낙의 점안이 황반부종을 감소시킨다는 연구 결과들이 있었다.14-16 또한 삼출성 나이관련황반변성 환자에서 유리체 내 주사 없이 브롬페낙 점안액 단독 치료를 시행한 경우에도 16주 내 망막하액 및 망막내액이 감소하였다는 증례보고가 있다.17
삼출성 나이관련황반변성에서 애플리버셉트는 혈관내피 성장인자에 대한 결합력이 라니비주맙에 비해 더 강하며 작용 시간 역시 더 긴 것으로 나타나 최근 많이 사용되고 있는 항혈관내피성장인자 주사제이다.18,19 그러나 유리체 내 주사와 병용하여 브롬페낙의 점안 효과를 확인하고자 한 이전 연구들은 라니비주맙을 주로 사용하였으며 애플리버셉트와 브롬페낙의 병용 치료에 대한 보고는 거의 없었다.20,21 이에 본 연구에서는 삼출성 나이관련황반변성에서 애플리버셉트 유리체 내 주사의 병용 치료로서 브롬페낙을 사용한 환자들의 2년간의 임상 결과에 대해 확인하고 이를 애플리버셉트 유리체 내 주사 단독 요법과 비교해보고자 하였다.
대상과 방법
본 연구는 본원의 임상시험심사위원회(Institutional Review Board, IRB)의 승인을 받았으며(승인번호: 2023-04-027) 헬싱키선언(Declaration of Helsinki)을 준수하였다.
2014년 8월부터 2020년 12월까지 본원에서 삼출성 나이 관련황반변성으로 처음 진단받고 애플리버셉트(Eylea®, Bayer Pharma AG, Berlin, Germany) 유리체 내 주사 치료를 받은 환자 중 2년 이상 경과 관찰하였던 환자를 대상으로 후향적 의무기록 분석을 하였다. 대상자들은 0.1% 브롬페낙(Bronuck® Ophthalmic Solution, Taejoon Pharm., Seoul, Korea) 점안 유무에 따라 두 군으로 분류되었다. 애플리버셉트 유리체 내 주사만 시행한 군은 애플리버셉트 단독 치료군으로 명명하였으며 2018년 8월 이후의 환자들은 첫 번째 주사 다음 날부터 24개월간 하루 2회 브롬페낙 점안을 지속하였고 브롬페낙 병용 치료군으로 명명하였다.
황반부종을 일으킬 수 있는 당뇨망막병증, 망막혈관폐쇄나 포도막염이 있는 경우, 심한 백내장(Lens Opacities Classification System III상 3단계 이상)이나 유리체출혈 등 심한 매체혼탁이 있는 경우, 시력에 영향을 줄 수 있는 다른 안과적 질환이 동반된 경우, 6개월 이내에 백내장수술 과거력이 있는 경우, 연구 기간 내 다른 약제로 유리체 내 주사를 받거나 유리체망막수술을 받은 경우는 제외하였다.
모든 대상자들은 진단 당시에 최대교정시력(best-corrected visual acuity), 안압, 세극등현미경검사, 산동안저검사, 스펙트럼영역 빛간섭단층촬영(Spectralis, Heidelberg Engineering, Heidelberg, Germany), 형광안저혈관조영술 및 인도시아닌그린혈관조영술(Heidelberg Retina Angiograph 2, Heidelberg Engineering, Heidelberg, Germany)을 시행하였다. 중심망막두께는 빛간섭단층촬영 장비에 내장된 프로그램을 이용하여 측정하였으며 Early Treatment Diabetic Retinopathy Study grid에서 황반부 중심 지름 1 mm 영역의 평균 중심망막두께로 정의하였다. 삼출성 나이관련황반변성은 황반부의 맥락막신생혈관, 망막하액, 망막색소상피박리, 망막하 삼출물과 출혈을 시사하는 과형광 및 후기 누출을 보이는 경우로 정의하였다. 인도시아닌그린혈관조영술에서 분지혈관망과 결절 모양 과형광 병변이 발견되는 경우 결절맥락막혈관병증으로 분류하였으며, 망막 내 혈관신생, 망막-망막혈관문합 혹은 망막-맥락막혈관 문합이 관찰되는 경우 망막혈관종 증식으로 분류하였다. 이러한 소견이 없는 경우에는 전형적 삼출성 나이관련황반변성으로 분류하였다.
대상자들은 진단 후 1개월 간격으로 3회 애플리버셉트 주사를 시행받았다. 이후에는 연구자의 판단에 따라 1-2개월 간격으로 경과 관찰하였으며 재발할 때에만 주사하는 as-needed 방식으로 치료를 하였다. Prospective OCT Imaging of Patients with Neovascular AMD Treated with intraOcular Ranibizumab Study22의 재주사 기준에 따라 1) 빛간섭단층촬영에서 황반부에 망막하액/망막내액이 있으면서 유의한 시력 감소가 있는 경우, 2) 중심망막두께가 100 μm 이상 증가한 경우, 3) 황반부의 새로운 출혈의 발생, 4) 새로운 맥락막신생혈관의 발생이 있는 경우 추가 주사를 시행하였으며 최소 재주사 간격은 8주였다. 유리체 내 주사는 한 명의 망막 전문의(D.H.P)가 시행하였다.
최대교정시력은 5 m용 한천석시력표를 이용하여 측정한 후 통계학적 분석을 위하여 logarithm of the minimal angle of resolution (logMAR)으로 변환하였다. 대상자들의 최대교정시력과 중심망막두께는 처음 진단 시, 6, 12, 18, 24개월째에 측정하였고, 6, 12, 18, 24개월째 총 유리체 내 주사 횟수를 각각 조사하였다.
통계 분석은 IBM SPSS ver. 29.0 (IBM Corp., Armonk, NY, USA)을 이용하였다. 연속형 자료는 평균 ± 표준편차로 표기하고 두 군 간의 비교는 unpaired two sample t-test를 이용하였다. 범주형 자료는 빈도(%)로 표기하고 chi-square test를 이용하였다. Repeated-measures analysis of variances 방법을 이용하여 서로 다른 시점에 측정된 값을 비교하였으며, 두 시점 사이의 비교는 Bonferroni method를 이용하였다. p-value가 0.05 미만인 경우에 통계적으로 유의하다고 판단하였다.
결 과
총 43안(43명)이 연구에 포함되었으며 애플리버셉트 단독 치료군이 25안, 브롬페낙 병용 치료군이 18안이었다. 애플리버셉트 단독 치료군의 평균 연령은 68.4 ± 9.0세, 브롬페낙 병용 치료군의 평균 연령은 69.2 ± 9.7세였으며 두 군 간의 유의한 차이는 없었다(p=0.792). 애플리버셉트 단독 치료군에서 전형적 삼출성 나이관련황반변성은 10안, 결절맥락막혈관병증은 15안, 망막혈관종증식은 0안이었으며, 브롬페낙 병용 치료군에서는 각각 7안, 11안, 0안이었다. 치료 전 최대교정시력(logMAR)은 애플리버셉트 단독 치료군이 0.56 ± 0.28, 브롬페낙 병용 치료군이 0.57 ± 0.23으로 두 군 간의 차이는 없었고(p=0.891), 치료 전 중심망막두께(μm)는 애플리버셉트 단독 치료군이 406.6 ± 83.2 µm, 브롬페낙 병용 치료군이 413.2 ± 108.9 µm로 두 군 간 차이는 없었다(p=0.825). 진단 시 성비, 고혈압, 당뇨, 백내장수술의 과거력, 삼출성 나이관련황반변성 유형 모두 두 군 간의 차이를 보이지 않았다(Table 1).
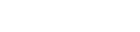
애플리버셉트 유리체 내 주사 시작 후 24개월간 총 주사 횟수를 비교해 보았을 때 6개월, 12개월째에는 두 군 간의 차이가 없었다(p=0.164, p=0.086) (Fig. 1). 18개월과 24개월째에 두 군 사이에 유의한 차이가 있었으며, 브롬페낙 병용 치료군이 애플리버셉트 단독 치료군에 비해 총 주사 횟수가 적었다(18개월, 6.1 ± 0.9회 vs. 7.4 ± 1.7회, p=0.011; 24개월, 7.4 ± 1.0회 vs. 9.0 ± 1.9회, p=0.008). 첫 1개월 간격의 3회 주사 후 24개월간 재발하지 않은 환자는 두 군 모두에서 없었다.
두 군 사이의 최대교정시력(logMAR) 변화를 비교해 보았을 때, 애플리버셉트 단독 치료군은 치료 전 0.56 ± 0.28에서 24개월 후 0.44 ± 0.28로, 브롬페낙 병용 치료군은 치료 전 0.57 ± 0.23에서 24개월 후 0.43 ± 0.19로 두 군 모두 시력 호전을 보였다(p=0.044, p=0.019) (Fig. 2). 모든 시점에서 최대교정시력은 두 군 간 차이는 없었으며(p>0.05), 치료 시작 후 24개월 동안의 최대교정시력의 변화 값은 애플리버셉트 단독 치료군에서 -0.11 ± 0.28, 브롬페낙 병용 치료군에서 -0.14 ± 0.23으로 두 군 모두 24개월째 최대교정시력이 호전되었으며 두 군 사이에 차이는 없었다(p=0.786)(Table 2).
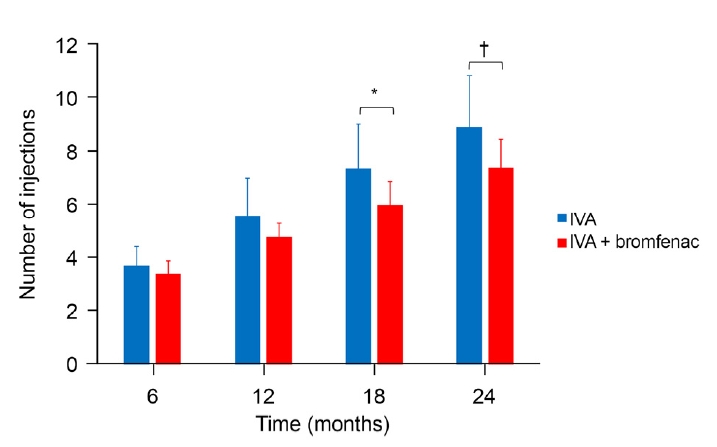
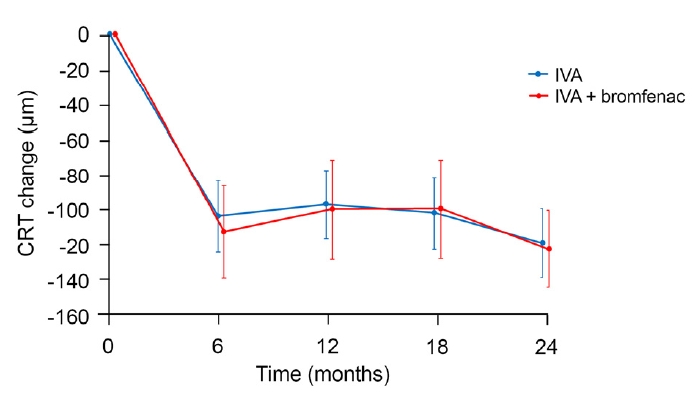
중심망막두께의 경우 애플리버셉트 단독 치료군에서 치료 전 406.6 ± 83.2 μm에서 24개월 후 286.9 ± 52.9 μm로, 브롬페낙 병용 치료군에서는 치료 전 413.2 ± 108.9 μm에서 24개월 후 289.8 ± 55.5 μm로 두 군 모두 유의하게 감소하였다(p<0.001) (Table 2). 또한 24개월간 중심망막두께의 변화값은 모든 시점에서 두 군 간 차이가 없었다(p>0.05) (Fig. 3). 두 군에서 초기 3회 유리체 내 주사 후 시기별 빛간섭단층촬영 대표 증례를 Fig. 4에 제시하였다. 본 연구 기간 동안 망막박리, 안내염 등 유리체 내 주사 후 심각한 부작용은 관찰되지 않았으며 브롬페낙 점안 후 각막 합병증 등 부작용으로 인해 약제 사용을 중단한 사례는 없었다.
고 찰
삼출성 나이관련황반변성에서는 브루크막의 파열 부위를 통해 망막색소상피층의 하부 혹은 위층으로 맥락막신생혈관(choroidal neovascularization, CNV)이 형성되거나 망막혈관에서부터 맥락막 쪽으로 혈관신생이 발생한다.23 이러한 신생혈관 증식을 유발하는 대표적 요인으로 혈관내피 성장인자(vascular endothelial growth factor, VEGF)가 있으며 브루크막에서 임파구, 섬유모세포, 대식세포 등 염증인자가 증가되어 있어 염증 반응 또한 중요한 역할을 한다고 알려져 있다.24 염증 반응으로 발생되는 prostaglandin은 염증 매개체로서 혈관확장, 혈관 투과도 증가 및 혈액망막장벽의 손상을 유발한다.14 COX는 prostaglandin 생성 과정의 중요한 효소로, 특히 COX-2와 이로 생성된 prostaglandin은 혈관 투과도 증가 및 혈관-유리체장벽의 파괴를 유발하여 염증을 촉진할 뿐만 아니라, VEGF 및 이의 수용체 발현을 증가시켜 CNV의 형성과 망막부종에 영향을 준다고 알려져 있다.12,14
NSAID는 COX 저해제로서 몇몇 연구에서 NSAID 점안제가 VEGF를 하향 조절하여 CNV 형성을 억제한다는 결과가 있었고 브롬페낙은 NSAID 점안제 중에서도 유리체 내 침투력이 높으며 COX-2에 더 선택적으로 작용하는 것으로 알려져 있다.25-27 Baklayan et al28은 동물연구에서 브롬페낙 점안 24시간 후 망막, 맥락막 및 공막에서 브롬페낙의 검출을 확인하였다. Pastore et al29은 유리체절제술을 받을 환자들을 대상으로 수술 3일 전부터 NSAID 점안 후 유리체 내 NSAID 농도 및 prostaglandin E2의 농도를 측정하였다. NSAID를 점안한 군에서 유리체 내 NSAID가 검출되었으며, 대조군과 비교 시 prostaglandin E2의 유의한 감소를 보여 점안 NSAID의 후극부 염증 치료의 가능성을 보고하였다. 다양한 망막 질환에서 브롬페낙 점안의 임상적 유용성을 보여준 여러 연구들도 있었다.16 Pinna et al15은 당뇨황반부종에서 한 달간 브롬페낙 점안 후 중심망막두께가 감소하였음을 보고하였으며, Shimura and Yasuda30는 망막분지정맥폐쇄로 인한 황반부종에서 베바시주맙 유리체 내 주사와 브롬페낙 점안을 병용할 경우 주사 횟수가 유의하게 적음을 보고하였다.
Flaxel et al20은 삼출성 나이관련황반변성 환자를 대상으로 라니비주맙 단독 치료군과 브롬페낙 병용 치료군을 비교하였으며 12개월간 유리체 내 주사 횟수는 두 군 사이에 유의한 차이가 없다고 보고하였다. 본 연구에서도 기존의 연구와 유사하게 1개월 간격의 연속된 주사 후 as-needed 방식으로 치료하였으며 1년째까지의 총 주사 횟수는 두 군 간 차이가 없었다. 그러나 18개월째부터는 브롬페낙을 병용한 군과 애플리버셉트 단독 치료군 사이에 유의한 차이가 발생하였다. 이러한 결과가 나타난 이유로는 두 군 모두 공통적으로 초기에 3회의 연속된 주사 치료를 받았기 때문에 1년째까지는 주사 횟수의 차이가 통계적으로 유의하지 않았을 수 있으며 1년 이상 경과 관찰하였을 때 두 군 간 주사 횟수에 차이가 나타났을 것으로 생각된다. 즉, as-needed 방식에서 1년 이상 장기적으로 브롬페낙을 점안할 경우 총 주사 횟수의 감소로 이어져 환자들에게도 경제적으로 도움이 될 것으로 생각된다.
본 연구에서 최대교정시력은 치료 시작 2년째 두 군 모두에서 초기보다 시력 호전이 있었으며 이는 기존의 연구와 유사한 결과를 보여주었다. Weber et al31은 삼출성 나이관련황반변성 환자를 대상으로 애플리버셉트 유리체 내 주사를 as-needed 방식으로 시행한 연구에서 24개월째 시력 호전이 있음을 보고한 바 있다. 또한 본 연구에서 두 군 간 최대교정시력에는 차이가 없었는데 이를 통해 브롬페낙 점안을 병용하더라도 시력에는 영향을 주지 않음을 알 수 있었다.
NSIAD 점안제의 부작용으로 디클로페낙과 케토롤락 점안 후 각막궤양 및 각막 융해와 같은 심각한 각막 합병증이 보고된 바 있으나32 브롬페낙 점안액에서는 안구 자극감 등 경한 부작용이 주로 확인되었다.16 본 연구 기간 동안에도 브롬페낙 점안과 관련된 심각한 부작용은 관찰되지 않았으며 다른 각막 질환이 없는 한 브롬페낙 점안액은 비교적 안전한 약제로 망막 질환의 치료에 도움이 될 것으로 기대된다.
본 연구의 제한점은 다음과 같다. 본 연구는 후향적 연구로 적은 수의 환자를 대상으로 하였으며 경과 관찰이 엄격한 기준에 의해 시행되지 않았다. 일부 환자에서는 경과 관찰 사이의 기간이 연장되어 재발이 늦게 발견되었을 수 있으며 이로 인해 주사 횟수가 적었을 가능성도 있다. 따라서 보다 정확한 자료를 얻기 위해서는 엄격하게 as-needed 방식으로 치료한 전향적 연구가 필요할 것이다. 또한 본 연구는 as-needed 방식으로 치료를 시행하였으나 treat-and-extend 방식으로 치료 후 브롬페낙 점안액을 병용한 결과에 대한 비교 연구도 필요할 것으로 보인다.
현재까지 라니비주맙 유리체 내 주사 치료와 NSAID 점안제의 병용 치료를 연구한 결과들은 있었으나, 애플리버셉트 유리체 내 주사 치료와 브롬페낙 점안액을 병용한 결과에 관한 연구는 없었다. 또한 기존 연구들은 평균 추적 기간이 8.7개월(6-12개월)로 짧은 기간에 비해 본 연구는 2년이라는 비교적 긴 기간의 관찰 결과를 분석하였다. 본 연구에서는 삼출성 나이관련황반변성에서 애플리버셉트 유리체 내 주사와 브롬페낙 점안을 병용한 경우 주사 횟수가 줄어드는 경향이 나타났다. 이러한 경향을 보다 명확하게 증명하기 위해서는 향후 잘 설계되고 더 많은 환자를 대상으로 하는 추가적인 연구가 필요할 것이다.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






