

ļģ╣ļé┤ņןņØĆ ņĢłņĢĢņāüņŖ╣ ļśÉļŖö ĒśłņĢĪņł£ĒÖś ņןņĢĀ ļō▒ ļŗżņ¢æĒĢ£ ņøÉņØĖņ£╝ļĪ£ ņŗ£ņŗĀĻ▓ĮņØ┤ ņĀÉņ░© ņåÉņāüļÉśņ¢┤ ņŗ£ņĢ╝Ļ▓░ņåÉņØ┤ ņ¦äĒ¢ēĒĢśļŖö ņ¦łĒÖśņØ┤ļŗż[1]. Ļ░£ļ░®Ļ░üļģ╣ļé┤ņן ņ╣śļŻīņŚÉņä£ Ļ░Ćņן ņżæņÜöĒĢ£ Ļ▓āņØĆ ņĢłņĢĢņØä ļé«ņČöļŖö Ļ▓āņØ┤ļ®░[2], ĻĘĖ ļ░®ļ▓Ģņ£╝ļĪ£ļŖö ņĢĮļ¼╝ņ╣śļŻī, ļĀłņØ┤ņĀĆņ╣śļŻī, ņłśņłĀņĀü ņ╣śļŻīĻ░Ć ņ׳ļŗż. ļīĆĻ░£ ņĢĮļ¼╝ņ╣śļŻīļź╝ ļ©╝ņĀĆ ņŗ£Ē¢ēĒĢśņ¦Ćļ¦ī, ņĢłņĢĢ ņĪ░ņĀłņŚÉ ņŗżĒī©ĒĢśĻ▒░ļéś ņĢĮļ¼╝ ļé┤ņä▒ņØ┤ļéś ļČĆņ×æņÜ®ņØ┤ ļ░£ņāØĒĢśļ®┤ ņłśņłĀņĀü ļ░®ļ▓ĢņØä ņé¼ņÜ®ĒĢśĻ▓ī ļÉ£ļŗż. ņłśņłĀņĀü ņ╣śļŻī ļ░®ļ▓Ģ ņżæ ņä¼ņ£ĀņŻ╝ņĀłņĀ£ņłĀņØĆ Ēśäņ×¼ Ļ░Ćņן ļäÉļ”¼ ņé¼ņÜ®ļÉśĻ│Ā ņ׳ļŖö ņŚ¼Ļ│╝ņłśņłĀļ▓Ģņ£╝ļĪ£[3], 67-94%ņØś ļåÆņØĆ ņä▒Ļ│ĄļźĀņØä ļ│┤ņØ┤ņ¦Ćļ¦ī, ņłĀ Ēøä ĒĢ®ļ│æņ”Ø ļśÉĒĢ£ ļ¦ÄņØ┤ ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ļŗż[4-6].
ņĄ£ĻĘ╝ņŚÉļŖö ļ»ĖņäĖņ╣©ņŖĄ ļģ╣ļé┤ņןņłśņłĀ(micro-invasive glaucoma surgery, MIGS)ļØ╝ ļČłļ”¼ļŖö ņāłļĪ£ņÜ┤ ļ░®ļ▓ĢņØ┤ Ļ░£ļ░£ļÉśņ¢┤ ņĢĮļ¼╝ņØś Ēł¼ņĢĮ ļČĆļŗ┤Ļ│╝ ĒĢ®ļ│æņ”ØņØä ņżäņØ┤ļŖö ĒÜ©Ļ│╝ņĀüņØĖ ņĢłņĢĢĻ░ÉņåīņØś ļīĆņĢłņØä ņĀ£Ļ│ĄĒĢśĻ│Ā ņ׳ļŗż[7]. ļśÉĒĢ£ MIGSļŖö ņ×Āņ×¼ņĀüņ£╝ļĪ£ ļŹö ņ╣©ņŖĄņĀüņØĖ ļģ╣ļé┤ņןņłśņłĀņØś ĒĢäņÜöņä▒ņØä Ļ░Éņåīņŗ£ĒéżĻ│Ā ņ¦ĆņŚ░ņŗ£Ēé¼ ņłś ņ׳ņØä Ļ▓āņØ┤ļŗż. ļ¦ÄņØĆ ņóģļźśņØś MIGS ņןņ╣śļōżņØ┤ ņ׳ņ£╝ļ®░[8-13], ĻĘĖņżæ ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖ(trabecular micro-bypass stent, iStent)ņØś ņ×äņāü Ļ▓░Ļ│╝ņŚÉ ļīĆĒĢ£ ĻĄŁņÖĖ ņŚ░ĻĄ¼ ļ│┤Ļ│ĀļŖö ļ¦ÄņØ┤ ņ׳ļŗż[14-19]. ĻĄŁļé┤ņŚÉļŖö ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖĻ░Ć Ēśäņ×¼ Ļ░Ćņן ļ©╝ņĀĆ ļÅäņ×ģņØ┤ ļÉśņ¢┤ņä£ ņé¼ņÜ®ļÉśņŚłņ¦Ćļ¦ī, ĻĄŁļé┤ņŚÉ ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņéĮņ×ģņłĀ(iStent ņéĮņ×ģņłĀ)ņØś ņ×äņāüĻ▓░Ļ│╝, ņĢłņĢĢĒĢśĻ░Ģ ĒÜ©Ļ│╝ ļ░Å ņØ┤ņÖĆ Ļ┤ĆļĀ©ļÉ£ ņØĖņ×ÉņŚÉ ļīĆĒĢ┤ņä£ļŖö ņ¦ĆĻĖłĻ╣īņ¦Ć ļ│┤Ļ│ĀļÉ£ ļ░öĻ░Ć ņŚåļŗż. ļö░ļØ╝ņä£, ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ļŖö Ļ░£ļ░®Ļ░üļģ╣ļé┤ņן ĒÖśņ×ÉļōżņŚÉņä£ ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņéĮņ×ģņłĀņØä ņŗ£Ē¢ēĒĢ£ Ēøä 6Ļ░£ņøöĻ░äņØś ņ×äņāü Ļ▓░Ļ│╝ ļ░Å ņ╣śļŻī Ļ▓░Ļ│╝ņŚÉ ņśüĒ¢źņØä ļ»Ėņ╣śļŖö ņśłĒøä ņØĖņ×ÉļōżņŚÉ ļīĆĒĢ┤ ļČäņäØĒĢśĻ│Āņ×É ĒĢśņśĆļŗż.
ļīĆņāüĻ│╝ ļ░®ļ▓Ģ
2018ļģä 3ņøöļČĆĒä░ 2018ļģä 12ņøöĻ╣īņ¦Ć ņ¢æņé░ļČĆņé░ļīĆĒĢÖĻĄÉļ│æņøÉĻ│╝ ļČĆņé░ļīĆĒĢÖĻĄÉļ│æņøÉņŚÉņä£ Ļ░£ļ░®Ļ░üļģ╣ļé┤ņןņØä ņ¦äļŗ©ļ░øĻ│Ā ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņéĮņ×ģņłĀ ļŗ©ļÅģ, ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņéĮņ×ģņłĀĻ│╝ ļ░▒ļé┤ņןņłśņłĀ ļ│æĒĢ®ņØä ņŗ£Ē¢ēĒĢ£ ĒÖśņ×Éļź╝ ļīĆņāüĻĄ░ņ£╝ļĪ£, Ļ░ÖņØĆ ĻĖ░Ļ░ä ļ░▒ļé┤ņןņłśņłĀļ¦ī ļŗ©ļÅģ ņŗ£Ē¢ēĒĢ£ ĒÖśņ×Éļź╝ ļīĆņĪ░ĻĄ░ņ£╝ļĪ£ ĒøäĒ¢źņĀüņ£╝ļĪ£ ļČäņäØĒĢśņśĆļŗż. ņČöņĀü Ļ┤Ćņ░░ņØ┤ 6Ļ░£ņøö ņØ┤ņāüņØĖ ĒÖśņ×ÉļōżņØä ļīĆņāüņ£╝ļĪ£, ņĀäļ░®Ļ░üņØ┤ Ļ░£ļ░®ļÉśņ¢┤ ņ׳ņ£╝ļ®░, ļģ╣ļé┤ņן ņ╣śļŻī ņĀä ņĢłņĢĢņØ┤ 21 mmHg ņØ┤ņāüņØ┤ņŚłļŹś ņØ╝ņ░©ņä▒ ļśÉļŖö ņØ┤ņ░©ņä▒ Ļ░£ļ░®Ļ░üļģ╣ļé┤ņןļ¦ī ĒżĒĢ©ņŗ£ņ╝░ņ£╝ļ®░, ņĀäļ░®Ļ░üĻ▓ĮĻ▓Ćņé¼ņāü ņä¼ņ£ĀņŻ╝Ļ░Ć 3ņé¼ļČäļ®┤ ņØ┤ņāüņŚÉņä£ ļ│┤ņØ┤ņ¦Ć ņĢŖĻ▒░ļéś ņŻ╝ļ│ĆļČĆ ĒÖŹņ▒ä ņĀäņ£Āņ░®ņØ┤ ņ׳ļŖö ĒÅÉņćäĻ░ü ļģ╣ļé┤ņןņØĆ ņĀ£ņÖĖĒĢśņśĆļŗż. ņłśņłĀ ņĀä ļģ╣ļé┤ņן ņĢĮļ¼╝ņ╣śļŻīļź╝ ļ░øņØĆ ĒÖśņ×ÉļōżņØä ļīĆņāüņ£╝ļĪ£ ĒĢśņśĆņ£╝ļ®░, ļģ╣ļé┤ņן ņĢĮļ¼╝ņ╣śļŻīļĪ£ ņĢłņĢĢņØ┤ 21 mmHg ņØ┤ĒĢśļĪ£ Ļ░ÉņåīĒĢ£ ĒÖśņ×ÉļŖö ņĀ£ņÖĖĒĢśņ¦Ć ņĢŖņĢśļŗż. ļśÉĒĢ£, ņØ┤ņĀäņŚÉ ņĢł ņłśņłĀņØś ļ│æļĀźņØ┤ ņ׳Ļ▒░ļéś ņĢłņ¦łĒÖśņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░, ĻĘĖļ”¼Ļ│Ā ņŗ£ņĢ╝ņŚÉ ņØ┤ņāüņØä ņ£Āļ░£ĒĢĀ ņłś ņ׳ļŖö ņŗĀĻ▓ĮĒĢÖņĀü ņ¦łĒÖśņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ ņŚ░ĻĄ¼ ļīĆņāüņŚÉņä£ ņĀ£ņÖĖĒĢśņśĆļŗż. ļ│Ė ņŚ░ĻĄ¼ļŖö ĒŚ¼ņŗ▒ĒéżņäĀņ¢ĖņØä ņżĆņłśĒĢśņŚ¼ ņŗ£Ē¢ēļÉśņŚłĻ│Ā, ņ¢æņé░ļČĆņé░ļīĆĒĢÖĻĄÉļ│æņøÉĻ│╝ ļČĆņé░ļīĆĒĢÖĻĄÉļ│æņøÉ ņāØļ¬ģņ£żļ”¼ņ£äņøÉĒÜīņØś ņŗ¼ņé¼ļź╝ ļ░øĻ│Ā, ņŖ╣ņØĖ ļ░øņĢśļŗż(ņŖ╣ņØĖ ļ▓łĒśĖ: 05-2019-102, IRB No 1909-002-082).
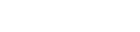
ņłśņłĀņØĆ 2ļ¬ģņØś ņłśņłĀņ×É(J.H.S, J.W.L)ņŚÉ ņØśĒĢ┤ ņŗ£Ē¢ēļÉśņŚłļŗż. iStent (Glaukos Corp., Laguna Hills, CA, USA)ļŖö ļåÆņØ┤ 0.33 mm, ĻĖĖņØ┤ 1.00 mmņØś L ļ¬©ņ¢æņØś ĒŚżĒīīļ”░ņ£╝ļĪ£ ņĮöĒīģļÉ£ Ēŗ░ĒāĆļŖä ņŖżĒģÉĒŖĖņØ┤ļ®░, 1ĒÜīņÜ® ņØĖņä£Ēä░ņŚÉ ņäżņ╣śļÉśņ¢┤ ņ׳ļŗż. 0.5% proparacaine hydrochloride (Alcaine, Alcon, Fort Worth, TX, USA)ļĪ£ ņĀÉņĢłļ¦łņĘ©ĒĢśņŚÉ 5% potadine ņÜ®ņĢĪņ£╝ļĪ£ Ļ▓░ļ¦ē ņåīļÅģ Ēøä ņŗ£Ē¢ēļÉśņŚłļŗż. ņØ┤ņĖĪļČĆņŚÉ Ēł¼ļ¬ģĻ░üļ¦ēņĀłĻ░£ļź╝ ĒĢśĻ│Ā ņĀÉĒāäļ¼╝ņ¦ł 1.4% sodium hyaluronate (Healon GV, Johnson & Johnson Surgical Vision, Inc., Santa Ana, CA, USA)ņØä ņĀäļ░®ņŚÉ ņ▒äņøī ņĀäļ░®Ļ░üņØä Ļ╣ŖĻ▓ī ĒĢśĻ│Ā ņĀäļ░®ņØä ņ£Āņ¦ĆĒĢśņśĆļŗż. ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņéĮņ×ģņłĀĻ│╝ ļ░▒ļé┤ņןņłśņłĀ ļ│æĒĢ®ņØä ĒĢśļŖö Ļ▓ĮņÜ░ ļ░▒ļé┤ņןņłśņłĀņØä ļ©╝ņĀĆ ņŗ£Ē¢ēĒĢśņśĆļŗż. ņØĖĻ│ĄņłśņĀĢņ▓┤ Ļ┤æĒĢÖļČĆļ│┤ļŗż ņĢĮĻ░ä ņ×æņØĆ 5 mm Ēü¼ĻĖ░ņØś ņøÉĒśĢ ņĀäļéŁ ņĀłĻ░£ļź╝ ņŗ£Ē¢ēĒĢśņśĆļŗż. Ļ┤ĆļźśņĢĪņØä ņé¼ņÜ®ĒĢśņŚ¼ ņłśļĀźļČäļ”¼ņłĀ Ēś╣ņØĆ ņłśļĀźļČäņĖĄņłĀņØä ņŗ£Ē¢ēĒĢ£ ļÆż ņ┤łņØīĒīī ņ£ĀĒÖöĻĖ░(Infinity, Alcon, Fort Worth, TX, USA)ļĪ£ ĒĢĄņØś ņłśņĀĢņ▓┤ņ£ĀĒÖöņłĀĻ│╝ Ēö╝ņ¦ł ĒØĪņ×ģņØä ņŗ£Ē¢ēĒĢśņśĆĻ│Ā ņØĖĻ│ĄņłśņĀĢņ▓┤ļź╝ ņØĖņĀØĒä░ ņŗ£ņŖżĒģ£(injector system)ņ£╝ļĪ£ ņłśņĀĢņ▓┤ ļéŁļé┤ņŚÉ ņéĮņ×ģĒĢśņśĆļŗż. ņĀäļ░®Ļ░üĻ▓ĮņØä ĒåĄĒĢ┤ ņä¼ņ£ĀņŻ╝ņÖĆ ņē┤ļĀśĻ┤ĆņØś ņ£äņ╣śļź╝ ĒÖĢņØĖĒĢśĻ│Ā Ļ░üļ¦ēņĀłĻ░£ ļČĆņ£äļź╝ ĒåĄĒĢ┤ ņØĖņä£Ēä░ļź╝ ļäŻņØĆ Ēøä ņŖżĒģÉĒŖĖļź╝ ņē┤ļĀśĻ┤ĆņŚÉ ņłśņ¦üņ£╝ļĪ£ ņéĮņ×ģĒĢśņśĆļŗż. ņŖżĒģÉĒŖĖĻ░Ć ņĀüņĀłĒĢ£ ņ£äņ╣śņŚÉ ņéĮņ×ģļÉ£ Ļ▓āņØä ĒÖĢņØĖĒĢ£ Ēøä ņĀÉĒāäļ¼╝ņ¦łņØä ņĀ£Ļ▒░ĒĢśņśĆĻ│Ā, Ēł¼ļ¬ģĻ░üļ¦ēņĀłĻ░£ļŖö ĻĖ░ņ¦łņłśĒÖö(stromal hydration)ļź╝ ņŗ£Ē¢ēĒĢśņśĆļŗż(Fig. 1). ņĢłņĢĮņØĆ ņłĀ Ēøä 0.5% levofloxacin (Cravit┬«, Santen Pharmaceutical Co., Ltd., Osaka, Japan)Ļ│╝ 1% prednisolone acetate (Predforte┬«, Allergan Inc., Irvine, CA, USA)ņØä ĒĢśļŻ© 4ĒÜī ņĀÉņĢłĒĢśļÅäļĪØ ĒĢśņśĆļŗż.
ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņéĮņ×ģņłĀņØś ņłśņłĀ ņä▒Ļ│Ą ĻĖ░ņżĆņØĆ ņĢłņĢĢ ĻĖ░ņżĆņ£╝ļĪ£ ņĀĢņØśĒĢśņŚ¼ ļČäņäØĒĢśņśĆļŗż. ļģ╣ļé┤ņן ņĢĮļ¼╝ņ╣śļŻīļź╝ ļ│æĒ¢ēĒĢśĻ▒░ļéś ĒĢśņ¦Ć ņĢŖļŖö ļ¬©ļōĀ Ļ▓ĮņÜ░ņŚÉņä£ ņłśņłĀ Ēøä ņĢłņĢĢņØ┤ 21 mmHg ļ»Ėļ¦īņØ┤Ļ│Ā, 20% ņØ┤ņāü ņĢłņĢĢņØ┤ Ļ░ÉņåīĒĢ£ Ļ▓ĮņÜ░ļź╝ ņä▒Ļ│Ąņ£╝ļĪ£ ņĀĢņØśĒĢśņśĆļŗż.
ĒåĄĻ│äņ▓śļ”¼ļŖö SPSS for Windows 18.0 (SPSS Inc, Chicago, IL, USA) ĒåĄĻ│ä ĒöäļĪ£ĻĘĖļשņØä ņØ┤ņÜ®ĒĢśņśĆņ£╝ļ®░, Kolmogorov-Smirnov Ļ▓ĆņĀĢņāü ņĀĢĻĘ£ņä▒ ļČäĒżļź╝ ĒÖĢņØĖĒĢśņśĆļŗż. ņłśņłĀ ņĀä ļīĆņĪ░ĻĄ░Ļ│╝ ļ╣äĻĄÉļź╝ ņ£äĒĢśņŚ¼ student t-testļź╝ ņé¼ņÜ®ĒĢśņśĆĻ│Ā, ņłśņłĀ ņĀäĒøä ļ│Ćņłś ļ╣äĻĄÉļź╝ ņ£äĒĢśņŚ¼ ļ¬©ņłś ļČäņäØņØĆ paired t-test ļ░Å ļ╣äļ¬©ņłś ļČäņäØņØĆ Wilcoxon signed rank testļź╝ ņé¼ņÜ®ĒĢśņśĆļŗż. ņłśņłĀ ņä▒Ļ│ĄļźĀ(cumulative probabilities of success) ĒÅēĻ░Ćļź╝ ņ£äĒĢśņŚ¼ Kaplan-Meier ņāØņĪ┤ ļČäņäØņØä ņé¼ņÜ®ĒĢśņśĆņ£╝ļ®░, ļéśņØ┤ ĻĖ░ņżĆņ£╝ļĪ£ ņłśņłĀ ņä▒Ļ│ĄļźĀņØś ļ╣äĻĄÉ ļČäņäØņØä ņ£äĒĢśņŚ¼ log-rank testļź╝ ņé¼ņÜ®ĒĢśņśĆļŗż. ņ£ĀņØśļÅä(pĻ░Æ) 0.05 ļ»Ėļ¦īņØĖ Ļ▓ĮņÜ░ļź╝ ĒåĄĻ│äņĀüņ£╝ļĪ£ ņ£ĀņØśĒĢ£ Ļ▓āņ£╝ļĪ£ Ļ░äņŻ╝ĒĢśņśĆļŗż. ņłĀ Ēøä 6Ļ░£ņøöņŚÉ ņłśņłĀ ņä▒Ļ│Ą ņŚ¼ļČĆņŚÉ ņśüĒ¢źņØä ņŻ╝ļŖö ņłĀ ņĀä ņØĖņ×É ļČäņäØņØä ņ£äĒĢ£ logistic regression ļČäņäØņØä ņé¼ņÜ®ĒĢśņśĆĻ│Ā, ņ£ĀņØśĒĢ£ ņłśņżĆ(p<0.10)ņØś ļ¬©ļōĀ ļ│Ćņłśļź╝ ļŗżļ│Ćļ¤ē ļ¬©ļŹĖņØä ņé¼ņÜ®ĒĢśņŚ¼ ĒÅēĻ░ĆĒĢśņśĆļŗż.
Ļ▓░ Ļ│╝
Ļ░£ļ░®Ļ░üļģ╣ļé┤ņןņØä ņ¦äļŗ©ļ░øĻ│Ā ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņéĮņ×ģņłĀņØä ņŗ£Ē¢ēĒĢ£ ĒÖśņ×ÉļŖö 33ļ¬ģ 33ņĢł, ļ░▒ļé┤ņןņłśņłĀļ¦ī ļŗ©ļÅģņØä ņŗ£Ē¢ēĒĢ£ ĒÖśņ×ÉļŖö 13ļ¬ģ 13ņĢłņØ┤ņŚłļŗż. ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņéĮņ×ģņłĀņØä ņŗ£Ē¢ēĒĢ£ ĒÖśņ×ÉĻĄ░ņŚÉņä£ ļé©ņ×ÉļŖö 28ļ¬ģ, ņŚ¼ņ×ÉļŖö 5ļ¬ģņØ┤ņŚłņ£╝ļ®░, ĒÅēĻĘĀ ņŚ░ļĀ╣ņØĆ 62.42 ┬▒ 16.57ņäĖņØ┤ļ®░, ņłśņłĀ ņĀä ņŗ£ņĢ╝ Ļ▓Ćņé¼ Ļ▓░Ļ│╝ņŚÉņä£ mean deviation (MD)ņØĆ -16.89 ┬▒ 10.68 dB, pattern standard deviation (PSD)ņØĆ 7.30 ┬▒ 3.75 dBņØ┤ņŚłļŗż. ļ░▒ļé┤ņןņłśņłĀļ¦ī ļŗ©ļÅģ ņŗ£Ē¢ēĒĢ£ ļīĆņĪ░ĻĄ░ņŚÉņä£, ļé©ņ×ÉļŖö 7ļ¬ģ, ņŚ¼ņ×ÉļŖö 6ļ¬ģņØ┤ņŚłņ£╝ļ®░, ĒÅēĻĘĀ ņŚ░ļĀ╣ņØĆ 66.08 ┬▒ 5.56ņäĖņØ┤ļ®░, ņłśņłĀ ņĀä ņŗ£ņĢ╝ Ļ▓Ćņé¼ Ļ▓░Ļ│╝ņŚÉņä£ MDņØĆ -13.81 ┬▒ 8.76 dB, PSDņØĆ 5.48 ┬▒ 3.64 dBņØ┤ņŚłļŗż(Table 1).
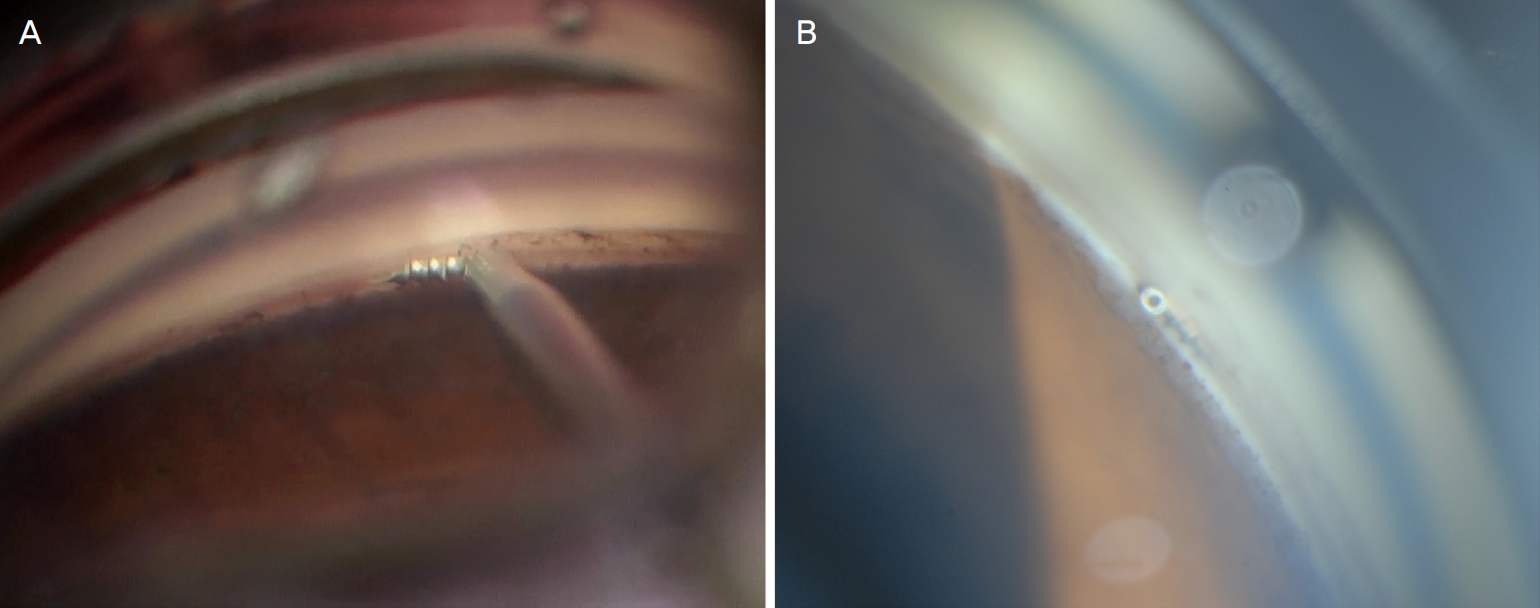
ĒÅēĻĘĀ ņĢłņĢĢņØś Ļ▓ĮņÜ░, ņłĀ ņĀä ņĢłņĢĢņŚÉ ļ╣äĒĢśņŚ¼, ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜīņŖżĒģÉĒŖĖņéĮņ×ģņłĀ ņŗ£Ē¢ēĒĢ£ ĻĄ░ņØĆ ņłĀ ņĀä 23.70 ┬▒ 6.26 mmHgņŚÉņä£, ņłĀ Ēøä 1Ļ░£ņøö, 3Ļ░£ņøö ļ░Å 6Ļ░£ņøöņŚÉ Ļ░üĻ░ü 15.73 ┬▒ 3.68 mmHg, 17.03 ┬▒ 5.79 mmHg, 18.03 ┬▒ 4.64 mmHgļĪ£(ļ¬©ļæÉ p<0.001), ĒÅēĻĘĀ ļģ╣ļé┤ņן ņĢĮļ¼╝ Ļ░£ņłśļÅä ņłĀ ņĀä 3.73 ┬▒ 0.67Ļ░£ņŚÉ ļ╣äĒĢ┤, ņłĀ Ēøä 1Ļ░£ņøö, 3Ļ░£ņøö ļ░Å 6Ļ░£ņøöņŚÉ Ļ░üĻ░ü 3.03 ┬▒ 1.01Ļ░£, 3.42 ┬▒ 0.66Ļ░£, 3.43 ┬▒ 0.67Ļ░£ļĪ£ ņ£ĀņØśĒĢśĻ▓ī Ļ░ÉņåīĒĢśņśĆļŗż(Ļ░üĻ░ü, p<0.001, p=0.037, p=0.027) (Fig. 2).
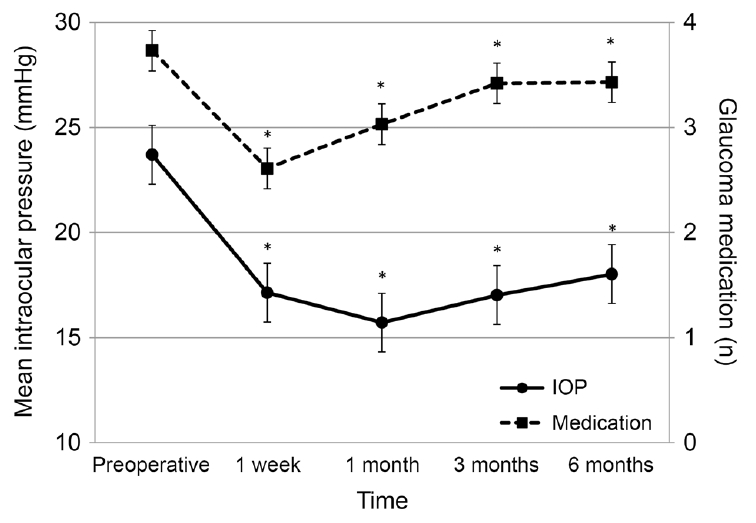
ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņéĮņ×ģņłĀ ņŗ£Ē¢ēĒĢ£ ĻĄ░ņØä ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖ ļŗ©ļÅģĻĄ░ ļ░Å ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖ ņéĮņ×ģĻ│╝ ļ░▒ļé┤ņןņłśņłĀ ļ│æĒĢ®ĻĄ░ņ£╝ļĪ£ ļéśļłäņ¢┤ ļČäņäØĒĢśņśĆņØä ļĢī, ĒÅēĻĘĀ ņĢłņĢĢņØś Ļ▓ĮņÜ░, ņłĀ ņĀä ņĢłņĢĢņŚÉ ļ╣äĒĢśņŚ¼ ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖ ļŗ©ļÅģĻĄ░ņØĆ ņłĀ ņĀä 26.25 ┬▒ 5.24 mmHgņŚÉņä£, ņłĀ Ēøä 1Ļ░£ņøö, 3Ļ░£ņøö ļ░Å 6Ļ░£ņøöņŚÉ Ļ░üĻ░ü 16.54 ┬▒ 3.68 mmHg, 17.67 ┬▒ 6.18 mmHg, 19.04 ┬▒ 4.63 mmHg (ļ¬©ļæÉ p<0.001), ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņÖĆ ļ░▒ļé┤ņןņłśņłĀ ļ│æĒĢ®ĻĄ░ņØĆ ņłĀ ņĀä 16.59 ┬▒ 2.42 mmHgņŚÉņä£, Ļ░üĻ░ü 13.22 ┬▒ 2.49 mmHg, 13.33 ┬▒ 1.80 mmHg, 13.89 ┬▒ 1.90 mmHg (Ļ░üĻ░ü, p=0.012, p=0.007, p=0.002), ļīĆņĪ░ĻĄ░ņØĆ ņłĀ ņĀä 16.23 ┬▒ 2.31 mmHgņŚÉņä£, Ļ░üĻ░ü 14.54 ┬▒ 2.37 mmHg, 13.85 ┬▒ 2.38 mmHg, 13.85 ┬▒ 2.44 mmHgļĪ£ ņäĖ ĻĄ░ ļ¬©ļæÉņŚÉņä£ ĒåĄĻ│äņĀüņ£╝ļĪ£ ņ£ĀņØśĒĢśĻ▓ī Ļ░ÉņåīĒĢśņśĆļŗż(Ļ░üĻ░ü, p=0.038, p=0.005, p=0.005) (Table 2, Fig. 3A).
ĒÅēĻĘĀ ļģ╣ļé┤ņן ņĢĮļ¼╝ Ļ░£ņłśļÅä ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖ ļŗ©ļÅģĻĄ░ņØĆ ņłĀ ņĀä 3.83 ┬▒ 0.48Ļ░£ņŚÉ ļ╣äĒĢ┤, ņłĀ Ēøä 1Ļ░£ņøö, 3Ļ░£ņøö ļ░Å 6Ļ░£ņøöņŚÉ Ļ░üĻ░ü 3.04 ┬▒ 1.08Ļ░£, 3.46 ┬▒ 0.66Ļ░£, 3.39 ┬▒ 0.67Ļ░£ļĪ£ ņ£ĀņØśĒĢśĻ▓ī Ļ░ÉņåīĒĢśņśĆĻ│Ā(Ļ░üĻ░ü, p=0.002, p=0.017, p=0.002), ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņÖĆ ļ░▒ļé┤ņןņłśņłĀ ļ│æĒĢ®ĻĄ░ņØĆ ņłĀ ņĀä 3.44 ┬▒ 1.01Ļ░£ņŚÉ ļ╣äĒĢ┤, Ļ░üĻ░ü 2.55 ┬▒ 0.72Ļ░£, 2.78 ┬▒ 0.83Ļ░£, 2.78 ┬▒ 0.44Ļ░£ļĪ£ ņłĀ Ēøä 1Ļ░£ņøöņŚÉļ¦ī ņ£ĀņØśĒĢśĻ▓ī Ļ░ÉņåīĒĢśņśĆĻ│Ā(Ļ░üĻ░ü, p=0.033, p=0.194, p=0.124), ļīĆņĪ░ĻĄ░ņØĆ ņłĀ ņĀä 2.62 ┬▒ 0.87Ļ░£ņŚÉ ļ╣äĒĢ┤, Ļ░üĻ░ü 2.46 ┬▒ 1.58Ļ░£, 2.38 ┬▒ 1.55Ļ░£, 2.53 ┬▒ 1.50Ļ░£ļĪ£ Ļ░ÉņåīĒĢśņśĆņ£╝ļéś, ņ£ĀņØśĒĢśņ¦Ć ņĢŖņĢśļŗż(Table 3, Fig. 3B).
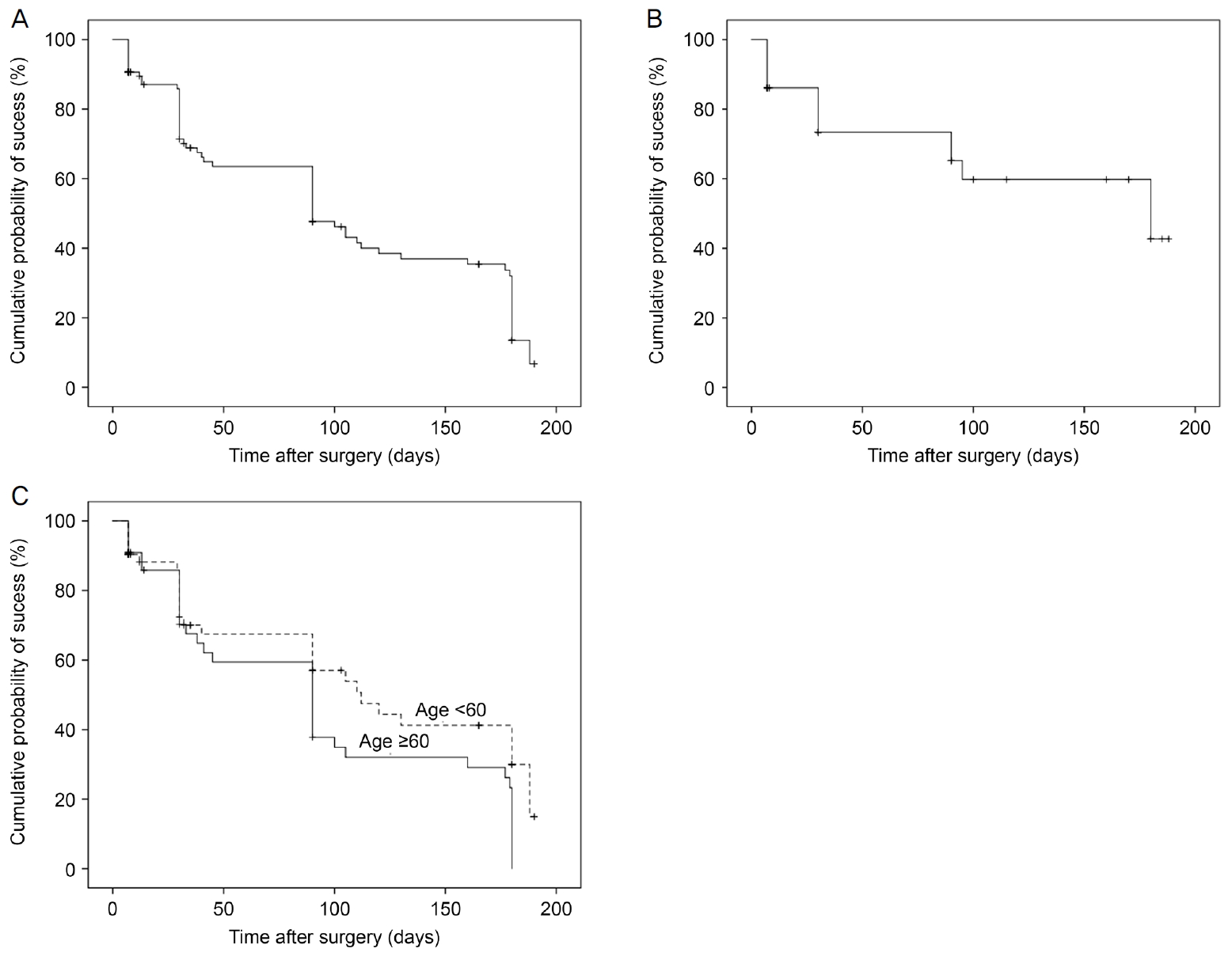
ņłśņłĀ Ēøä ņĢłņĢĢ ĻĖ░ņżĆņŚÉ ļö░ļØ╝ ņłśņłĀ ņä▒Ļ│ĄļźĀņØä ĒīÉļŗ©ĒĢśņśĆņØä ļĢī, 6Ļ░£ņøö Ļ▓ĮĻ│╝ Ļ┤Ćņ░░ Ēøä ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖ ļŗ©ļÅģĻĄ░ņØś ņä▒Ļ│ĄļźĀņØä ļ│┤ļ®┤, Kaplan-Meier ņāØņĪ┤ ļČäņäØ Ļ▓░Ļ│╝ņŚÉ ļö░ļźĖ ļłäņĀü ņłśņłĀ ņä▒Ļ│ĄļźĀņØĆ ņłĀ Ēøä 1Ļ░£ņøöņŚÉņä£ 71.3 ┬▒ 4.9%, ņłĀ Ēøä 3Ļ░£ņøöņŚÉņä£ 58.9 ┬▒ 5.6%, ņłĀ Ēøä 6Ļ░£ņøöņŚÉņä£ 33.7 ┬▒ 5.5%ņØ┤ļ®░(Fig. 4A), ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņÖĆ ļ░▒ļé┤ņןņłśņłĀ ļ│æĒĢ®ĻĄ░ņŚÉņä£ Ļ░üĻ░ü 73.4 ┬▒ 7.7%, 59.8 ┬▒ 9.5%, 42.7 ┬▒ 12.3%ņśĆļŗż(Fig. 4B).
60ņäĖ ĻĖ░ņżĆņ£╝ļĪ£ ļłäņĀü ņłśņłĀ ņä▒Ļ│ĄļźĀņØä ļ╣äĻĄÉ ļČäņäØĒĢśņśĆņØä ļĢī, ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖ ļŗ©ļÅģĻĄ░ņØś 60ņäĖ ļ»Ėļ¦īņŚÉņä£, ņłĀ Ēøä 1Ļ░£ņøö, 3Ļ░£ņøö, 6Ļ░£ņøöņŚÉņä£ Ļ░üĻ░ü 85.9 ┬▒ 5.0%, 59.2 ┬▒ 7.6%, 36.2 ┬▒ 8.1%ņØ┤ļ®░, 60ņäĖ ņØ┤ņāüņŚÉņä£, ņłĀ Ēøä 1Ļ░£ņøö, 3Ļ░£ņøö, 6Ļ░£ņøöņŚÉņä£ Ļ░üĻ░ü 70.2 ┬▒ 7.2%, 38.7 ┬▒ 7.9%, 23.3 ┬▒ 7.0%ļĪ£, 60ņäĖ ļ»Ėļ¦īņŚÉņä£ ļłäņĀü ņłśņłĀ ņä▒Ļ│ĄļźĀņØ┤ 60ņäĖ ņØ┤ņāüņŚÉ ļ╣äĒĢ┤ ņ£ĀņØśĒĢśĻ▓ī ļåÆņØĆ Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż(Fig. 4C) (p=0.023 by the Mantel-Cox log-rank test).
ļéśņØ┤, ņä▒ļ│ä, ņłĀ ņĀä ņĢłņĢĢ, ļģ╣ļé┤ņן ĒāĆņ×ģ, ņłĀ ņĀä ļģ╣ļé┤ņן ņĢĮļ¼╝ Ļ░£ņłś, ņŗ£ņĢ╝Ļ▓Ćņé¼ ņĖĪņĀĢņ╣ś, Ļ░üļ¦ēļæÉĻ╗ś, ņĢłņČĢņן, ļ░▒ļé┤ņןņłśņłĀ ļÅÖļ░ś ņŚ¼ļČĆļź╝ ņłĀ Ēøä ņĢłņĢĢņŚÉ ņśüĒ¢źņØä ļ»Ėņ╣śļŖö ņØĖņ×É ļČäņäØņŚÉ ņé¼ņÜ®ĒĢśņśĆļŗż. ļśÉĒĢ£, ņłśņłĀ ņä▒Ļ│Ą ņŚ¼ļČĆņÖĆ Ļ░ü ņØĖņ×ÉļōżņØś Ļ┤ĆĻ│äļź╝ ļŗżņżæĒÜīĻĘĆļ¬©ĒśĢņØä ņØ┤ņÜ®ĒĢśņŚ¼ ņłśņłĀ ņŗżĒī©ņØś ņ£äĒŚśņØĖņ×Éļź╝ ļČäņäØĒĢ£ Ļ▓░Ļ│╝, ļéśņØ┤Ļ░Ć ņłśņłĀ ņŗżĒī©ņŚÉ ņ£ĀņØśĒĢśĻ▓ī ņśüĒ¢źņØä ņŻ╝ļŖö ņ£äĒŚśņØĖņ×ÉļĪ£ ļéśĒāĆļé¼ļŗż(odds ratio 1.076, 95% ņŗĀļó░ĻĄ¼Ļ░ä 0.996-1.164, p=0.045) (Table 4).
Ļ│Ā ņ░░
ļ│Ė ņŚ░ĻĄ¼ļŖö ĒĢ£ĻĄŁņØĖņŚÉņä£ ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņéĮņ×ģņłĀņØś ļŗ©ĻĖ░Ļ░ä Ļ▓░Ļ│╝ļź╝ ņĢīņĢäļ│┤Ļ│Āņ×É ĒĢśņśĆļŗż. ņłĀ Ēøä 1Ļ░£ņøö, 3Ļ░£ņøö ļ░Å 6Ļ░£ņøö ļ¬©ļæÉņŚÉņä£ ņłĀ ņĀäņŚÉ ļ╣äĒĢ┤ ņ£ĀņØśĒĢ£ ņĢłņĢĢĒĢśĻ░Ģ ļ░Å ņĢłņĢĮ Ļ░£ņłś Ļ░ÉņåīĻ░Ć ļéśĒāĆļé¼ņ£╝ļ®░, ļ░▒ļé┤ņןņłśņłĀ ļ│æĒĢ® ņ£Āļ¼┤ņŚÉ ļö░ļØ╝ ĻĄ░ņØä ļéśļłäņ¢┤ņä£, ņä▒Ļ│ĄļźĀņØä ļČäņäØĒĢśņśĆņØä ļĢī, ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖ ļŗ©ļÅģĻĄ░ņØś ņä▒Ļ│ĄļźĀņØĆ ņłĀ Ēøä 1Ļ░£ņøö, 3Ļ░£ņøö ļ░Å 6Ļ░£ņøöņŚÉ Ļ░üĻ░ü 71.3%, 58.9%, 33.7%, ļ░▒ļé┤ņןņłśņłĀ ļ│æĒĢ®ĻĄ░ņØĆ Ļ░üĻ░ü 73.4%, 59.8%, 42.7%ļĪ£ ļéśĒāĆļé¼ļŗż. ļśÉĒĢ£ ĒÖśņ×ÉņØś ļéśņØ┤Ļ░Ć ņĀŖņØäņłśļĪØ, ņłĀ Ēøä 6Ļ░£ņøöņ¦Ė ņä▒Ļ│ĄļźĀņØ┤ ļåÆņØĆ Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż.
ĻĄŁņÖĖņŚÉ ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņéĮņ×ģņłĀņØś ļŗ©ĻĖ░ ļ░Å ņןĻĖ░Ļ░ä ņłśņłĀ Ļ▓░Ļ│╝ ļ│┤Ļ│ĀļŖö ļ¦ÄņØ┤ ņ׳ļŗż[14-19]. Le and Saheb [14]ņØĆ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņéĮņ×ģņłĀņØś ņłśņłĀ Ļ▓░Ļ│╝ ļ│┤Ļ│ĀļōżņØä ņÜöņĢĮĒĢśņŚ¼ ļ░£Ēæ£ĒĢ£ ļģ╝ļ¼ĖņŚÉ ļö░ļź┤ļ®┤, ņłĀ Ēøä ņĢłņĢĢĒĢśĻ░ĢņØĆ 16-33%, ļģ╣ļé┤ņן ņĢĮļ¼╝ Ļ░ÉņåīļŖö 0.5-2Ļ░£ļź╝ ļ│┤ņśĆļŗż. ļśÉĒĢ£ Katz et al [15]ņØĆ ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖ ņéĮņ×ģ Ļ░£ņłśņŚÉ ļö░ļźĖ ņĢłņĢĢĒĢśĻ░ĢņØä ļ╣äĻĄÉĒĢśņśĆļŖöļŹ░, 42Ļ░£ ņøöĻ╣īņ¦Ć 1Ļ░£, 2Ļ░£, 3Ļ░£ ņéĮņ×ģĻĄ░ņŚÉņä£ Ļ░üĻ░ü 24%, 22%, 27%ņØś ņĢłņĢĢĒĢśĻ░ĢņØ┤ ļéśĒāĆļé¼ņ£╝ļ®░, 20% ņØ┤ņāüņØś ņĢłņĢĢĒĢśĻ░ĢņØä ļ│┤ņØ┤ļŖö ļ╣äņ£©ņØĆ Ļ░üĻ░ü 61%, 91%, 91%ļź╝ ļ│┤ņŚ¼ņä£, 2Ļ░£ ņØ┤ņāüņØś ņŖżĒģÉĒŖĖņéĮņ×ģņØ┤ ļŗ©ļÅģ ņéĮņ×ģņŚÉ ļ╣äĒĢ┤ ņĢłņĢĢĒĢśĻ░Ģ ĒÜ©Ļ│╝Ļ░Ć ļŹö ņóŗļŗżĻ│Ā ļ│┤Ļ│ĀĒĢśņśĆļŗż. ļ░▒ļé┤ņןņłśņłĀĻ│╝ ļ│æņÜ®ĒĢ£ ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņéĮņ×ģņłĀņØś ņłśņłĀ Ļ▓░Ļ│╝ ļ│┤Ļ│Āļź╝ ļ│┤ļ®┤[16-18], iStent injection Study Group ņŚ░ĻĄ¼ņŚÉņä£, ņłśņłĀ Ēøä 24Ļ░£ņøö ņĢłņĢĢĒĢśĻ░Ģ Ļ▓░Ļ│╝ņŚÉņä£, 5.4 mmHgņØś Ļ░Éņåīļź╝ ļ│┤ņØĖ ļ░▒ļé┤ņןņłśņłĀ ļŗ©ļÅģĻĄ░ņŚÉ ļ╣äĒĢśņŚ¼, 7.0 mmHgņØś Ļ░Éņåīļź╝ ļ│┤ņØĖ ļ░▒ļé┤ņןņłśņłĀĻ│╝ ļ│æņÜ®ĒĢ£ ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņéĮņ×ģņłĀ ņŗ£Ē¢ēĻĄ░ņØ┤ ņ£ĀņØśĒĢśĻ▓ī ļŹö Ēü░ ņĢłņĢĢĒĢśĻ░ĢņØä ļ│┤ņśĆļŗż[16]. ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ļÅä, ņłĀ ņĀäņŚÉ ļ╣äĒĢśņŚ¼ ņłĀ Ēøä 6Ļ░£ņøöņŚÉ ĒÅēĻĘĀ 27.7%ņØś ņĢłņĢĢĒĢśĻ░ĢņØä ļ│┤ņŚ¼ ĻĄŁņÖĖ ņŚ░ĻĄ¼ņÖĆ ņ£Āņé¼ĒĢ£ Ļ▓░Ļ│╝ļź╝ ļ│┤ņśĆņ£╝ļéś, ņĢłņĢĢ 20 mmHg ļ»Ėļ¦ī ļ░Å 20% ņØ┤ņāüņØś ņĢłņĢĢĒĢśĻ░ĢņØä ĻĖ░ņżĆņ£╝ļĪ£ ĒĢśļŖö ņłśņłĀ ņä▒Ļ│ĄļźĀņØĆ ņłĀ Ēøä 6Ļ░£ņøöņŚÉ 33.7%ļĪ£ ļŗżļźĖ ņŚ░ĻĄ¼ņŚÉ ļ╣äĒĢśņŚ¼ ļé«ņĢśļŗż.
ņØ┤ļ¤¼ĒĢ£ Ļ▓░Ļ│╝Ļ░Ć ļéśĒāĆļé£ ņØ┤ņ£ĀļĪ£, ņ▓½ņ¦ĖļŖö ļ│Ė ņŚ░ĻĄ¼ņŚÉ ņ░ĖņŚ¼ĒĢ£ ĒÖśņ×ÉņŚÉĻ▓ī ņŖżĒģÉĒŖĖļź╝ 1Ļ░£ļ¦ī ņéĮņ×ģĒĢśņŚ¼ņä£, ņŖżĒģÉĒŖĖļź╝ 2Ļ░£ ņéĮņ×ģĒĢ£ ļŗżļźĖ ņŚ░ĻĄ¼ņŚÉ ļ╣äĒĢ┤ ņłśņłĀ ņä▒Ļ│ĄļźĀņØ┤ ļé«ņØä ņłś ņ׳ļŗż. Johnstone [20]ņØĆ ņĢłņĢĢ ļ│ĆĒÖöņŚÉ ļö░ļźĖ ļ░®ņłś ņ£ĀņČ£ ņĪ░ņ¦üņØś ļ│Ćņä▒ņØä ņŗżĒŚśņĀüņ£╝ļĪ£ ļ│┤ņŚ¼ ņŻ╝ņŚłļŖöļŹ░, Katz et al [15]ņØĆ ņØ┤ļ¤¼ĒĢ£ ņĪ░ņ¦ü ļ│ĆĒÖöĻ░Ć ņŖżĒģÉĒŖĖņØś ņ×æņÜ®ņØä Ļ░Éņåīņŗ£ĒéżĻĖ░ ļĢīļ¼ĖņŚÉ, ņŖżĒģÉĒŖĖņØś Ļ░£ņłśĻ░Ć ļ¦ÄņØäņłśļĪØ ĒÜ©Ļ│╝ Ļ░Éņåīļź╝ ļ¦ēņØä ņłś ņ׳ņØä Ļ▓āņ£╝ļĪ£ ļ│┤Ļ│ĀĒĢśņśĆļŗż. ļŗżļźĖ ņØ┤ņ£ĀļĪ£ļŖö, ĒĢ£ĻĄŁņØĖņØ┤ ĒżĒĢ©ļÉ£ ļÅÖņĢäņŗ£ņĢäņØĖņØ┤ ņØ╝ļ░śņĀüņ£╝ļĪ£, ļŹö ņóüņØĆ ņĀäļ░®Ļ░üņØä Ļ░Ćņ¦ĆĻ│Ā ņ׳ņ¢┤ņä£, ĒÖŹņ▒ä ļō▒ņØś ĻĄ¼ņĪ░ļ¼╝ņŚÉ ņØśĒĢ┤ ņéĮņ×ģļÉ£ ņŖżĒģÉĒŖĖĻ░Ć ĒÅÉņćä ļ░Å ĻĖ░ļŖźņĀĆĒĢśĻ░Ć ņāØĻĖĖ ņłś ņ׳ņØä Ļ▓āņ£╝ļĪ£ ņÜ░ļĀżļÉ£ļŗż. ņŗżņĀ£ļĪ£, ņØ╝ļ│ĖņØĖņØä ļīĆņāüņ£╝ļĪ£ 2Ļ░£ņØś ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņéĮņ×ģņłĀ Ļ▓░Ļ│╝ ļ│┤Ļ│ĀņŚÉņä£, Shiba et al [19]ņØĆ 23.2%ņØś ņĢłņĢĢĒĢśĻ░Ģ ĒÜ©Ļ│╝ļź╝ ļ│┤Ļ│ĀĒĢśņŚ¼ņä£, 2Ļ░£ņØś ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖ ņéĮņ×ģ Ļ▓░Ļ│╝ļź╝ ļ│┤Ļ│ĀĒĢ£ ļŗżļźĖ ņÖĖĻĄŁ Ļ▓░Ļ│╝ļ│┤ļŗż ļé«Ļ▓ī ļéśĒāĆļé¼ļŗż. ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£, ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņéĮņ×ģņłĀņØä ļ░øņØĆ ļģ╣ļé┤ņן ĒÖśņ×ÉņØś ņżæļō▒ļÅä ļČäĒżļź╝ ļ│┤ļ®┤[21], ļ¦ÉĻĖ░(severe), ņżæĻĖ░(moderate), ņ┤łĻĖ░(early) ļģ╣ļé┤ņןņØĆ Ļ░üĻ░ü 66.7%, 6.1%, 27.3%ņØś ļČäĒż ļ╣äņ£©ņØä ļ│┤ņśĆļŗż. Ļ░£ļ░®Ļ░üļģ╣ļé┤ņןņŚÉņä£ ņä¼ņ£ĀņŻ╝Ļ░Ć ļ░®ņłśņ£ĀņČ£ļĪ£ņØś ņĀĆĒĢŁņä▒ņØä ņØ╝ņ£╝ĒéżļŖö ņØ╝ņ░©ņĀü ļČĆņ£äņØ┤Ļ│Ā[22], ļģ╣ļé┤ņן ņżæļō▒ļÅäĻ░Ć ļåÆņØäņłśļĪØ ņä¼ņ£ĀņŻ╝ ļ░®ņłś ņ£ĀņČ£ļĪ£ņØś ņĀĆĒĢŁņä▒ņØ┤ ļåÆļŗżļŖö Ļ▓āņØĆ ļ░®ņłś ņ£ĀņČ£ļĪ£ņØś ĻĖ░ļŖźņØä ņ”ØĻ░Ćņŗ£ĒéżĻĖ░ ņ£äĒĢ£ ņä¼ņ£ĀņŻ╝ņĀłĻ░£ņłĀ(trabeculetome)ņØś Ļ▓░Ļ│╝ļĪ£ ĒÖĢņØĖļÉśņŚłļŗż[23]. ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ ļ¦ÉĻĖ░ ļģ╣ļé┤ņן ĒÖśņ×ÉņØś ļ╣äņ£©ņØ┤ ļåÆĻ│Ā ņä¼ņ£ĀņŻ╝ ļ░®ņłśņ£ĀņČ£ļĪ£ņØś ņĀĆĒĢŁņä▒ņØ┤ ļåÆĻĖ░ ļĢīļ¼ĖņŚÉ ņłśņłĀ ņä▒Ļ│ĄļźĀņØ┤ ļé«ņØĆ ņøÉņØĖņØ┤ ļÉĀ ņłś ņ׳ņØä Ļ▓āņ£╝ļĪ£ ļ│┤ņØĖļŗż. ļśÉĒĢ£ ņłśņłĀ Ēøä 1Ļ░£ņøö, 3Ļ░£ņøö, 6Ļ░£ņøöņØ┤ ļÉĀņłśļĪØ ņĢłņĢĢņØ┤ ņĀÉņĀÉ ļŗżņŗ£ ņāüņŖ╣ĒĢśĻ│Ā ņłśņłĀ ņä▒Ļ│ĄļźĀņØ┤ ņĀÉņ░© ņżäņ¢┤ļō£ļŖö Ļ▓░Ļ│╝ļŖö ņĪ░ņ¦üĒĢÖņĀüņ£╝ļĪ£ ņŖżĒģÉĒŖĖ ļé┤Ļ░Ģ(lumen)ņØś ņä¼ņ£ĀĒÖöļĪ£ ņŖżĒģÉĒŖĖņØś ĻĖ░ļŖź Ļ░ÉņåīņÖĆ Ļ┤ĆļĀ©ņØ┤ ņ׳ņØä Ļ▓āņ£╝ļĪ£ ļ│┤ņØĖļŗż[24].
ļ│Ė ņŚ░ĻĄ¼ļŖö ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņéĮņ×ģņłĀņØś ņä▒Ļ│ĄņŚÉ ņśüĒ¢źņØä ļ»Ėņ╣śļŖö ņłĀ ņĀä ņØĖņ×ÉņŚÉ ļīĆĒĢ£ ļČäņäØļÅä Ļ░ÖņØ┤ ĒĢśņśĆļŖöļŹ░, ĻĘĖ Ļ▓░Ļ│╝ ļéśņØ┤Ļ░Ć ņĀŖņØäņłśļĪØ ņłśņłĀ ņä▒Ļ│ĄļźĀņØ┤ ļåÆņĢäņ¦ĆļŖö Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż. ņØ┤ļŖö ņĪ░ņ¦üĒĢÖņĀüņ£╝ļĪ£, ņŖżĒģÉĒŖĖļź╝ ĒåĄĒĢ£ ļ░®ņłśņ£ĀņČ£ņØ┤ ņē┤ļĀśĻ┤Ć ļ░öĻ╣źņ¬ĮņŚÉ ņĪ┤ņ×¼ĒĢśļŖö ņŗ¼ļČĆ Ļ│Ąļ¦ē ņ¢╝ĻĖ░(deep scleral plexus) ļé┤ņØś ņ¦æĒĢ®Ļ┤ĆņØä ĒåĄĒĢ┤, ņāüĻ│Ąļ¦ēņĀĢļ¦ź ļśÉļŖö ļ░®ņłśņĀĢļ¦źņ£╝ļĪ£ ļ╣ĀņĀĖļéśĻ░ĆļŖö Ļ│╝ņĀĢņŚÉņä£, ļéśņØ┤Ļ░Ć ļōżņłśļĪØ, ņäĖĒż ĻĖ░ņĀĆļ¦ēņØś ļæÉĻ╗ś ņ”ØĻ░ĆļĪ£ ņØĖĒĢ£ ņ£ĀņČ£ļĪ£ņØś ņĀĆĒĢŁņä▒ņØ┤ ņ”ØĻ░ĆļÉśņ¢┤ņä£, ņŖżĒģÉĒŖĖņéĮņ×ģņłĀņØ┤ ņĀüņĀłĒ׳ ņŗ£Ē¢ēļÉśņ¢┤ļÅä, ņĢłņĢĢĒĢśĻ░ĢņØ┤ ņĀüĻ▓ī ņØ╝ņ¢┤ļéĀ ņłś ņ׳ļŗż[25,26].
ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£, ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņéĮņ×ģņłĀ ņŗ£Ē¢ē Ēøä, ĒĢ®ļ│æņ”ØņØĆ ļ│┤Ļ│ĀļÉśņ¦Ć ņĢŖņĢśļŗż. ĻĘĖļ”¼Ļ│Ā, ĒåĄĻ│äņĀüņ£╝ļĪ£ ņ£ĀņØśĒĢśņ¦Ć ņĢŖņĢśņ£╝ļéś, ļ░▒ļé┤ņןņłśņłĀĻ│╝ ļ│æņÜ®ĒĢ£ Ļ▓ĮņÜ░ņŚÉ ļŹö ļåÆņØĆ ņłśņłĀ ņä▒Ļ│ĄļźĀņØä ļ│┤ņśĆļŗż. Ēæ£ņżĆ ņłśņłĀļĪ£ ņĢīļĀżņĀĖ ņ׳ļŖö ņä¼ņ£ĀņŻ╝ņĀłņĀ£ņłĀņØś Ļ▓ĮņÜ░, ĒÜ©Ļ│╝ņĀüņØĖ ņĢłņĢĢĒĢśĻ░Ģ ĒÜ©Ļ│╝ļź╝ ļ│┤ņŚ¼ņŻ╝ļŖö ņłśņłĀņØ┤ņ¦Ćļ¦ī, ļ░▒ļé┤ņןņłśņłĀĻ│╝ ļ│æņÜ®ĒĢśļŖö Ļ▓ĮņÜ░ņŚÉ ļŹö ļ¦ÄņØĆ ĒĢ®ļ│æņ”ØņØ┤ ļéśĒāĆļéśļ®░, ņłśņłĀ Ēøä ņŗ£ļĀź ĒÜīļ│Ą ņŗ£Ļ░ä ļśÉĒĢ£ ņ¦ĆņŚ░ļÉ£ļŗżļŖö ļ│┤Ļ│ĀĻ░Ć ņ׳ļŗż[27-29]. Vlasov and Kim [30]ņØĆ ņä¼ņ£ĀņŻ╝ņĀłņĀ£ņłĀņŚÉ ļ╣äĒĢ┤ ņĢłņĀäĒĢśĻ│Ā, ĒĢ®ļ│æņ”ØņØ┤ Ļ▒░ņØś ņŚåļŖö ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņéĮņ×ģņłĀņØ┤ ĒÖ£ļÅÖņØ┤ ĒÖ£ļ░£ĒĢ£ ņĀŖņØĆ ĒÖśņ×ÉņŚÉĻ▓ī ņ£ĀņÜ®ĒĢĀ Ļ▓āņ£╝ļĪ£ ĻĖ░ļīĆļÉ£ļŗżĻ│Ā ņĀ£ņĢłĒĢśņśĆļŗż. ļö░ļØ╝ņä£, ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ ļ│┤Ļ│ĀĒĢ£ ņĀŖņØĆ ĒÖśņ×ÉņŚÉņä£ ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņéĮņ×ģņłĀņØ┤ ĒÜ©Ļ│╝Ļ░Ć ņ׳ļŗżļŖö Ļ▓░Ļ│╝ņÖĆ ņØ╝ņ╣śĒĢ£ļŗżĻ│Ā ļ│╝ ņłś ņ׳ļŗż.
ņØ┤ļ▓ł ņŚ░ĻĄ¼ ņĀ£ĒĢ£ņĀÉņØĆ ļīĆņāüņ×ÉņØś ņłśĻ░Ć 33ļ¬ģņ£╝ļĪ£ ņĀüņŚłĻ│Ā, ĒøäĒ¢źņĀüņ£╝ļĪ£ ņØśļ¼┤ĻĖ░ļĪØņØä ļČäņäØĒĢ£ Ļ▓░Ļ│╝ņØ┤ļ®░, ņłśņłĀ Ēøä 6Ļ░£ņøöņØś ņ¦¦ņØĆ Ļ▓ĮĻ│╝ Ļ┤Ćņ░░ĻĖ░Ļ░äņØś ņŚ░ĻĄ¼ņśĆļŗżļŖö ņĀÉņØ┤ļŗż. ļśÉĒĢ£, ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖ ļŗ©ļÅģ ņéĮņ×ģņłĀ ņŗ£Ē¢ēĒĢ£ ĻĄ░ņØ┤ ļ░▒ļé┤ņןņłśņłĀ ļ│æĒĢ®ĻĄ░ ļ░Å ļīĆņĪ░ĻĄ░Ļ│╝ ņ£ĀņØśĒĢ£ ņłĀ ņĀä ņĢłņĢĢ ļ░Å ļéśņØ┤ ņ░©ņØ┤Ļ░Ć ļéśĒāĆļéśņä£, ņØ┤ļĪ£ ņØĖĒĢ£ ņäĀĒāØ ļ░öņØ┤ņĢäņŖż(selection bias)ļź╝ ļ░░ņĀ£ĒĢĀ ņłś ņŚåļŖö ĒĢ£Ļ│äņĀÉņØ┤ ņ׳ļŗż. ļ│Ė ņŚ░ĻĄ¼ļŖö ņØ╝ņ░©ņĀüņ£╝ļĪ£ ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņłśņłĀņØ┤ ņłĀ ņĀäņŚÉ ļ╣äĒĢ┤ ņ£ĀņØśĒĢ£ ņĢłņĢĢĒĢśĻ░ĢņØä ļ│┤ņŚ¼ņŻ╝ļŖöĻ░Ćļź╝ ļČäņäØĒĢśĻ│Āņ×É ĒĢśņśĆĻĖ░ ļĢīļ¼ĖņŚÉ, ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņłśņłĀņØĆ ņĢłņĢĢĒĢśĻ░ĢņØä ņØ╝ņ░© ļ¬®ņĀüņ£╝ļĪ£ ĒĢśļŖö ļ░▒ļé┤ņןņłśņłĀņØ┤ ĒĢäņÜö ņŚåļŖö ĒÖśņ×ÉĻ░Ć ĒżĒĢ©ļÉśņ¢┤ņä£, ļ░▒ļé┤ņןņłśņłĀņØä ņŗ£Ē¢ēĒĢ£ ļ░▒ļé┤ņןņłśņłĀ ļ│æĒĢ®ĻĄ░Ļ│╝ ļīĆņĪ░ĻĄ░ņŚÉ ļ╣äĒĢ┤, ļåÆņØĆ ņłĀ ņĀä ņĢłņĢĢ ļ░Å ņĀŖņØĆ ļéśņØ┤ļź╝ ļ│┤ņØ┤ļŖö Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé£ ĒĢ£Ļ│äņĀÉņØ┤ ņ׳ņ£╝ļ®░, ņČöĒøä ņłĀ ņĀä ņĢłņĢĢ ļ░Å ļéśņØ┤ņØś ņ░©ņØ┤Ļ░Ć ņŚåļŖö ļīĆņĪ░ĻĄ░Ļ│╝ņØś ņןĻĖ░ņĀüņØĖ ļ╣äĻĄÉ ļČäņäØņØä ĒĢśļŖö ņĀäĒ¢źņĀüņØĖ ņŚ░ĻĄ¼Ļ░Ć ĒĢäņÜöĒĢĀ Ļ▓āņ£╝ļĪ£ ņé¼ļŻīļÉ£ļŗż. Ļ▓īļŗżĻ░Ć, ļ│Ė ņŚ░ĻĄ¼ļŖö ļ░▒ļé┤ņןņłśņłĀ ļÅÖļ░ś ļ░Å ņéĮņ×ģņłĀ ļŗ©ļÅģņØä Ļ░ÖņØ┤ ĒżĒĢ©ĒĢśņŚ¼ ņŚ░ĻĄ¼ ļČäņäØņØä ņŗ£Ē¢ēĒĢśņśĆņ£╝ļ»ĆļĪ£ ļ░▒ļé┤ņןņłśņłĀ ĒÜ©Ļ│╝Ļ░Ć ļ│Ė ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ņŚÉ ņśüĒ¢źņØä ļ»Ėņ╣Ā ņłś ņ׳ļŗż. ĒĢśņ¦Ćļ¦ī, ļīĆņāü ņłśļŖö ņĀüņ£╝ļéś, ļ░▒ļé┤ņןņłśņłĀ ļ│æĒĢ®ĻĄ░Ļ│╝ ļīĆņĪ░ĻĄ░Ļ│╝ņØś ņłĀ Ēøä ņĢłņĢĢĒĢśĻ░Ģ ļ░Å ņĢĮļ¼╝ Ļ░£ņłś ļ│ĆĒÖöļź╝ ļ╣äĻĄÉ ļČäņäØĒĢśņŚ¼ņä£, ļīĆņĪ░ĻĄ░Ļ│╝ ļŗ¼ļ”¼, ļ░▒ļé┤ņןņłśņłĀ ļ│æĒĢ®ĻĄ░ņŚÉņä£, ņ£ĀņØśĒĢ£ ņĢĮļ¼╝ Ļ░£ņłś Ļ░ÉņåīĻ░Ć ļéśĒāĆļé¼ļŗż. ņØ┤ņÖĆ ĒĢ©Ļ╗ś ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ļŖö 2ļ¬ģņØś ņłśņłĀņ×ÉņŚÉ ņØśĒĢ┤ ņŗ£Ē¢ēļÉ£ Ļ▓░Ļ│╝ļź╝ ļČäņäØĒĢ£ ņŚ░ĻĄ¼ļĪ£ņä£, ņłśņłĀņ×É ņÜöņåīņØś ņśüĒ¢źņØ┤ ņ׳ņØä ņłś ņ׳ņ£╝ļéś ļ╣äĻĄÉņĀü Ēæ£ņżĆĒÖöļÉ£ ņłśņłĀļĪ£ Ļ▓░Ļ│╝ņŚÉ ņżæļīĆĒĢ£ ņśüĒ¢źņØä ļ»Ėņ╣śņ¦Ć ņĢŖņĢśņØä Ļ▓āņØ┤ļØ╝ ņāØĻ░üļÉśņ¦Ćļ¦ī ļ│Ė ņŚ░ĻĄ¼ņØś ņĀ£ĒĢ£ņĀÉņØ┤ļØ╝Ļ│Ā ĒĢĀ ņłś ņ׳ļŗż. Ļ▓░ļĪĀņĀüņ£╝ļĪ£ ĒĢ£ĻĄŁņØĖņŚÉņä£ ņä¼ņ£ĀņŻ╝ ļ»ĖņäĖņÜ░ĒÜī ņŖżĒģÉĒŖĖņéĮņ×ģņłĀņØĆ ņ£ĀņØśĒĢ£ ņĢłņĢĢĒĢśĻ░ĢņØ┤ ļéśĒāĆļé¼ņ£╝ļ®░, ĒŖ╣Ē׳ ņĀŖņØĆ ĒÖśņ×ÉņŚÉņä£, ļŹö ņóŗņØĆ ņłśņłĀ ņä▒Ļ│ĄļźĀņØä ļ│┤ņØ┤ļŖö Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






