인공수정체 공막고정술에서 공막누르기를 이용한 주변부 유리체절제술의 효과
The Utility of Peripheral Vitrectomy Featuring Scleral Indentation during Scleral Fixation of Intraocular Lenses
Article information
Abstract
목적
인공수정체 탈구 환자에서 인공수정체 공막고정술과 함께 유리체절제술을 시행할 때 공막누르기를 이용한 주변부 유리체절제술을 시행한 군의 수술 성적을 대조군과 비교하여 공막누르기를 이용한 주변부 유리체절제술의 효과를 확인해보고자 한다.
대상과 방법
2018년 1월부터 2020년 12월까지 전체 유리체절제술, 인공수정체 제거술, 인공수정체 공막고정술을 시행받은 인공수정체 탈구 환자 20안을 대상으로 하였으며, 이 중 10안에서는 공막누르기를 통한 주변부 유리체절제술을 추가 시행하였다. 수술은 1명의 술자에 의해 진행되었으며 6개월 미만의 추적 관찰 기간, 망막 및 녹내장수술의 과거력, 시력에 중대한 영향을 미치는 망막이상 및 녹내장 환자는 제외하였다. 수술 후 최대교정시력, 안압, 난시 변화, 수술 후 합병증을 의무기록지를 바탕으로 후향적으로 분석하였다.
결과
수술 6개월 후 공막누르기를 이용한 주변부 유리체절제술을 시행한 군에서 최대교정시력은 0.95(스넬렌), 대조군에서 0.60이었으며(p=0.029), 전체난시굴절량은 공막누르기를 이용한 주변부 유리체절제술을 시행한 군에서 0.48디옵터, 대조군에서는 2.80디옵터로 통계적으로 유의한 차이를 보였다(p<0.001).
결론
인공수정체 탈구 환자에서 인공수정체 공막고정술과 함께 유리체절제술을 시행하는 경우, 공막누르기를 이용한 주변부 유리체절제술을 시행하는 것이 시력 개선 효과를 더욱 증진시킬 수 있을 것으로 보이며, 이는 주변부 유리체를 최대한 제거함으로써 잔존 유리체에 의해 발생할 수 있는 인공수정체 위치 불안정화 감소에 의한 것으로 생각된다.
Trans Abstract
Purpose
We evaluated the utility of peripheral vitrectomy featuring scleral indentation; we compared a group who underwent peripheral vitrectomy to a control group for whom vitrectomy was combined with scleral fixation of intraocular lenses (IOLs) in patients exhibiting IOL dislocations.
Methods
From January 2018 to December 2020, 20 eyes of patients evidencing IOL dislocations that underwent total vitrectomy, IOL removal, and IOL scleral fixation were evaluated; peripheral vitrectomy with scleral indentation was performed in 10 patients. All operations were performed by the same surgeon. We excluded patients with follow-up periods less than 6 months, those with a history of retinal and/or glaucoma surgery, and patients with retinal abnormalities or glaucoma that might significantly compromise visual acuity. The postoperative best-corrected visual acuity, intraocular pressure, astigmatism changes, and complications were retrieved from the medical records.
Results
Six months after surgery, the best corrected visual acuity was 0.95 (the Snellen measure) in the group who underwent peripheral vitrectomy featuring scleral indentation, and 0.60 in the control group (p = 0.029). The total astigmatism values were 0.48 diopter in the former and 2.80 diopter in the latter group; the difference was significant (p < 0.001).
Conclusions
In patients with IOL dislocations who underwent vitrectomy combined with IOL scleral fixation, improvements in visual acuity were further enhanced when peripheral vitrectomy was combined with scleral indentation. Complete removal of the peripheral vitreous may stabilize IOL positioning by the remnant vitreous.
백내장수술은 많이 시행되는 안과수술 중 하나로, 수정체유화술 및 인공수정체삽입술이 가장 많이 시행되고 있다[1]. 백내장수술 후 나타날 수 있는 합병증으로는 망막박리, 인공수정체 탈구, 안내염, 상처 벌어짐, 각막부종, 낭포성 황반부종 등이 있고[2,3], 이 중 인공수정체 탈구는 0.2-3.0%의 발병률을 가지는 것으로 보고된다[4]. Pueringer et al [5]에 따르면 백내장수술 후 5년마다 인공수정체 탈구가 발생할 누적 위험률이 0.1%, 0.1%, 0.2%, 0.7%로 증가한다고 하였으며, 그리고 술 후 25년 뒤에는 1.7% 정도 인공수정체 탈구 누적 위험률이 있다고 보고하였다.
섬모체소대의 약화 등의 요인으로 인해 후낭의 지지가 약해질 경우, 인공수정체의 위치가 적절히 유지될 수 없어 인공수정체 탈구로 인한 시력저하가 발생될 수 있고 이를 해소하기 위해 여러 수술 방법이 소개되었으며, 이 중 평면부 유리체절제술과 인공수정체 공막고정술 동시 시행이 가장 많이 이용되고 있다[3]. 지금까지 평면부 유리체절제술 및 인공수정체 공막고정술과 관련하여 많은 연구가 보고되었으나, 저자들이 PubMed® (https://pubmed.ncbi.nlm.nih.gov)를 통하여 Scleral fixation, Transscleral fixation, Pars plana vitrectomy, Peripheral vitrectomy, Scleral indentation을 검색어로 하여 문헌을 검색하였으나, 공막누르기를 이용한 주변부 유리체절제술을 시행한 경우 인공수정체 공막고정술의 임상적 효과에 대한 연구는 검색되지 않았다. 이에 본 저자들은 인공수정체 탈구 환자에서 평면부 유리체절제술과 인공수정체 공막고정술을 동시에 하는 경우 공막누르기를 이용한 주변부 유리체절제술의 임상적 효과를 확인해보고자 하였다.
대상과 방법
2018년 1월부터 2020년 12월까지 경상국립대학교 병원에 내원한 인공수정체 탈구 환자 중 전체 유리체절제술, 인공수정체 제거술 및 인공수정체 공막고정술을 받은 환자 20명, 20안의 의무기록을 후향적으로 분석하였다. 본 연구는 후향적으로 의무기록을 분석한 피험자 동의 면제 연구로, 경상국립대학교 병원 생명의학연구윤리 심의위원회의 승인을 받았으며(승인 번호: GNUH 2022-01-005), 모든 연구 과정에서 헬싱키선언을 준수하였다. 수술은 1명의 술자(WSY)에 의해 진행하였으며 20안 모두에서 전체 유리체절제술을 시행하였고, 10안에서는 공막누르기를 이용한 주변부 유리체절제술을 추가로 시행하였으며, 공막누르기를 사용하지 않은 10안을 대조군으로 설정하였다. 공막누르기를 이용한 주변부 유리체절제술은 주변부 망막의 열공 및 찢김, 격자성 변성이 발견되는 경우, 유리체 전방 탈출로 인한 동공 모양 이상이 발생 관찰되는 경우 술자의 판단에 의해 시행하였으며, 모든 환자에서 사용한 인공수정체는 동일한 3피스 인공수정체 모델(AcrySof MA60®; Alcon, Fort Worth, TX, USA)을 사용하였다. 유리체절제술 시 유리체수술 장치는 Constellation® (Alcon)를 사용하였으며, 25게이지 유리체절제침을 사용하였다. 공막누르기를 이용한 주변부 유리체절제술 시 유리체절제침의 흡입압은 550 mmHg, 절제속도는 7,500 cpm으로 설정하였다. 수술 시 보조자 1인과 함께 시행하였으며, 눈속관찰시스템은 비접촉형 광각관찰시스템(Resight® 700 Fundus Viewing System; Carl Zeiss AG, Oberkochen, Germany)을 사용하였다. 수술받은 환자 중 6개월 미만의 추적 관찰 기간, 안축장이 26 mm 이상인 경우, 망막 및 녹내장수술의 과거력, 시력에 중대한 영향을 미치는 망막이상 및 녹내장 환자는 제외하였다.
수술은 다음과 같이 시행하였다. 25게이지 3개 삽입관을 평면부에 삽입 후 전체 유리체절제술을 시행하였으며, 모든 환자에서 잔존된 수정체낭이 있는 경우 망막집게로 제거하였다. 탈구된 인공수정체는 망막집게로 잡은 후, 12시 방향 각막윤부에 6 mm 절개를 하여 탈구된 인공수정체를 제거하였다. 환자 중 주변부 유리체절제술 시행하는 경우 공막누르기를 통해 홍채 뒤나 망막톱니둘레 앞까지 유리체절제술을 추가로 시행하였다. 이후 4, 10시 방향 각막윤부로부터 2 mm 떨어진 곳에 결막을 절개하여 공막을 노출시킨 후 양쪽 끝에 바늘이 달린 Straight double-armed 10-0 polypropylene (PROLENE®; Ethicon, Raritan, NJ, USA)을 4시 방향에서 통과시켜 후방으로 지나가게 하였다. 반대편에서 26게이지 주사침을 삽입하여 4시 방향에 삽입된 주사침이 26 G 주사침을 통해 10시 방향으로 나오게 하였다. 홍채갈고리로 후방을 관통하고 있는 봉합사를 각막 절개창으로 꺼내어 중간 부분을 자른 후, 각각을 인공수정체지지부의 끝에서 2 mm 지점에 봉합사를 고정시킨 뒤 인공수정체를 후방에 삽입하였다. 각막윤부 절개창을 10-0 monofilament black nylon (Alcon) 봉합한 후 양측의 봉합사를 조절하여 인공수정체 광학부를 중앙에 오도록 조정한 뒤 주사침을 삽입한 공막 위치에 직침을 구부려 공막 두께의 약 1/3 정도의 공막 부분층 봉합을 시행하고 봉합사는 결막 아래에 묻은 후 결막 봉합을 시행하였다. 이후 25 G 삽입관을 제거하였으며 누출이 있는 경우 흡수성 봉합사인 8-0 polyglactin (VICRYL®; Ethicon)을 이용하여 공막창 봉합을 시행하였다. 수술 후 1주간 moxifloxacin 점안액(Moroxacin®; Hanmi Pharm, Seoul, Korea)과 1% prednisolone acetate 점안액(Prednilone®; Daewoo Pharm, Seoul, Korea)을 1일 4회 사용하였으며, 수술 후 1-2주 이내에 각막윤부 절개 봉합사는 모두 제거하였다.
인공수정체 공막고정술은 술 후 근시성 변화가 나타날 수 있어[6,7] SRK/T 공식을 토대로 정시에 가깝게 도수를 결정하였다. 모든 환자에서 술 전 최대교정시력, 골드만평편안압, 각막곡률(Pentacam®; Oculus Inc., Arlington, WA, USA), 안축장(Aviso®; Quantel Medical, Rockwall, TX, USA)을 측정하였고, 전체난시와 각막난시는 자동굴절각막곡률측정기(KR-8900®; Topcon, Tokyo, Japan)로 측정하였다. 또한 파장가변 빛간섭단층촬영계(Triton®, Topcon)를 이용하여 central subfield thickness를 중심황반두께로 정의하여 측정하였다. 술 후 1, 6개월째 최대교정시력, 골드만 평편안압, 중심황반두께, 전체난시, 각막난시를 술 전과 같은 방법으로 측정하여 공막누르기를 이용한 주변부 유리체절제술을 시행한 군과 대조군을 비교하였다. 최대교정시력은 자동굴절각막곡률측정기와 조절마비굴절검사를 이용하여 교정한 시력 중 가장 좋은 시력으로 정의하였다.
통계 분석은 SPSS ver. 21.0 for windows® (SPSS Inc., Chicago, IL, USA)를 이용하였다. 두 군 간의 비교는 명목 척도인 경우 chi-square 검증을 이용하였으며, 연속변수는 비모수 검정인 Mann-Whitney U 검정을 시행하였으며, 중간값과 1분위 및 3분위값으로 본문과 표에 표기하였다. 또한 p값이 0.05 미만인 경우를 통계학적으로 유의하다고 판정하였다.
결 과
전체 수술 대상자는 총 20명, 20안으로 공막누르기를 이용한 주변부 유리체절제술을 시행한 군과 대조군 각각 10명이었다. 인구학적 특성인 성별, 나이, 인공수정체 탈구 원인에 있어서 두 군의 의미 있는 차이가 없었으며, 인공수정체 탈구의 형태 중 수정체낭을 포함한 탈구(in the bag dislocation)는 각각 3안이었다. 술 전 측정한 스넬렌 최대교정시력(0.1, 0.1), 안압(18.0 mmHg, 15.0 mmHg), 중심황반두께(282.5 µm, 289.0 µm)도 통계적으로 의미가 있는 차이를 보이지 않았다(Table 1, Fig. 1).
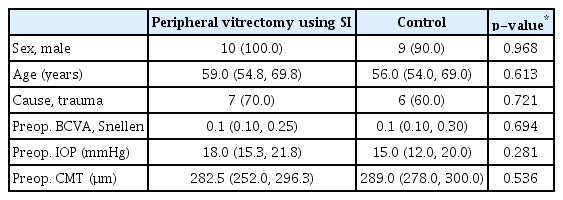
Demographics and clinical characteristics of peripheral vitrectomy group using scleral indentation and control group
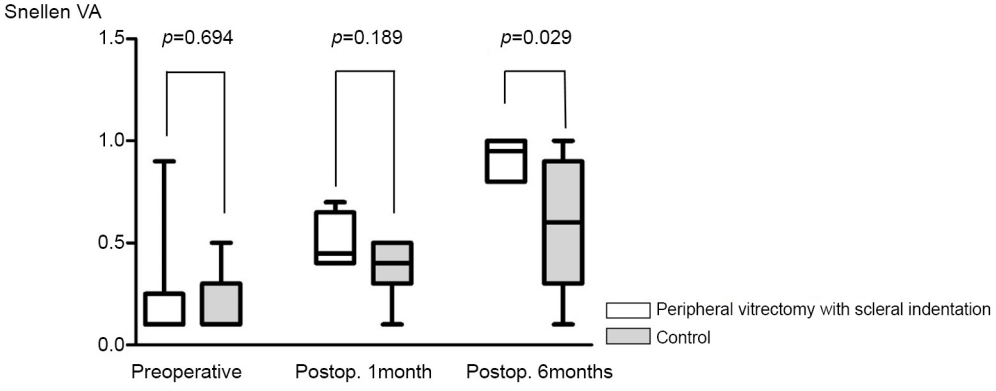
Comparison of BCVA of peripheral vitrectomy using scleral indentation and control group at preoperative, postoperative 1 month and 6 months. BCVA at preoperative and postoperative 1 month was has no difference between group, and has statistically difference between group at postoperative 6 months. VA = visual acuity; Postop. = postoperative; BCVA = best-corrected visual acuity.
또한 술 전 측정한 안구계측량을 비교하였을 때 전체난시(0.63디옵터[diopter, D], 1.25 D), 각막곡률(44.2 D, 44.1 D), 각막난시(0.80 D, 0.80 D), 안축장(23.75 mm, 24.49 mm) 및 목표 구면렌즈대응치(-0.01 D, -0.11 D) 모두 두 군에서 의미 있는 차이를 보이지 않았다(Table 2, Fig. 2).
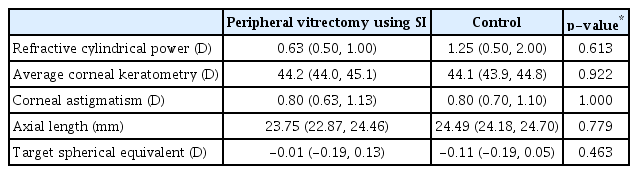
Preoperative characteristics of peripheral vitrectomy group using scleral indentation and control group

Comparison of refractive cylindrical power in peripheral vitrectomy using scleral indentation and control group at preoperative, postoperative 1 month and 6 months. Total amount of astigmatism at preoperative and postoperative 1 month was has no difference between group, and has statistically difference between group at postoperative 6 months. Postop. = postoperative.
술 후 6개월째, 주변부 유리체절제술을 시행한 군에서 최대교정시력은 0.95로 시행하지 않은 군의 0.60에 비해 통계적으로 의미 있는 차이를 보였으며(p=0.039), 각막난시는 각각 0.90 D, 0.80 D로 차이를 보이지 않았으나(p=0.520), 전체난시는 공막누르기를 이용하여 주변부 유리체절제술 시행한 군에서 0.48 D로 대조군의 2.80 D에 비해 낮게 나타났다(p<0.001) (Table 3, Fig. 1, 2).
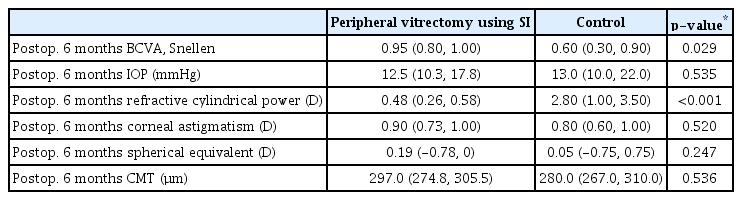
Clinical characteristics of peripheral vitrectomy group using scleral indentation and control group at postoperative 6 months
술 후 발생한 합병증으로는 두 군에서 낭포황반부종이 각 각 1안에서 발생하였으나 국소 Bromofenac 점안제(Bronuck®, Taejoon Pharm, Seoul, Korea) 사용 후 호전되었으며 대조군 2안에서 인공수정체의 동공물림이 발생하여 재위치술을 시행하였고, 그중 1안에서 동공물림이 반복 재발하여 동공성형술을 추가로 시행하였다(Table 4, Fig. 3).
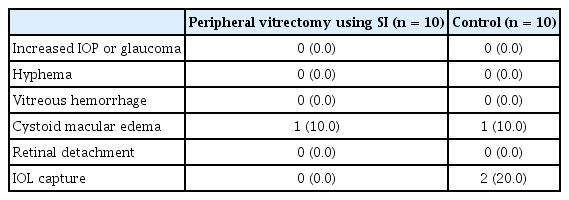
Complications of surgery in peripheral vitrectomy using scleral indentation and control group

Anterior segment photography of representative case with IOL pupil capture. (A) Pupillary capture of IOL was shown. (B) Pupilloplasty and IOL reposition was performed. IOL = intraocular lens.
고 찰
백내장수술 후 발생한 인공수정체 탈구는 흔하지는 않으나 시력에 큰 영향을 끼칠 수 있는 백내장수술 후 합병증 중의 하나로, 주요 원인으로 초기에는 수술 중 발생한 섬모체소대의 파괴에 의한 조기 탈구와 거짓비늘증후군 환자 등에서 발생하는 후기 탈구로 나눌 수 있으며, 일부 연구에서 고도근시가 인공수정체 탈구의 위험인자로 보고되고 있다[4,8]. 인공수정체 탈구의 수술적 치료에는 평면부 유리체절제술과 함께 인공수정체 공막고정술, 인공수정체 홍채고정술, 전방 인공수정체 삽입술을 이용하는 방법이 있고[9-11], 그 중 공막고정술은 상대적으로 안전한 술기, 적은 합병증으로 이용되는 술기로 특히 각막병변, 홍채손상, 녹내장이나 전방각의 이상이 있는 환자에서 효과적이다[12-14]. 평면부 유리체절제술과 인공수정체 공막고정술 후 시력 회복에 효과적이라고 보고되고 있으며[15] 본 연구에서는 평면부 유리체절제술과 인공수정체 공막고정술을 동시 시행 시 공막누르기를 이용한 주변부 유리체절제술의 임상적 결과를 대조군과 비교해보았다. 저자들의 연구 결과에서 술 후 6개월에 각막난시의 변화는 두 군 간의 차이가 없었으나 전체난시가 공막누르기를 이용한 주변부 유리체절제술을 한 경우 더 적게 나타나고 더불어 더 나은 시력 개선 효과가 있음을 확인하였다. 인공수정체 공막고정술 후 발생하는 난시는 각막, 인공수정체, 망막의 이상에 의해 발생할 수 있으며, 특히 수술 전후 인공수정체의 중심 이탈이나 기울어짐 등이 그 요인으로 생각해볼 수 있다[16]. Ma et al [17]은 공막 절편을 통한 인공수정체 공막고정술 후 각막난시가 증가함을 보고한 바 있는데, 본 연구에서의 공막누르기를 이용한 주변부 유리체절제술을 시행한 군과 대조군 모두 각막난시가 다소 증가하였으나, 두 군을 비교 시 수술 전, 수술 6개월째 각막난시는 통계적으로 의미 있는 차이를 보이지는 않았다. 하지만 전체난시는 공막누르기를 이용한 주변부 유리체절제술을 시행한 군에서 의미 있게 적게 나타났고, 이는 주변부 유리체를 제거함으로써 인공수정체 위치의 불안정화를 일으킬 수 있는 요인을 줄여 인공수정체의 기울임 혹은 회전이 적어짐에 따른 난시를 감소시켜 시력 개선에 도움이 되었을 것으로 예상된다. Toklu et al [18]은 유리체절제술 시 유리체기저의 유리체절제술을 시행한 경우와 그렇지 않은 경우에 전안부 계측을 비교하였는데, 연구에서 불완전한 유리체기저부 유리체의 제거가 오히려 수정체-홍채 가로막의 후방이동을 막아주고 이로 인해 전반의 계측치의 안정화를 이룬다고 보고하였다. 하지만 본 연구와는 달리 인공수정체 공막고정술이 아닌 수정체유화술의 경우에서 연구가 이루어졌으며, 본 연구에서는 잔존하는 수정체낭을 수술 시 전부 제거함으로써 인공수정체의 위치에 영향을 주는 것으로 수정체-홍채 가로막의 역할보다는 주변부 유리체의 역할이 더 중요할 것이라 생각된다.
인공수정체 공막고정술은 안압상승, 유리체출혈, 낭포황반부종, 인공수정체의 동공물림 등의 합병증이 발생하는 것으로 알려져 있다[9,10]. 본 연구에서의 두 군 모두 1명씩의 낭포황반부종이 생겼으나 약물 치료로 모두 호전되었으며, 대조군 환자 2명에서 인공수정체 동공물림 현상이 발생하였고, 그중 1안은 인공수정체 재위치술 후에도 반복적인 재발이 발생하여 동공성형술을 시행하여 동공물림을 치료하였다. 이와 같은 동공물림 역시 제거되지 않은 주변부 유리체로 인한 인공수정체의 위치 불안정화로 인한 회전 및 기울어짐이 하나의 요인으로 유추할 수 있으며, 따라서 공막 누르기를 이용한 주변부 유리체절제술이 인공수정체 위치 안정화의 효과적인 방법으로 생각해 볼 수 있을 것이다.
본 연구의 제한점으로는 첫째, 적은 수의 연구 대상자로 인한 통계적 오류 가능성과 상대적으로 짧은 추적 관찰 기간으로 장기간의 효과를 반영하지 않았다는 점, 둘째, 1인 수술자에 의한 수술 방법에 선택에 있어 선택 편견이 개입할 가능성이 있다는 점, 셋째, 후향적 연구로 인한 혼합 변수의 제어가 부족한 점이 있이 있다, 추후 다수의 환자를 대상으로 한 전향적인 연구를 통한 효과 확인이 필요할 것으로 생각되며, 공막누르기를 이용한 주변부 유리체의 제거가 전방에 미치는 영향에 대한 계측을 통해 실제 인공수정체의 위치의 변화를 수치화하여 확인하는 것이 필요하다. 그리고 공막누르기를 이용한 주변부 유리체절제술 시 발생할 수 있는 망막열공 및 섬모체손상 등의 합병증에 대한 가능성도 고려하여 위험-이득에 대한 철저한 고찰도 필요할 것이다. 하지만 이러한 제한점에도 본 연구는 기존에 보고되지 않은 인공수정체 탈구 환자에서 유리체절제술과 인공수정체 공막고정술에서 공막누르기를 이용한 주변부 유리체절제술의 효과를 확인한 연구로 의의를 가질 수 있다고 생각된다.
결론적으로 인공수정체 탈구 환자에서 유리체절제술과 인공수정체 공막고정술은 안전하고 효과적인 시력 개선 효과를 나타내며, 더불어 공막누르기를 이용한 주변부 유리체절제술을 시행할 경우 인공수정체의 위치 안정화를 통한 난시 개선과 합병증 발생을 낮춰 줌으로써 술 후 시력 개선에 효과적인 방법의 하나가 될 수 있을 것으로 생각된다.
Notes
Conflicts of Interest
The authors have no conflicts to disclose.
References
Biography
이동우 / Dong Woo Lee
경상국립대학교 의과대학 안과학교실
Department of Ophthalmology, Gyeongsang National University College of Medicine
