소아에서 발생한 특발성 시신경교차염
Idiopathic Chiasmal Optic Neuritis in a Pediatric Patient
Article information
Abstract
목적
특발성 시신경교차염으로 진단된 소아 환자의 임상양상과 치료 결과를 보고하고자 한다.
증례요약
기저질환이 없는 13세 남아가 내원 5일 전부터 시작된 양안의 시력저하로 내원하였다. 최대교정시력은 우안 0.08, 좌안 안전수지 30 cm였고, 안저검사에서 양안의 경미한 시신경유두부종이 관찰되었으며, 시야검사에서 우안 이측반맹, 좌안 전맹 소견을 보였다. 뇌 자기공명영상촬영에서 시교차 부위에 결절성 조영증강이 확인되었다. 뇌척수액 및 혈액검사에서 감염과 자가면역질환의 증거는 없었다. 따라서 특발성 시신경교차염으로 진단하였고 고용량 스테로이드 치료를 시작하였다. 치료 후 5일째 양안의 시력이 호전되기 시작했으며, 1개월째 시야결손은 작은 중심암점만 남기고 거의 소실되었으며, 유두부종은 거의 관찰되지 않았다. 치료 후 4개월째인 현재까지 재발 없이 안정적인 경과를 보이고 있고, 시력은 정상으로 호전되었다.
결론
소아에게서 발생한 특발성 시신경교차염에 대해 스테로이드 치료를 시행하였으며, 시기능은 정상 범위로 회복되었다. 중추신경계 탈수초질환을 시사하는 소견은 확인되지 않았으나, 지연성으로 발생할 수 있는 가능성을 염두에 두고 지속적인 경과 관찰이 필요하다.
Trans Abstract
Purpose
We report a case of idiopathic chiasmal optic neuritis in a pediatric patient.
Case summary
A 13-year-old boy with no history of systemic disease was referred to our ophthalmology clinic because of visual disturbance in both eyes of 5 days in duration. The best-corrected visual acuity was 0.08 in the right eye and finger counting at 30 cm in the left eye; mild blurring of the disc margins (both eyes) was evident on fundus examination, as were temporal hemianopsia in the right eye and diffuse field loss in the left eye. Brain magnetic resonance imaging revealed focal nodular enhancement in the optic chiasm. Blood and cerebral fluid analysis yielded no evidence of infection or autoimmune disease. Therefore, we diagnosed isolated idiopathic chiasmal optic neuritis and commenced a systemic steroid. After 5 days, the visual acuity began to improve, and the field defect was almost eliminated (except for a small central scotoma) at 1 month. He has remained stable to the time of writing (4 months after treatment) and his visual acuity has normalized.
Conclusions
Isolated idiopathic chiasmal optic neuritis developed in a pediatric patient and the visual function improved after steroid treatment. Although there was no evidence of systemic demyelinating disease, regular observation is scheduled given the possibility of late-onset disease.
시신경교차염(optic chiasmal neuritis)은 수직 경선을 따르는 양안의 귀쪽 시야결손과 함께 영상학적 검사에서 시교차의 염증 소견이 나타나는 질환이다[1]. 시신경교차염은 염증성, 감염성, 독성, 자가면역성 기전에 의해서도 발생하지만, 특발성으로 발생하는 경우가 더 흔하다고 알려져 있다. 기존의 특발성 시신경교차염을 주제로 한 연구는 다발경화증과 같은 중추신경계의 탈수초질환의 일환으로 연구한 바가 많고[2-4], 단독 발생을 보고한 바는 흔하지 않다[5]. 본 저자는 단독으로 발생한 특발성 시신경교차염 소아 환자 1예를 경험한 증례를 보고하고자 한다.
증례보고
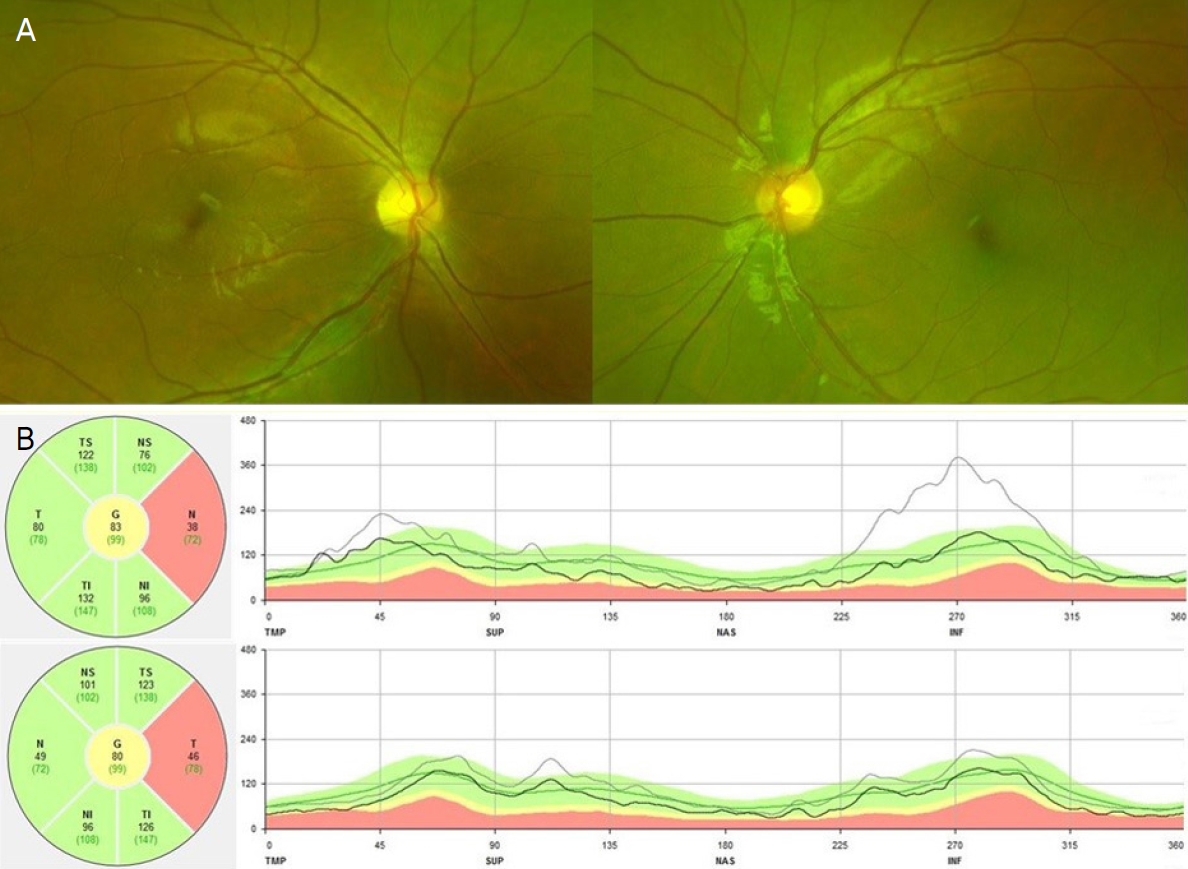
13세 남아가 내원 5일 전부터 시작된 양안의 시력저하로 내원하였다. 기저질환 없이 건강하였던 환아로 안과적 수술력 및 외상력은 없었다. 내원 당시 최대교정시력은 우안 0.08, 좌안 안전수지 30 cm였고, 좌안의 경미한 상대구심동공운동장애가 관찰되었다. Hardy-Rand-Rittler 색각검사상 양안의 저명한 색각이상이 있었으며, 험프리시야검사상 우안의 이측반맹, 좌안의 전맹 소견이 관찰되었다(Fig. 1A). 안저검사상 양안의 경미한 시신경유두부종이 관찰되었으며, 형광안저촬영검사에서는 우안의 시신경유두 부위의 조영증가가 있었고, 형광 누출 소견이 확인되었다(Fig. 2). 빛간섭단층촬영에서는 양안에서 시신경유두 주위 망막신경섬유층의 두께가 증가되어 있었다(Fig. 2). 원인 감별을 위해 시행한 뇌 자기공명영상촬영(magnetic resonance imaging, MRI)에서 다발경화증을 의심할 만한 소견 및 시교차 부위를 압박하는 종괴는 없었고, 시교차 부위의 좌측 전체와 우측 일부에서 결절성 조영증강(nodular enhancement)이 확인되었다(Fig. 3). 뇌 자기공명혈관조영술에서 협착이나 폐쇄, 동맥류와 같은 혈관 이상은 없었고, 뇌 척수액검사에서도 특이점은 없었다. 혈액검사에서 감염이 의심되는 소견은 없었으며, 류마티스 인자와 항핵항체(antinuclear antibody) 등 자가면역질환을 나타내는 표지자에서도 음성 소견을 보였다. 항아쿠아포린4항체검사에서도 음성 소견을 보였으며, 사르코이드 유두염을 배제하기 위하여 검사한 항목인 혈청 안지오텐신 전환 효소는 정상 범위였고, 전신검사에서 결절성 홍반 등의 피부병변은 확인되지 않았으며, 단순 흉부 촬영에서 특이 소견은 없었다.

Visual field test (30-2 threshold) in both eyes. (A) On the admission day, a temporal hemianopsia in the right eye and total anopsia in the left eye was noted. (B) At 5 days after treatment, temporal hemianopsia of the right eye showed regression. (C) At 11 days after treatment, there was regression except small central scotoma in both eyes. (D) Visual field defect on both eyes were almost improved at 1 month after treatment.

Fundus photographs, fluorescein angiography and optical coherence tomography at first visit. Optic disc swelling with blurred margin in both eyes was seen in his fundus photographs (A), and leakage of dye near optic disc in the right eye was noted in fluorescein angiography (B). Thickening of retinal nerve fiber layer in both eyes were seen (C). TS = temporosuperior; NS = nasosuperior; T = temporal; N = nasal; TI = temporoinferior; NI = nasoinferior; G = global; TMP = temporal; SUP = superior; NAS = nasal; INF = inferior.
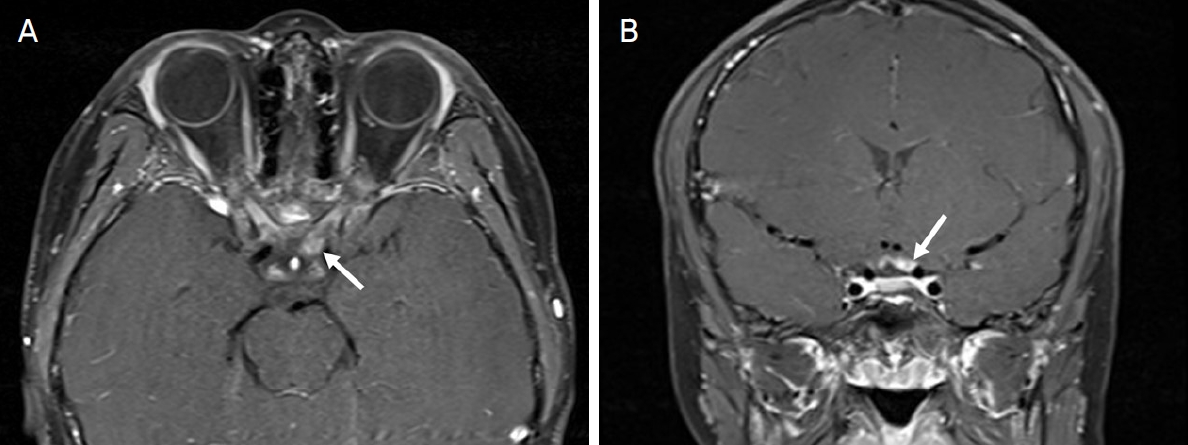
The gadolinium-enhanced brain magnetic resonance imaging before treatment. Axial (A) and coronal (B) views revealed the focal nodular enhancement of the left side in optic chiasm (arrows).
이에, 임상학적 소견과 영상검사, 혈액검사 등을 종합하여 특발성 시신경교차염으로 진단하였고 고용량 스테로이드 Methyl-prednisolone (MethysolⓇ, Reyon Pharm, Ltd., Seoul, Korea)을 5 mg/kg을 하루 4번 3일간 투여하였으며, 용량을 반으로 줄여 3일간 추가 정맥 주입하였다. 이후 경구용 스테로이드 Prednisolone (SolondoⓇ, Yuhan Corp., Seoul, Korea)로 전환하여 점차 감량하였다. 치료 후 5일째 교정시력 우안 0.7, 좌안 0.01로 양안의 시력이 호전되기 시작했으며, 시야검사에서 우안 시야결손의 저명한 호전이 확인되었다(Fig. 1B). 치료 후 11일째 교정시력은 우안 0.9, 좌안 0.02였고, 시야결손은 양안의 중심 암점 형태로 관찰되었다(Fig. 1C). 치료 후 1개월째 교정시력 우안 0.9, 좌안 0.5였으며, 시야결손은 작은 중심암점만 남기고 거의 소실되었다(Fig. 1D). 안저검사에서 시신경유두부종도 완전히 호전되었다(Fig. 4). 치료 후 4개월째인 현재까지 시신경교차염은 재발 없이 안정적인 경과를 보이고 있고, 최대교정시력은 양안 모두 1.0이었으며, 색각검사 및 시야검사에서도 양안에서 정상이었다.
Fundus photographs and optical coherence tomography after treatment. Optic disc swelling in both eyes was improved (A). Thickening of retinal nerve fiber layer in both eyes decreased (black line), compared to initial visit (gray line) (B). TS = temporosuperior; NS = nasosuperior; T = temporal; N = nasal; TI = temporoinferior; NI = nasoinferior; G = global; TMP = temporal; SUP = superior; NAS = nasal; INF = inferior.
고 찰
시신경교차염은 단안 혹은 양안의 급격한 시력저하와 함께 수직 경선을 따른 시야결손이 동반된 환자에게서 영상 검사와 종합하여 진단할 수 있다. 시신경염에서 나타나는 일반적인 증상인 시야장애, 색각이상, 대비민감도 저하 등의 시기능 이상이 관찰되고, 광시증, 눈부심의 증상이 나타날 수 있는데[6], 안통을 호소하는 빈도는 특발성 시신경염에 비하여 현저하게 적다고 알려져 있다[1]. 기존의 보고에서 중추신경계 탈수초질환의 일환으로 보고된 시신경교차염을 주제로 한 연구는 있으나 단독으로 발생한 시신경교차염을 보고한 바는 드물다. 특히 국내에서는 Kim and Chang [5]이 25세 환자의 시신경교차염을 경험한 증례를 보고한 바 있으나 소아 환자의 증례는 본 연구가 처음이다.
시신경교차염은 다양한 원인에 의해 발생할 수 있다. 엡스타인-바 바이러스(Epstein-Barr Virus), 수두대상포진바이러스(Varicella Zoster Virus), 볼거리 바이러스(Mumps Virus) 등의 바이러스 감염, 혹은 결핵균, 크립토코커스 감염이 원인이 된 시신경교차염 증례들이 보고되었으며[7,8], 사르코이드증과 같은 염증성 원인, 모야모야 병과 같은 허혈성 원인, 전신홍반루푸스와 같은 자가면역성 원인에 의한 시신경교차염의 증례들이 보고되었다[9,10]. 특발성으로 발생하는 빈도가 가장 높지만[1], 감염성, 허혈성, 자가면역성 원인에 대한 충분한 검사를 통하여 정확한 원인을 감별하여 그것에 대한 치료를 병행하는 것이 중요하다.
시신경교차염을 진단하는 데 있어 뇌 MRI는 중요한 역할을 한다. 대부분이 뇌 MRI에서 시교차 부위의 조영증강이 확인되지만, 일부에서는 그렇지 않은 경우도 있다[1,5]. Kawasaki and Purvin [1]은 뇌 MRI를 시행한 시신경교차염 환자 중 80%에서 시교차의 비대 혹은 시교차 부위의 조영증강이 확인되었으나, 20%에서는 영상검사에서 시교차 부위의 병변이 나타나지 않았다고 보고하였다. 더불어 Miller et al [11]의 보고에서도 시신경염으로 진단된 37명 환자의 뇌 MRI를 분석하였을 때 시교차 부위에 이상을 보이는 비율은 2%로 드물다고 하였는데, 부검을 통해 시교차 부위의 병변이 확인되더라도 뇌 MRI에서는 병변이 잘 나타나지 않는 원인으로 시교차 부위와 주위 뇌척수액과의 대조도가 낮아 영상에 잘 나타나지 않고, 시교차의 병변은 크기가 작더라도 시신경전도장애를 일으킬 수 있으므로 임상증상에 비해 매우 작은 병변이 관찰되지 않았을 수 있기 때문이라고 하였다[5,11]. 본 증례의 뇌 MRI에서는 시교차 부위의 좌측 전체와 우측 일부에서 조영증강이 관찰되었고, 임상증상으로 우안 이측반맹, 좌안 전맹 소견이 있어서, 영상검사에서 확인된 병변과 안과적 소견이 상응하는 것을 확인할 수 있었다.
소아에서 발생한 시신경염은 양안 침범 및 시신경유두부종을 보이는 경우가 많다고 알려져 있다[12]. 본 증례의 특이점은 안저검사에서 관찰된 유두염의 정도가 우안이 심하고 좌안은 경미하지만 시력저하와 시야결손은 오히려 좌안이 심하였다는 점인데, 이는 환자의 시기능에 시신경교차 부위의 결절성 염증이 유두부의 염증보다 더 큰 영향을 미쳤기 때문일 수 있다. 즉 뇌 MRI에서 확인된 결절성 조영증강의 위치가 시교차와 인접한 좌측 시신경 전체를 포함하면서 시교차 몸체까지 이어진 것으로 볼 때 이 병변으로 인하여 좌안 시야의 광범위한 결손 및 심한 시력저하가 나타났고, 우안은 유두부의 염증 및 시교차 몸체의 염증으로 인한 시야결손 및 시력저하가 나타나서 상대적으로 좌안보다 시기능의 손상이 덜 하였던 것으로 생각된다.
소아 시신경염을 주제로 한 과거 연구에서 진단 당시 뇌 MRI에서 다발경화증을 의심할 만한 소견은 없었던 소아 시신경염 환자 15명 중 5명에서 평균 2년 내에 다발경화증이 발병하였다는 연구 결과[13] 및 특발성 시신경교차염으로 치료 후 3년이 지나 지연성으로 다발경화증이 이환된 경우도 보고되므로[1], 본 증례에서도 추후의 경과 관찰에서 중추신경계의 탈수초질환의 발병 여부를 유심히 확인하여야 한다. 더불어 최근 연구에서 시신경염이 반복되거나 양안으로 발생한 소아 시신경염에 있어서 항미엘린희소돌기세포당단백질(antimyelin oligodendrocyte-glycoprotein, MOG) 항체의 임상적 유용성이 대두되고 있는데, 본 증례에서는 MOG 항체 검사를 시행하지 못한 한계가 있다[14].
시신경교차염에 특화된 치료 방침은 현재까지 정립되지 않았지만, 역학과 임상양상, 시력예후, 추후 다발경화증이 발생하는 양상 등이 특발성 시신경염과 차이가 없다는 점에서 Optic Neuritis Treatment Trial (ONTT)에서 제시된 가이드라인에 따라 치료를 시행하는 것이 일반적이다[1,15]. 특히 소아의 시신경염의 치료는 ONTT와 같은 대규모 연구가 이루어지지 않았기에 사용하는 스테로이드 용량은 보고마다 다른데[6], 본 증례에서는 methyl-pednisolone (MethysolⓇ, Reyon Pharm, Ltd.) 5 mg/kg을 하루 4번 3일간 투여하였고, 용량을 반으로 줄여 3일간 추가 정맥 주입하였다. 이후 경구요법으로 전환하여 감량하였으며, 임상적으로 시력회복과 시야결손의 호전을 확인하였다.
본 증례는 특발성 시신경교차염 소아 환자에 대해 고용량 스테로이드 치료를 시행한 후 호전을 보인 증례로, 4개월의 경과 관찰 동안 중추신경계 탈수초질환을 시사하는 소견은 확인되지 않았으나 과거 발표된 연구를 보았을 때 지연성으로 발생할 수도 있다는 가능성을 염두에 두고 지속적인 경과 관찰이 필요하다. 이러한 증례는 기존에 국내에서 유사 증례가 보고된 바 없기에 임상에서 소아 환자의 시신경교차염을 진료하는 데 도움이 될 것으로 생각한다.
Notes
Conflicts of Interest
The authors have no conflicts to disclose.
References
Biography
전재평 / Jae Pyeong Jeon
대구파티마병원 안과
Department of Ophthalmology, Daegu Fatima Hospital
