실리콘관삽입술 환자에서 콧속 실리콘관 위치와 배양 결과에 대한 연구
Tube Position and Culture in the Nasal Cavities of Patients Treated with Silicone Tube Intubation
Article information
Abstract
목적
실리콘관삽입술 후 비강 내 실리콘관의 위치와 방향 변화와 수술 후 임상양상과의 관계를 알아보고자 하였다.
대상과 방법
이 연구는 코눈물관폐쇄로 진단받고 실리콘관삽입술을 시행한 52명 70안을 대상으로 시행하였다. 실리콘관 삽입 직후 비강 내 실리콘관의 위치 및 방향과 제거 전 위치 및 방향을 비교하였다. 균 배양은 실리콘관 삽입 전에는 비강 내 면봉 배양검사를 시행하였고 제거 시에는 제거된 실리콘관으로 세균 및 진균 배양을 시행하였다.
결과
비강 내 실리콘관 길이는 삽입 직후 8.7 ± 3.1 mm에서 제거 시 7.3 ± 3.4 mm로 감소하였으며, 방향은 후방으로 이동하는 양상이었다(p<0.05). 세균 배양률은 실리콘관 삽입 전 94.3%에서 제거 시 75.7%로 변했다. 가장 흔한 그람 양성균은 술 전후 모두 혈청응고효소 음성 포도상구균이 제일 많았고, 그람 음성균은 술 전 클리브시엘라 막대균에서 술 후 스테노트로포모나스 말토필리아로 변했다. 진균 배양률은 7.1%에서 51.4%로 변화하였고, 후방으로 이동하는 양상일 때 진균 배양 양성률이 증가하였다(p<0.05). 실리콘관의 길이 및 방향은 임상증상, 눈꺼풀높이의 변화와 상관관계가 없었다.
결론
실리콘관삽입술 후 비강 내 실리콘관 길이는 짧아지고, 고정 부위 방향이 후방으로 이동하는 경향을 보였다. 이와 함께 비강 내 진균 배양률이 증가하는 양상을 고려하면 비강 내 실리콘관 고정 부위를 아래콧길 전방에 위치시키는 것이 좋을 것으로 생각한다. 추후 눈물배출계의 위치에 따른 진균 배양에 대한 연구가 추가적으로 필요할 것이다.
Trans Abstract
Purpose
To evaluate the relationship between the position and direction of a silicone tube in the nasal cavity after silicone tube intubation and clinical features.
Methods
This study included 70 eyes of 52 patients who were diagnosed with nasolacrimal duct obstruction and had silicone intubation surgery. The position and direction of the silicone tube were compared after tube intubation and before extubation. An intranasal swap culture was performed before tube intubation, and the removed silicone tubes were cultured.
Results
The length of the silicone tube decreased from 8.7 ± 3.1 mm after intubation to 7.3 ± 3.1 mm before extubation, and the direction of the tube moved backward in the nasal cavity (p < 0.05). The bacterial culture rate changed from 94.3% before intubation to 75.7% before extubation. The most common Gram-positive bacteria (both preoperative and postoperative) was coagulase-negative Staphylococcus aureus. The most common Gram-negative bacteria were converted from Klebsiella aerogenes to Stenotrophomonas maltophilia. The fungal culture rate changed from 7.1% to 51.4%, and the culture rate increased when the silicone tube direction was moved backward (p < 0.05). The length and direction of the silicone tubes were not correlated with clinical symptoms or changes in eyelid height.
Conclusions
The length of the silicone tube in the nasal cavity decreased, and the tube tended to move in a posterior direction after silicone tube intubation. Considering the increase in the intra-nasal fungal culture rate, it is better to place the silicone tube in the anterior part of the nasal cavity from the inferior meatus. To clarify further the fungal infection and its clinical findings, a study of cultures with respect to location in the lacrimal system would be required.
눈물흘림 증상으로 코눈물관폐쇄를 진단받은 환자들은 주로 눈물배출계의 염증과 섬유화가 발생할 수 있으며 폐쇄 정도에 따라 내시경적 혹은 피부경유눈물주머니코안연결술을 시행할 수 있다[1-3]. 이후 코눈물관폐쇄 환자에서 눈물주머니코안연결술 없이 실리콘관삽입술 단독으로 시행한 수술에서의 높은 성공률이 보고되었고[4,5], 침습적인 수술적 치료의 감소를 위해 실리콘관삽입술 시행 중 눈물길 폐쇄 병변의 확인 및 비강 내 관찰이 가능한 비내시경과 눈물길미세내시경을 이용한 실리콘관삽입술의 유용성에 대한 연구들이 보고되었다[6-8].
눈물주머니코안연결술에 비해 실리콘관삽입술이 비침습적이며 비점막을 보호한다는 수술 방법의 유용성에도 불구하고 흔한 합병증으로 실리콘관의 조기 이탈 및 실리콘관의 유지기간에 따른 만성적 자극 등이 발생할 수 있으며[9], 이에 따라 실리콘관의 길이 및 실리콘관의 유지기간에 따른 합병증 및 수술 성공률에 대한 많은 연구들이 보고되었다[10-16].
실리콘관의 위치가 비강으로 갈수록, 실리콘 관의 길이가 길수록 관 주변의 염증 반응이 심하게 나타나며, 삽입 기간이 길수록 눈물배출계의 염증과 섬유화를 보고한 연구들이 보고되었다[15,16]. 이에 본 연구는 실리콘관삽입술 후 비강 내 실리콘관의 위치를 조사하고 수술 후 임상양상과의 관계를 알아보고자 하였다.
대상과 방법
2018년 4월부터 2018년 10월까지 눈물흘림을 주소로 본원을 방문한 환자 중 병력 청취, 세극등검사, 눈물소관관류검사, 빛간섭단층촬영(spectral-domain optical coherence tomography, SD-OCT; SPECTRALIS®, Heidelberg Engineering, GmbH, Heidelberg, Germany)을 이용한 아래눈물띠높이(tear meniscus height, TMH)검사 및 눈물주머니조영술 시행을 통해 코눈물관폐쇄로 진단받은 후 눈물길미세내시경을 사용하여 실리콘관삽입술을 시행받고, 실리콘관 제거 이후 1달 이상 외래 경과 관찰이 가능했던 환자 52명 70안을 대상으로 의무기록의 후향적 분석을 통해 연구하였다. 단, 급성 누낭염, 부비동염 수술, 비염 등의 감염 치료의 기왕력이나 치료가 필요한 경우는 대상에서 제외하였다.
모든 수술은 환자의 동의를 얻은 후 한 명의 수술자(H. Lew) 의해 전신마취 혹은 국소마취하에 시행되었다. 눈물점 확장기를 이용하여 눈물점을 확장한 후 눈물점을 통해 직경 0.9 mm의 probe tip, bent type 눈물길미세내시경(RUIDO Fiberscope, FiberTech Co., Tokyo, Japan)을 삽입한 후 내시경에 연결된 관류 통로로 생리식염수를 관류하며 위 및 아래 눈물소관, 공통눈물소관, 눈물주머니, 코눈물길, 비강에 이르는 눈물길 내부 상태를 확인하였다. 또한 눈물점에서 하비도까지 실리콘관삽입술을 시행한 후 코 내부에서 실리콘관을 견인하여 적당한 장력을 유지해 3 mm 길이의 Hem-o-lok 클립(Weck® Hem-o-lok® Polymer locking ligation system, Teleflex Medical, Durham, NC, USA)으로 고정한 후 비강 내에 위치시켰다(Fig. 1).
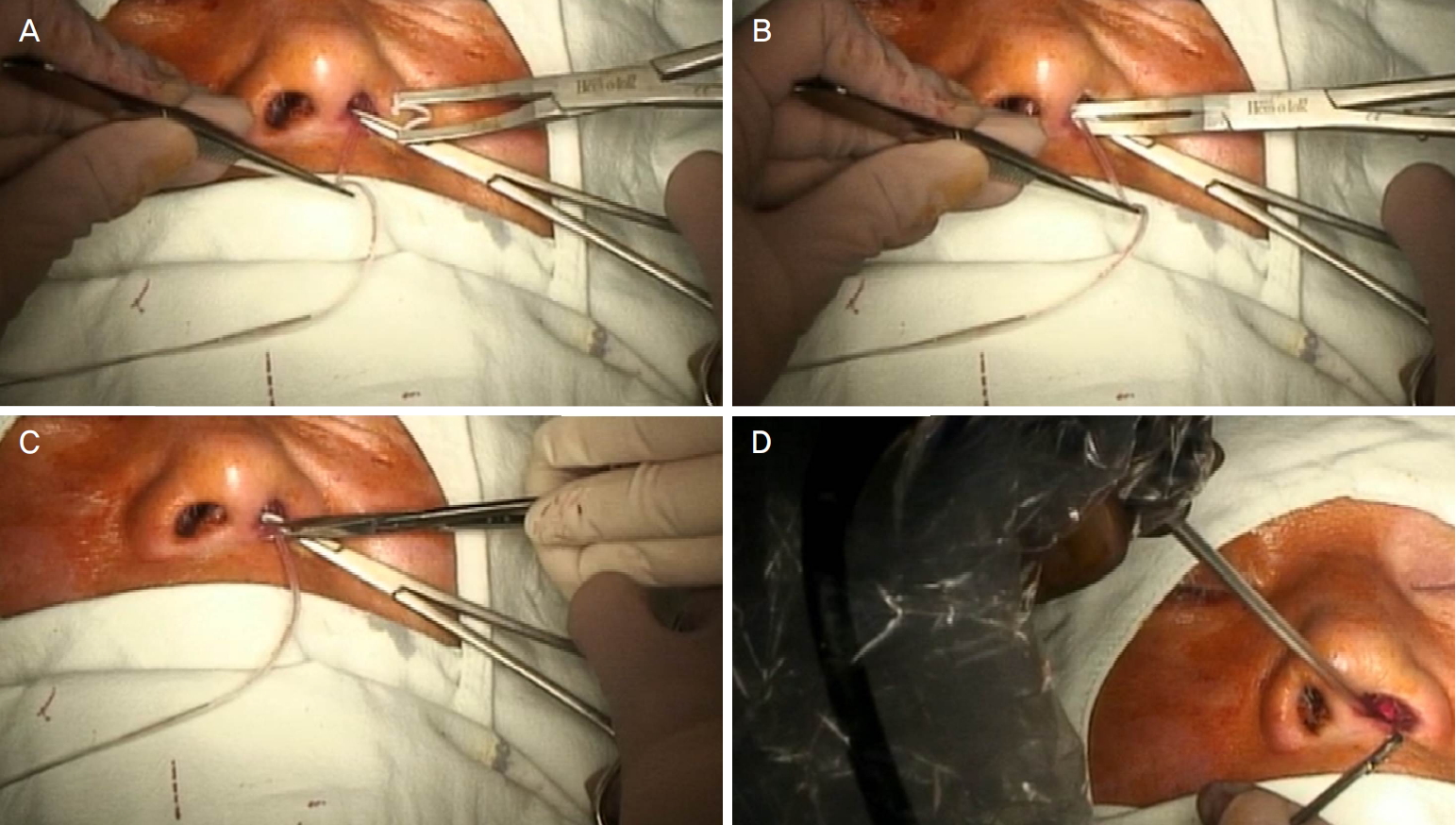
The method of silicone tube fixation by using Hem-o-lok in the nasal cavity. (A) Attraction silicone tube from the nasal cavity with smooth forceps. (B) Fixation silicone tube with Hem-o-lok. (C) Cutting about 1 cm length from the Hem-o-lok fixing part. (D) Exploration of the silicone tube and fixed Hem-o-lok in the nasal cavity by using nasal endoscopy.
수술 후 1주일 동안만 하루 4회 0.04% mitomycin 점안액(Mitomycin® -C Kyowa inj., Kyowa Kirin Co., Ltd., Tokyo, Japan), 0.5% levofloxacin 점안액(Cravit®, Santen Pharmaceutical Co., Ltd., Osaka, Japan), 0.1% fluorometholone 점안액(Flumetholone®, Santen Pharmaceutical Co., Ltd.)을 점안하였고, 술 후 1주 이후의 시점에서는 mitomycin 점안액 사용의 중단 및 levofloxacin과 fluorometholone 점안액을 하루 2회 점안하면서 2개월, 4개월, 6개월 또는 그 이상 시점에서 외래 경과 관찰하였다.
비강 내 실리콘관 위치는 실리콘관 삽입 후와 실리콘관 제거 시 실리콘관의 길이와 방향으로 측정하였다. 실리콘관의 비강 내 길이는 지름 0.94 mm의 실리콘관 두께를 참고하여 실리콘관을 고정한 Hem-o-lok에서 아래콧길까지의 거리로 정의하고 Image J program (NIH, Bethesda, MD, USA)을 이용하여 측정하였고, 비강 내 방향은 아래콧길을 기준으로 실리콘관이 어느 방향으로 향하는지로 정의하였다(Fig. 2).
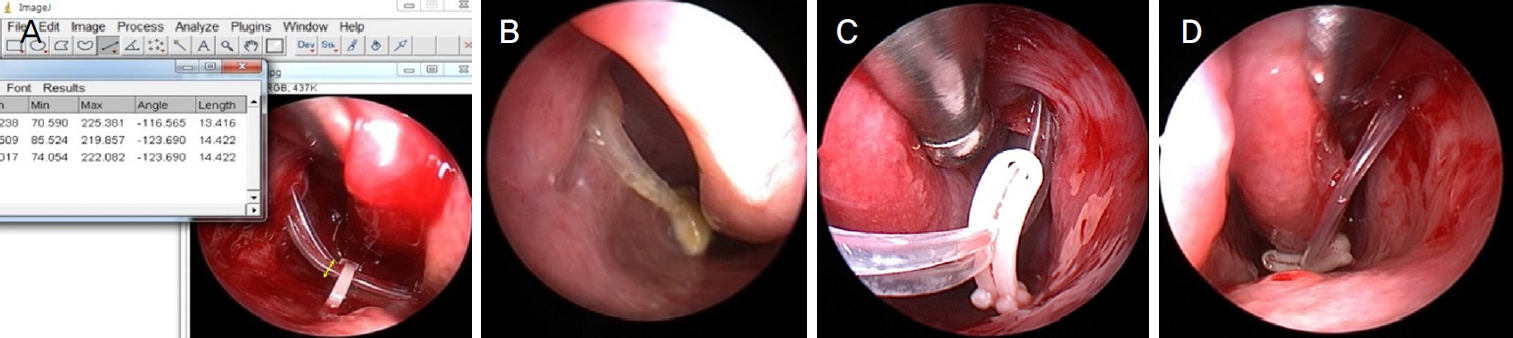
Evaluation of the nasal position silicone tube in terms of length and direction. (A) Measurement of the length of a silicone tube from the hem-o-lok to an inferior meatus based on a silicone tube with a diameter of 0.94 mm using Image J program. (B) Neutral direction based on the inferior meatus. (C) Anterior direction based on the inferior meatus. (D) Posterior direction based on the inferior meatus.
위눈꺼풀높이는 눈꺼풀각막반사간거리 1 (marginal reflex distance 1, MRD1)로 환자의 사진을 토대로 Image J program 을 이용하여 측정하였다. 비강 내 세균 및 진균 배양검사는 수술 전 비강 내 면봉배양검사의 결과와 실리콘관제거 시 실리콘관을 무균의 유리관에 담아 진단검사실로 보낸 후 진행되었다. 배양 실시 4주까지 진균이 자라지 않는 경우를 진균 배양 음성으로 간주하였다. 수술 성공은 실리콘관 제거 후 Munk score 1점 이하 및 아래눈물띠높이 300 µm 이하인 경우로 정의하였다.
통계적 분석은 SPSS version 25.0 (IBM Corp., Armonk, NY, USA)을 이용하였고 independent t-test, paired t-test, Phi correlation, Cramer’s V test를 이용하여 결과를 검증하였으며, p-value가 0.05보다 작은 경우를 통계학적으로 유의한 것으로 보았다. 본 연구는 본원 의학연구심의위원회(Institutional Review Board, IRB)의 승인을 받고(승인 번호: 000-2019-11-030) 연구관련 심의 규정 및 지침에 따라 진행되었다.
결 과
대상 환자의 연령은 62.1 ± 18.0세였고, 남자 17안(24.3%), 여자 53안(75.7%)이었으며 눈물 흘림 증상의 기간은 4.6 ± 6.5년이었다. 실리콘관 삽입 기간은 5.3 ± 0.8개월이었다. 수술 전 Munk 점수는 평균 3.7 ± 1.0이었으며 수술 후 평균 1.0 ± 1.1이었고, SD-OCT를 사용하여 측정한 수술 전 평균 TMH는 431.0 ± 216.4 µm였고, 수술 후 285.4 ± 209.2 µm였다(Table 1).

Demographic characteristics of subjects
비강 내 실리콘관의 길이는 삽입 직후 8.7 ± 3.1 mm에서 제거 시 7.3 ± 3.4 mm로 의미있게 감소하였으며(p=0.012), 실리콘관의 방향은 삽입 직후에 비해 후방으로 이동하였으며(p=0.001), 통계학적으로 유의하게 나타났다(Table 2). 전체 수술 성공률은 80.4% (57/70)였으며, 비강 내 실리콘관 길이 및 방향은 임상증상(이물감, 염증, 이탈 등), 위눈꺼풀 높이의 변화, 성공률과 통계학적으로 유의한 상관관계가 없었다(Table 3). 실리콘관 길이는 세균 및 진균 배양검사 결과와 유의한 상관관계가 없었으나, 실리콘관의 방향을 후방으로 이동하였을 때 진균 배양 양성률이 증가하였으며(p=0.008), 통계학적으로 유의하게 나타났다(Table 3).
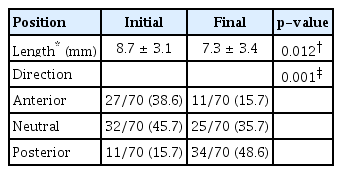
Position of silicone tubes in the nasal cavity (mm)
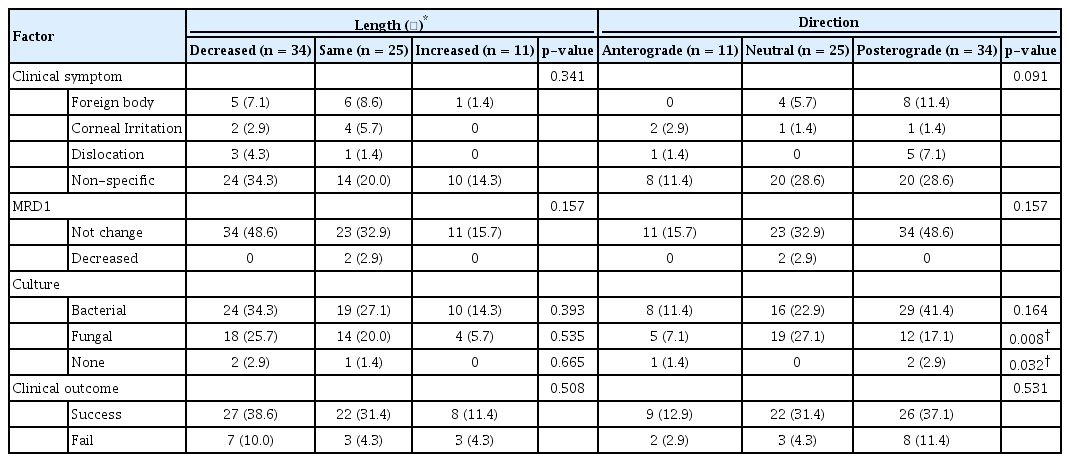
Correlations of changes in silicone tube length, direction and clinical findings
본 연구에서 실리콘관 삽입 전 94.3%의 세균 배양률을 보였으며, 그람 양성균 82.9%, 그람 음성균 11.4%였다. 실리콘관 제거 후에는 75.7%의 세균 배양률을 보였고, 그람 양성균 48.6%, 그람 음성균 27.1%였다. 수술 전후 모두 가장 흔한 그람 양성균은 Coagulase-negative staphylococcus으로 나타난 반면, 수술 전 가장 흔한 그람 음성균은 Klebsiella aerogenes에서, 수술 후는 Stenotrophomonas maltophilia로 나타났다(Table 4).

Comparison of bacteria and fungus culture in the nasal mucosa
실리콘관 삽입 전 진균 배양률은 7.1%였고 가장 흔한 진균은 Candida였다. 실리콘관 삽입 후 진균 배양률은 51.4%로 증가하였고(p<0.001), 실리콘관이 가운데 위치(neutral)하였던 경우에서 진균 배양률이 가장 높았으며 candida (22.9%)와 trichophyton (21.4%)이 흔한 균주로 나타났다(Table 4).
고 찰
비강 내 미생물에 대한 기존의 여러 연구에서 비강 내에는 정상적으로 세균 및 진균이 존재할 수 있으며 코눈물관폐쇄가 정상 상재균 조성의 변화 및 균주와 병적 균주의 과성장을 유발시킬 수 있다는 것이 보고되었다[17-22]. Purgason et al [22]은 코눈물관폐쇄에서 Candida albicans가 코눈물관폐쇄의 직접적인 원인이 될 수 있음을 증명한 바 있다.
코눈물관폐쇄의 치료로 실리콘관삽입술의 성공률은 보고된 연구마다 차이가 있지만 모두 높은 성공률을 보였다[4-8]. 그러나 코눈물관에 삽입된 실리콘관 주변에서 염증 반응이 발생할 수 있으며 비강쪽으로 갈수록, 실리콘관이 길수록 염증 반응이 심하게 나타난다고 보고된 바 있으며[15], 수술 후 감염 및 염증이 비강 내의 실리콘관과 관련이 있을 수 있다고 제시하고 삽입 기간이 길수록 눈물배출계의 염증과 섬유화를 유발한다고 보고되기도 하였다[16,23]. 본 연구에서는 비강 내 실리콘관의 위치가 수술 후 감염 및 임상증상, 수술 성공률에 미치는 영향에 대해 알아보고자 하였다. 이전의 연구와 달리 비강 내 실리콘관 길이는 감소하는 양상을 보이나 실리콘관의 길이와 세균 및 진균 배양 양성률, 임상양상과는 관계가 없었다. 흥미롭게도 실리콘관의 위치는 후방으로 이동하는 양상을 보이면서 진균 배양 양성률이 증가하는 양상을 보이나 이것이 임상양상 및 수술 성공률과는 관계가 없었다.
Shin et al [24,25]은 액상 도말 세포진검사를 이용한 실리콘관 주위 세포학적 관찰을 통해 실리콘관삽입술보다 눈물주머니코안연결술군에서 균사 관찰이 유의하게 높았으며, 실리콘관을 3등분하여 진균 배양을 하였을 때 실리콘관 위치가 비강에 가까울수록 진균 배양률이 높게 나타났고 실리콘관삽입술군에서는 Trichsporon spp.이 가장 높게 배양됨을 보고한 바 있다. Moon and Ahn [26]은 실리콘관 위치에 따른 세균 및 진균 배양률을 보고하였으며 실리콘관의 위치가 비강에 가까울수록 진균 배양률이 높게 나타났으나 배양된 진균은 모두 Candida spp.였고 위치에 따른 세균 총 배양률 및 세균 종류별 배양률의 차이는 보이지 않았다고 보고하였다. 두 연구 모두 실리콘관에서 배양된 균과 임상증상과의 연관성의 측면에서 실리콘관삽입술 전 세균 및 진균에 대한 연구가 필요함을 시사하였다. 본 연구에서는 기존 연구와는 다르게 수술 전후 비강 내 세균 및 진균 배양률 및 종류에 대해 비교하였으며, 술 전에 비해 술 후 진균 배양률이 크게 증가함을 확인하였고 비강 내 가장 흔한 균주도 술 전에는 Candida spp.에서 술 후 Candida spp. 외, Trichophyton spp.이 증가함을 알게 되었다. 술 전 진균 배양률이 매우 낮아 결과 해석에 한계가 있지만 이와 같은 결과로 보아 코눈물관폐쇄 환자에서 술 후 실리콘관에서의 진균 배양이 술 전 존재보다는 술 후 이차적으로 증가되었을 가능성이 큰 것으로 볼 수 있겠다.
제거된 실리콘관에서 그람 양성균과 음성균 모두 동정될 수 있으며 연구마다 다르지만 60%부터 94%까지 세균 양성 배양률이 보고되었다[18,23,27-29]. Ali et al [27]은 94%의 세균 양성 배양률과 가장 흔한 균주는 P.aerusinosa와 S.aureus라고 보고하였고, Chaudhry et al [18] 역시 가장 흔한 그람 양성균은 Staphylococcus species이고 그람 음성균은 P. aerusinosa와 Haemophilus species이라 보고하였다. 수술 성공과 관련하여 여러 연구들에서 P. aerusinosa와 수술 실패와 같은 합병증이 관련 있다고 보고하였다[23,28-30]. 본 연구에서는 술 전후 세균 배양률 및 균주 동정을 비교하였는데, 술 전 94.3%, 양성 배양률에서 75.7%로 오히려 감소하는 양상을 보였으며 술 전후 모두 가장 흔한 그람 양성균은 Staphylococcus species였고, 그람 음성균은 술 전 Klebsiella aerogenes에서 술 후 Stenotrophomonas maltophilia가 가장 많이 동정되었다. 이는 술 후 사용한 levofloxacin 점안액으로 인해 술 후 세균 양성 배양률이 감소하였으나, 술 후 실리콘관의 염증 반응 과정으로 병적 균주 조성 변화와 과성장이 발생하여 S. maltophilia와 같은 다제 내성 그람 음성균의 등장으로 그람 음성균의 배양률이 증가하였을 것으로 생각해 볼 수 있다.
이러한 미생물군의 변화가 코눈물관폐쇄에 의해서도 발생할 수 있으나 실리콘관삽입술로 인해 상재균 및 병적 균주에 의해 생물막이 형성될 수 있으며[29,30], 일단 생물막이 형성되면 여기에서 세균과 진균이 성장할 수 있다. 따라서 이로 인해 수술 전후 배양된 세균의 균주 변화 및 진균 배양률의 증가가 발생하였을 것으로 사료된다. 그러나 본 연구에서 실리콘관의 균 배양률 및 균 종류와 수술 성공률과 관계가 없었기에 실리콘관의 세균 및 진균 유무가 수술 후 경과에 직접적인 영향을 끼치지는 않을 것으로 사료되나, 실리콘관의 방향 변화가 진균 배양률을 증가시키는 것으로 보아 실리콘관 고정 시 고정 부위를 아래콧길 전방에 위치시키는 것이 좋을 것으로 생각한다.
실리콘관 삽입 후 코눈물관폐쇄의 원인은 아직 확실하지 않으나, 지금까지 많은 연구에서 수술 후 재협착의 원인으로 감염과 염증에 중점을 두었다. 그러므로 술 후에도 지속적인 염증 소견 및 감염 소견이 존재하는 경우 진균 감염 및 항생제 내성을 고려한 치료가 임상적으로 중요하다고 생각한다.
본 연구에서는 대상과 방법에 기술한 바와 같이 기존 연구에서 눈물배출계 위치에 따라 실리콘관을 세 부분이나 네 부분으로 구분하여 세균 및 진균배양검사를 시행하지 못한 점, 그리고 실리콘관 고정 시 사용한 hem-o-lok 클립 자체에 의한 실리콘관 위치 변화 요소를 비교할 수 있는 봉합사를 사용하는 대조군이 없다는 점에서 한계가 있다. 그러나 본 연구는 실리콘관삽입술 직후와 제거 시 비강 내 실리콘관 위치를 길이와 방향으로 구분하여 조금 더 구체적이고 가시적으로 평가할 수 있는 방법을 제시하였을 뿐만 아니라 실리콘관에서 균주 및 진균 배양의 결과를 비교함으로써, 술 전에 비해 술 후 비강 내 진균 배양률이 의미있는 증가를 보고한 것이라는 데에 의의가 있다. 진균 배양률과 임상적 소견 및 성공률이 상관관계가 없었던 점을 미루어 보아 코눈물관폐쇄 환자에서 코눈물관협착이나 폐쇄의 발생이 진균 감염의 직접적인 연관성보다는 코눈물관폐쇄로 인해 상재균의 조성의 변화 및 균주 과성장이 발생하여 술 후 실리콘관 표면에 생물막을 형성으로 인한 진균 감염의 증가도 생각해볼 수 있을 것으로 사료된다. 코눈물관폐쇄 환자에서 수술 후 실리콘관 진균 감염의 눈물배출계의 역행성 전파 여부 및 임상적 연관성과의 명확한 인과관계를 알아보기 위해 실리콘관 제거 시 눈물배출계의 위치에 따른 진균 배양에 관한 추가적인 연구가 필요할 것으로 생각한다.
Notes
Conflict of Interest
The authors have no conflicts to disclose.
References
Biography
장정경 / Jeong Kyeong Jang
차의과학대학교 분당차병원 안과학교실
Department of Ophthalmology, CHA Bundang Medical Center, CHA University
