안구운동장애를 동반한 호산구 변종의 육아종증다발혈관염 증례 1예
An Eosinophilic Variant of Orbital Granulomatosis with Polyangiitis with Ocular Motility Disorder
Article information
Abstract
목적
안구운동장애를 동반하고 호산구 및 immunoglobulin E (IgE)의 증가를 초래하는, 안와에 국한된 육아종증다발혈관염(granulomatosis with polyangiitis, GPA)의 호산구 변종(eosinophilic variant) 증례를 보고한다.
증례요약
특이 병력 없는 61세 남자로, 2일 전 발생한 양안 복시로 내원하였다. 최대교정시력 양안 1.0, 좌안의 눈꺼풀부종과 상방 및 하방주시와 외전시 운동 제한을 보였다. 혈액검사에서 세포질 내 항중성구세포질항체 양성, 증가된 호산구 분율(28.3%, 2,462/mm3)과 IgE (400 KU/L)가 이상 소견으로 나타났고, 자기공명영상에서 안와 하이측에 종괴, 눈물샘 확장과 외안근 주위 염증이 관찰되었다. 눈물샘 조직검사에서 국소적 호산구 침윤을 동반한 GPA의 변종으로 진단되었다. 안와 조직에 일차적으로 생성된 GPA에서 전신적호산구 및 IgE 증가증을 동반하는 호산구 변종으로 진단하고, 수술 없이 경구용 스테로이드 치료로 안구운동장애를 완치하였다.
결론
급성 복시를 동반한 안와 염증 환자에서 드물게 GPA가 원인 질환일 수 있으므로 영상검사와 혈액검사를 통한 배제진단이 필요하다.
Trans Abstract
Purpose
To present the case of a patient with localized orbital granulomatosis with polyangiitis (GPA) characterized by a significant ocular motility disorder, increased eosinophilia, and hyper-immunoglobulin E (hyper-IgE).
Case Summary
A 61-year-old male, with no previous history of allergy, atopy, asthma, sinonasal disease, respiratory disease, or renal disease, came to our hospital due to a 2-day history of binocular diplopia. His left eye exhibited inward and upward deviation, along with gaze limitation. His vision was 20/20 in both eyes, and the pupillary light reflex and color test were normal. He had severe eyelid swelling and conjunctival injection without tenderness in his left eye, and retinal vessel congestion around the optic nerve, without proptosis. Laboratory tests revealed a positive cytoplasmic antineutrophil cytoplasmic antibody (cANCA), a normal WBC count, elevated eosinophils at 28.3% (2,462/mm3), and high serum levels of IgE (400 KU/L). Magnetic resonance imaging showed an inferolateral orbital mass with an enlarged lacrimal gland and myositis of the extraocular muscles. A biopsy of the lacrimal gland revealed nonspecific chronic inflammation with an eosinophilic infiltrate. The presence of cANCA, in combination with clinical and pathological findings, led to the diagnosis of an eosinophilic variant of localized orbital GPA. This variant was primarily confined to the orbital tissue, marked by elevated eosinophil and IgE levels, and was treated with oral steroids without requiring surgery for the ocular motility disorder.
Conclusions
GPA may present as acute strabismus with orbital inflammation, even in the absence of systemic signs. Therefore, it should be considered in the differential diagnosis of unexplained acute orbital syndromes.
육아종증다발혈관염(granulomatosis with polyangiitis, GPA)은 과거 베게너 육아종증(Wegener’s granulomatosis)으로 명명되었던 질환으로, 주로 호흡기와 신장의 작거나 중간 크기의 혈관을 침범하는 전신성 괴사성 혈관염 및 육아종성 염증을 특징으로 하는 질환이다.1 서양인에서 이 질환의 눈 및 눈 부속기관 침범은 대략 45-60%로 알려져 있는데,2,3 그중에서 안와 조직에만 국한되어 원발성으로 발생하는 GPA는 약 15%로 추정된다.4 서양인의 눈 및 부속기관에 침범되는 경우보다 한국에서의 보고는 약 18%로 더 낮게 보고되고 있다.5 특히, GPA에 의한 안와 병변은 안와 질환 중 0.4%, 안와의 육아종성 병변 중 17%를 차지하는데, 안와 침범이 GPA의 원발성 부위가 될 수가 있기에 진단 시 주의가 요구된다.4
혈관염에서 호산구증가증은 과거 척-스트라우스증후군(Churg-Strauss syndrome)으로 명명되었던 호산구육아종증 다발혈관염(eosinophilic granulomatosis with polyangiitis, EGPA)의 특징으로, 주요 진단 기준 중 하나이다.1 GPA의 약 12% 이하에서도 호산구증가가 나타날 수 있으나 경미한 정도의 상승을 보이지만,6 특히 EGPA에서처럼 현저한 호산구증가증7-11이나 고면역글로불린E혈증(hyperimmunoglobulinemia E, hyper-IgE)7,10,11까지 동반하는 경우는 매우 드물다. 그리고 GPA에서 아토피나 천식 등 알레르기 질환의 증거 없이 조직 내 호산구 침윤을 보이는 경우를 호산구 변종(eosinophilic variant)으로 정의하는데,12 특히 안와에만 국한되어 증상이 발생한 경우는 매우 드물며,13 국내에서는 아직 보고된 적이 없다.
저자들은 국내에 보고된 적 없는 세포질 내 항중성구 세포질항체(cytoplasmic antineutrophil cytoplasmic antibody, cANCA) 양성 소견, 호산구증가 및 고면역글로불린E혈증의 혈액 소견과 안와의 조직 소견에서 원발성으로 생긴 안와의 호산구 변종인 GPA의 증례를 보고하고자 한다.
증례보고
61세 남자가 2일 전 발생한 양안 복시 증상으로 안과에 내원하였다. 제2형 당뇨의 기저 질환이 있었으나, 그 외 천식, 아토피 등 알레르기 질환이나 호흡기 및 신장 질환 등의 특이 병력은 없었다. 안과검사에서 최대교정시력 우안 1.0, 좌안 1.0, 동공반응 및 색각검사는 정상이었다. 외안부 검사에서 좌안 눈꺼풀부종과 상이측 결막충혈 및 부종이 관찰되었고, 안구돌출이나 압통, 눈운동 시 통증은 없었다(Fig. 1A, B). 안위검사에서는 정면에서 18프리즘디옵터(prism diopters, PD) 좌안 내사시 및 4 PD 좌안 상사시 소견을 보였고, 상방 및 하방주시와 외전시 좌안의 운동제한도 관찰되었다(Fig. 2). 전방 및 유리체 내 염증은 없었고, 안저검사에서는 시신경유두 부위의 망막정맥 울혈 소견이 관찰되었다. 자기공명영상에서 하이측에 조영이 증강되는 약 16×17 mm 크기의 종괴 양상의 병변 및 눈물샘을 포함한 안와 상측, 이측, 하측에 걸친 광범위한 안와 연부조직의 조영증강 소견이 관찰되었다(Fig. 1C-E). 혈액검사에서 cANCA 양성, perinuclear antineutrophil cytoplasmic antibody (pANCA) 등 다른 자가면역항체검사는 음성, erythrocyte sedimentation rate 정상, C-reactive protein는 경도의 상승을 보였다. 백혈구 수치는 정상이면서 호산구 분율은 28.3% (2,462/mm3)로 증가되어 있었고, IgG4는 27.86 mg/dL로 정상인 반면, IgE가 400 KU/L로 상승되어 있었다. 사르코이드증 감별을 위한 혈청 안지오텐신 전환효소검사는 49 U/L로 정상이었고, 흉부 X선 및 소변검사, 매독혈청검사 및 기생충 항체를 비롯한 감염과 관련된 검사에서도 이상 소견은 없었다. 눈물샘 조직검사에서는 림프구, 조직구에 의한 염증 및 국소 호산구 침윤의 소견을 보였으며, 세균 및 진균은 동정되지 않았다(Fig. 1F). GPA의 안와 병변에서 확인되는 조직 소견과 혈액검사상 cANCA 양성을 근거로 전신 침범이 없는 안와 국한형 GPA로 진단하면서, 호산구증가증과 전신 IgE 상승을 동반한 호산구 변종으로 진단되었다. 환자 체중은 60 kg으로, 경구 스테로이드를 1 mg/kg/day 기준으로 처방하여 초기 용량 prednisolone 60 mg/day으로 투약을 시작하였고, 초기 용량 투여 2주째 c-ANCA 음전이 확인되면서, 눈꺼풀과 결막의 부종 및 충혈, 복시 등 임상 증상도 관해를 보였다. 이후 6주간에 걸쳐 1주당 약 10 mg씩 스테로이드 감량 투여하였으며, 26개월간의 경과 관찰 기간 동안 재발의 소견은 없었다.
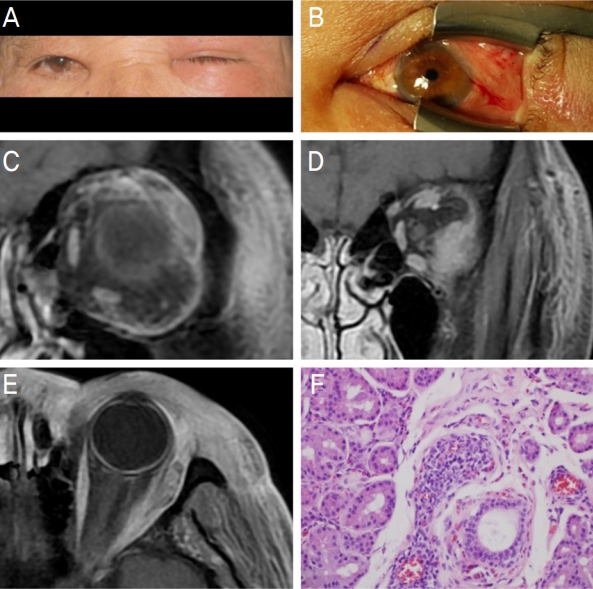
Clinical and histopathologic presentations. Clinical photograph shows periorbital erythematous edema with complete ptosis of the left eye (A). Severe conjunctival injection with chemosis was noted (B). T1-weighted magnetic resonance imaging with fat suppression demonstrates the enlarged lacrimal gland (C), an inferolateral orbital mass of the left orbit (D) and an involvement of lateral rectus muscle (E). Histologic micrograph of lacrimal gland biopsy shows the inflammation composed of lymphocytes, plasma cells and scattered eosinophils (hematoxylin-eosin, original magnifications ×200) (F).
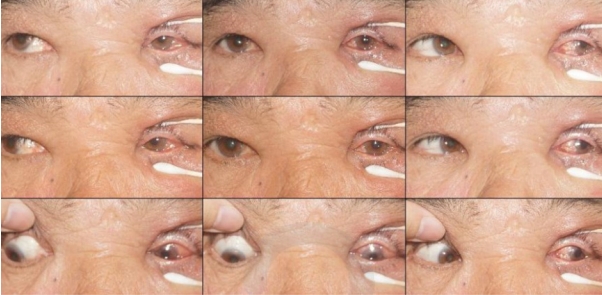
Nine gaze photographs note the esotropia and hypertropia with limitation of depression, elevation and abduction in the left eye.
고 찰
안와 염증 질환은 안와 질환의 약 6%를 차지하며, 병인은 크게 감염과 면역 질환으로 분류된다.14 감염 질환의 원인은 대부분 세균이나 진균이고, 가장 흔한 면역 질환은 특발안와염이지만 전신 질환으로 인한 경우는 갑상샘눈병증이 호발 원인이다.14 특히 안와 염증이 급성으로 발현된 경우 이러한 다빈도의 감염성 안와연조직염, 특발안와염, 갑상샘눈병증 외에도, 드물지만 종양 관련 급성 염증반응이나 육아종성 염증 질환일 가능성도 있어 그에 대한 감별이 필요하다.14 안와 염증을 유발할 수 있는 육아종성 염증질환은 사르코이드증, GPA, EGPA, Erdheim-Chester disease 등으로 대부분 혈액 또는 조직에서 특이적인 생체지표를 보여 진단에 도움이 된다.14
그중 GPA와 EGPA, 이 두 질환은 모두 작거나 중간 크기의 혈관을 침범하는 전신성 혈관염이라는 유사한 특징을 공유하면서도 치료 방침에는 차이가 있기에 서로 감별해야 할 대표적인 질환이다. 이에 대한 노력의 일환으로 2022년 미국 류마티스학회(American College of Rheumatology, ACR)와 유럽 류마티스학회(European Alliance of Associations for Rheumatology, EULAR)가 공동으로 제안하여 GPA와 EGPA의 진단 기준을 새롭게 개정하였다.1 개정된 기준에서는 GPA를 시사하는 임상 기준 3가지, 검사(혈액, 영상, 조직) 기준 5가지, 감별진단 기준 2가지가 정립되었고, 각 항목별 점수가 차등화되어 점수의 합이 5점 이상일 때 GPA로 확진된다. GPA 확진을 시사하는 가장 높은 점수(+5)의 항목은 cANCA 양성이며, 감별진단에서 가장 높은 점수(-4)는 혈중 호산구(≥1×109/liter) 항목인데 혈중 호산구 증가는 EGPA를 강하게 시사하는 주요 진단 기준이다.1 특히 cANCA는 이미 널리 알려진 바와 같이 GPA에서 민감도와 특이도가 높아 최고점의 진단기준으로 인정되고 있다.1,3
GPA는 신장이나 주요 장기 침범을 동반하는 전신형과는 별개로 신장이나 주요 장기 침범이 없는 국소형으로도 발현될 수 있다.3 전신형과 국소형 모두에서 안과적 합병증은 상대적으로 흔하게 발생하는데,2,3 국소형이 안와 조직에만 단독으로 발생하는 형태는 극히 드물며13 국내에서는 이 증례 보고가 처음이다. 비록 EGPA에서는 안와나 안와 부속기 침범이 거의 발생하지 않을 정도로 드무나, GPA가 안와에 국소적 형태로 발생하였을 때에도 EGPA의 가능성을 고려하여 ANCA 등 질병 특이적인 검사를 시행해야 한다.2,15
GPA의 안와 병변 조직 소견에서 전형적인 병리 3징후인 조직의 괴사, 혈관염, 염증반응은 31-54%에서 발생하며,2,15 특히 초기에는 전형적인 혈관염 없이 육아종성 염증만 생기므로15 안와 부위의 조직검사 확진 비율은 그리 높지 않다. 그리하여 개정된 2022년 ACR/EULAR 진단 기준에서는 기존의 병리 3징후보다는 조직검사상 육아종 염증 또는 거대세포의 존재만으로도 2점의 진단 가점이 부여되는 것으로 수정되었다. 본 증례의 경우도 비록 조직검사에서는 비전형적 염증성 병변을 보였으나, 질병 특이 소견인 cANCA가 양성인 점에 더해 혈액 소견상 호산구 및 IgE의 증가를 근거로 하여 GPA의 호산구 변종이라는 세부 진단이 가능하였다.1,4 따라서 임상적으로 안와 질환의 정확한 진단을 위해서는 조직검사뿐 아니라 적절한 혈액검사 소견이 중요하기에, 반드시 질병 특이 소견을 암시하는 검사 기준을 포함한 혈액검사의 병행이 매우 중요하다.
GPA와 EGPA에 대한 명확한 진단 기준의 존재에도 불구하고 드물지만 본 증례처럼 두 질환의 주요 특징이 혼재된 양상으로 나타나는 예들이 보고되었다.7-13 기존의 전통적인 혈관염 분류에 부합하지 못하는 이러한 중첩된 양상의 증례들은 “polyangiitis overlap syndrome”이라는 별도의 임상증후군으로 재정립 후 분류하고 있다.16 Polyangiitis overlap syndrome은 두 가지 이상의 혈관염이 혼재되어 발현되는 질병군으로 정의되며, 가장 흔한 형태가 GPA와 EGPA의 중첩이다.16 두 질환의 여러 특징이 다양한 양상으로 조합되어 나타나는데, 특히 본 증례처럼 GPA에 특이적인 cANCA가 양성이면서, EGPA의 대표적 임상 양상인 천식이나 아토피 같은 알레르기 질환의 동반 없이도 전신 호산구증가증을 보이는 형태가 전형적이다.7-11 현재까지 보고된 polyangiitis overlap syndrome의 증례는 모두 타 장기의 침범을 동반하고 있으나, 본 증례의 경우는 전신 호산구증가증을 보이면서도 안와에만 발생하였으므로 polyangiitis overlap syndrome의 국소형 변이로 볼 수 있으며, 세부적으로는 GPA의 호산구 변종 형태로 생각된다. Polyangiitis overlap syndrome의 다른 특징은 천식이나 아토피 같은 알레르기 질환의 존재 없이도, 전신 호산구뿐만 아니라 IgE까지 동반 상승(11-38%)을 보이는 점이다.7,8,10,11 GPA의 병인과는 무관한 호산구증가증과 IgE 상승의 원인에 대해서는 아직 그 기전이 명확하게 밝혀지지는 않았으나, 혈관염에 의해 조직 손상이 진행되는 과정에서 특정 물질 혹은 외부 항원에 대한 면역 노출이 발생하고 이에 이차적으로 유발되는 일종의 과민 반응으로 생각되며, polyangiitis overlap syndrome의 잠재적인 병인과 관련성이 있는 것으로 보인다.10,13
일반적으로 GPA는 스테로이드와 면역억제제 병용이 표준 치료법이지만, EGPA는 스테로이드 단독 치료만으로도 치유가 잘 되는 것으로 알려져 있다.16 본 증례의 환자는 통상적인 GPA와는 달리 스테로이드 단독 치료만으로도 내사시와 상사시 및 안구운동 제한, 눈꺼풀부종 등의 임상 증상 호전과 cANCA 음전, 재발 및 전신 침범 없이 2년 이상의 완전 관해를 보였다. 이렇게 스테로이드 단독 치료만으로도 좋은 장기 치료 효과를 보인 점은 EGPA 발병 기전과 유사한 과민반응 혹은 알레르기반응과 연관된 잠재적인 병인을 공유하고 있을 가능성이 높다. 또한 기존에 발표된 polyangiitis overlap syndrome 증례들은 폐 또는 신장 등 다른 전신 장기를 침범한 경우로 전신형의 양상을 보여 면역억제제의 추가 투여가 필요한 경우였으나,5 본 증례는 polyangiitis overlap syndrome 중에서도 경미한 형태 즉 전신침범이 없는 국소형 호산구 변종이었기에 초기 스테로이드 단독 투여만으로도 호전이 가능하였던 것이 차이점으로 생각된다.
국내에 처음으로 보고되는 증례로, 안와의 염증이 GPA의 초기 증상이자 유일한 병변으로 발현되면서 혈액검사 및 조직검사를 통해 GPA의 호산구 변종으로 진단되어 polyangiitis overlap syndrome의 국소 변이형으로 확인된 경우였다. 급성 양안 복시를 동반한 안와 염증 환자에서 GPA는 감별진단을 요하는 병인 중 하나로 고려되어야 하며, 적절한 검사를 통해 정확한 진단 및 치료 계획을 수립할 수 있을 것으로 생각한다.
Acknowledgements
This study was presented for “Walsh-in-Asia” of 9th Asian Neuro-Ophthalmology Society Meeting, 2017.
Notes
Conflicts of Interest
The authors have no conflicts to disclose.
References
Biography
임성은 / Sung Eun Im
메리놀병원 안과
Department of Ophthalmology, Maryknoll Medical Center
