발덴스트룀고분자글로불린혈증 환자에서 발생한 양안 과점도증후군 연관 망막병증 1예
Hyperviscosity Syndrome-related Retinopathy in a Patient with Waldenström Macroglobulinemia
Article information
Abstract
목적
발덴스트룀고분자글로불린혈증 환자에서 발생한 양안 과점도증후군 연관 망막병증 1예를 경험하여 이를 보고하고자 한다.
증례요약
77세의 남성 환자가 2개월 전부터 서서히 발생한 양안 시력저하를 주소로 내원하였다. 안저검사에서 광범위한 화염상 망막 출혈, 정맥울혈이 확인되었고, 빛간섭단층촬영에서 황반부종, 빛간섭단층촬영혈관조영술에서 망막의 표층 및 심층모세혈관망의 손상, 큰 맥락막혈관의 확장을 확인할 수 있었다. 양안 황반부종을 동반한 중심망막정맥폐쇄로 진단하고 베바시주맙 주입술 및 후테논낭하트리암시놀론 주입술을 시행하였지만 황반부종은 변화가 없었다. 혈액질환과 관련된 망막병증의 가능성으로 혈액종양내과에 정밀검사를 의뢰한 결과 발덴스트룀고분자글로불린혈증으로 진단되었다. 항암 치료를 시작하면서 양안 망막출혈 및 황반부종은 감소하였고, 6회의 항암 치료 후 양안 망막출혈의 흡수 및 황반부종의 호전을 확인하였고, 빛간섭단층촬영혈관조영술에서 맥락막혈관의 확장도 호전된 것을 확인할 수 있었다.
결론
고령의 환자에서 양안 황반부종을 동반한 중심망막정맥폐쇄의 양상을 보이는 경우, 혈액 질환과 관련된 과점도증후군 연관 망막병증의 가능성에 대한 전신적인 검사가 필요하다.
Trans Abstract
Purpose
We report a case of retinopathy related to bilateral hyperviscosity syndrome in a patient with Waldenström macroglobulinemia.
Case summary
A 77-year-old male presented with reduced visual acuities of both eyes 2 months in duration. Fundus examination revealed extensive flame-shaped retinal hemorrhages and venous congestion. Optical coherence tomography (OCT) evidenced macular edema and OCT angiography (OCTA) indicated damage to the superficial and deep capillary plexi of retina and choriocapillaris and dilated large choroidal vessels. We diagnosed central retinal vein occlusion with macular edema and prescribed intravitreal bevacizumab and posterior subtenon triamcinolone injections, however, the edema did not improve. As retinopathy associated with hematological disease was thus suspected, we referred the patient to our department of hematology and oncology for further assessment. He was diagnosed with Waldenström macroglobulinemia. After initiation of chemotherapy, the retinal hemorrhage in and macular edema of both eyes decreased. After six chemotherapy cycles, the retinal hemorrhages resolved and the macular edema improved in both eyes. OCTA revealed that the choroidal vessel dilation also improved.
Conclusions
In elderly patients presenting with central retinal vein occlusions and macular edema of both eyes, it is important to assess whether the retinopathy is associated with a hyperviscosity syndrome linked to a hematological disease.
발덴스트룀고분자글로불린혈증은 림프구증식성 B세포 장애로 단클론성항체 immunoglobulin M (IgM)의 과생성을 보이는 질환이다.1 전신에 이차적으로 과점도증후군을 유발하며, 안과적으로는 과점도증후군 연관 망막병증을 나타낸다. IgM의 과형성은 크게 3가지 범주의 임상 양상을 나타내는데, 두통, 메스꺼움, 어지러움 및 현훈, 감각 이상 및 드물게는 혼수상태를 유발하는 등의 신경학적 증상과 식욕감퇴 및 체중저하, 피로감 악화와 같은 전신적인 증상 그리고 울혈성 심부전, 장 및 구강점막의 출혈, 비출혈, 시신경유두부종, 망막정맥의 확장, 망막병증에 의한 시력저하 등 혈관의 문제를 나타낸다.2 발덴스트룀고분자글로불린혈증의 유병률은 한 해에 백만 명당 4명 정도이며,1 이 질환에 의해 혈장의 과점도로 인해 중심망막정맥폐쇄가 발생한 사례들이 드물게 보고되었다. 저자들은 발덴스트룀고분자글로불린혈증 환자에서 발생한 황반부종을 동반한 양안 과점도증후군 연관 망막병증 환자가 항암 치료 후 호전된 증례를 경험하였으며, 또한 항암 치료 전과 후의 빛간섭단층촬영(optical coherence tomography, OCT) 및 빛간섭단층촬영혈관조영술(OCT angiography, OCTA)의 변화를 확인하였기에 이를 보고하고자 한다.
증례보고
본 연구는 경북대학교병원 임상연구심의위원회(Institutional Review Board, IRB)의 승인(승인 번호 : 2022-12-014)을 받아 진행되었고, 헬싱키선언(Declaration of Helsinki)을 준수하였다.
77세의 남성 환자가 약 2개월 전부터 서서히 발생한 양안 시력저하를 주소로 내원하였다. 당시에 환자는 3개월 전부터 지속적인 비출혈 및 빈혈로 본원 혈액종양내과에서 골수형성이상증후군으로 치료 중인 상태였다. 초진 당시 최대교정시력은 양안 0.6으로 측정되었고 안압은 우안 14 mmHg, 좌안 13 mmHg로 확인되었다. 세극등현미경검사에서 양안 특이 소견은 없었으나, 안저검사에서 광범위한 화염상 망막출혈, 정맥울혈이 확인되었고, 빛간섭단층촬영에서 양안에 망막하액 및 망막내액을 동반한 황반부종이 관찰되었다. 형광안저혈관촬영(fluorescein angiography)에서는 망막정맥의 구불거림 및 울혈, 망막혈관의 형광충만지연, 다발성의 산발된 양상의 과형광점이 관찰되었으나, 형광 누출은 확인되지 않았다(Fig. 1). 빛간섭단층촬영혈관조영술 촬영기(ZEISS CIRRUS 6000 AngioPlex, Carl Zeiss Meditec, Dublin, CA, USA)를 이용하여 황반부에 6×6 mm 구역의 표층 및 심층모세혈관망, 맥락막모세혈관, 할러층(Haller layer)의 큰 맥락막혈관(large choroidal vessel)을 확인하였다. 시행한 빛간섭단층촬영혈관조영술에서 표층 및 심층모세혈관망과 맥락막모세혈관의 손상 및 큰 맥락막혈관의 확장이 관찰되었다(Fig. 2). 양안 황반부종을 동반한 중심망막정맥 폐쇄로 진단하고 유리체 내의 베바시주맙(Avastin®, Genetech, San Francisco, CA, USA) 주입술 및 후테논낭하 트리암시놀론 주입술을 시행하였지만 3주 후 시행한 빛간섭단층촬영에서 황반부종은 변화가 없었다. 혈액 질환과 관련된 망막병증의 가능성을 고려하여 본원 혈액종양내과에 정밀검사를 의뢰하였고, 혈액종양내과에서 시행한 혈액검사 결과에서 혈색소수치 8.7 g/dL로 빈혈이 확인되었으며, 말초혈액도말검사에서 적혈구염주(rouleaux formation) 및 적혈구 부동증(anisocytosis)이 관찰되었다. 소변의 단백질 전기영동검사에서 M-spike (β region) 52.3%(정상≤0.0), M-spike (γ region) 7.5%(정상≤0.0)가 검출되어 단백뇨를 보였으며, 단클론성 감마병증(monoclonal gammopathy)의 양상이 관찰되었다. 또한 혈장에서 면역글로불린M (IgM)이 3,300 mg/dL 이상(정상 50-300 mg/dL)으로 높은 수치가 확인되어 골수생검을 시행하였다. 골수생검 결과에서 림프형질세포성 림프구(lymphoplasmacytic lymphocyte)의 증가 소견이 확인되어 발덴스트룀고분자글로불린혈증으로 진단되었다. 진단 후 혈액종양내과에서 rituximab-bendamustine 항암요법을 시작하면서 경과 관찰하였다. 2회의 항암 치료 후 최대교정시력은 우안 0.9, 좌안 0.5로 우안 시력이 호전되었고, 빛간섭단층촬영에서 양안 황반부종 및 망막하액이 일부 감소된 소견이 관찰되었으며 안저검사에서 양안 망막 출혈이 일부 소실되었다. 6회의 항암 치료 이후 최대교정시력은 우안 0.9, 좌안 0.7로 양안 시력이 호전되었고 안저검사에서 양안 망막출혈은 소실되었으며 빛간섭단층촬영에서 황반부종 또한 감소하였다(Fig. 3). 빛간섭단층촬영혈관조영술에서 표층 및 심층모세혈관과 맥락막모세혈관의 손상이 감소되었으며, 큰 맥락막혈관의 확장도 일부 호전된 것을 확인할 수 있었다(Fig. 4). 혈액검사에서도 혈색소는 13.4 g/dL, 말초혈액도말검사에서 적혈구염주 및 적혈구부동증이 소실되었으며, 면역글로불린M (IgM)도 2,251 mg/dL로 항암 치료 전과 비교하여 감소한 것이 확인되었다. 현재 환자는 항암 치료 이후 발덴스트룀고분자글로불린혈증의 재발 없이 안정된 상태를 유지 중이다.
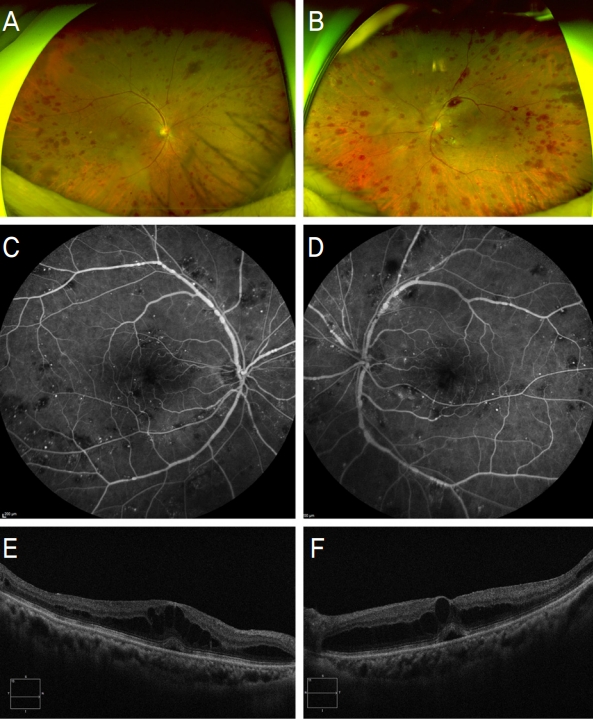
Wide-field fundus photography, fluorescein angiography and optical coherence tomography at initial visit. The initial ultra-wide field fundus photographs show multiple flame-shaped retinal hemorrhages and dilated retinal vessels in right eye (A) and left eye (B). Fluorescein angiography shows tortuous retinal vein with congestions and diffuse punctuate hyperfluorescence with blockage of fluorescein staining disc leakage in right eye (C) and left eye (D). Optical coherence tomographic images show serous retinal detachment with macular edema in right eye (E) and left eye (F).
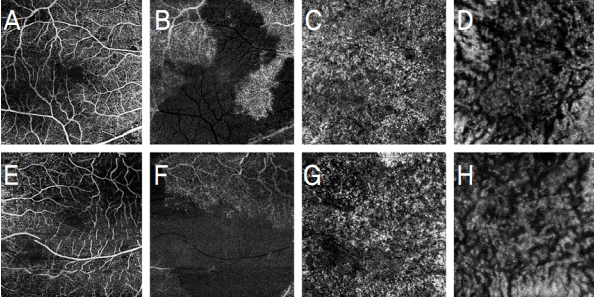
Optical coherence tomography angiography of the right eye (A-D) and left eye (E-H) at initial visit. The initial optical coherence tomography angiography shows damage of superficial (A, E) and deep capillary plexus (B, F) of retina and damaged choriocapillaris (C, G) and dilated large choroidal vessels (D, H) in both eyes.
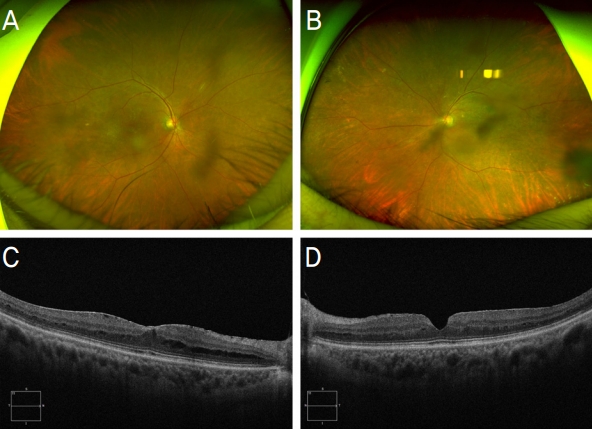
Wide-field fundus photography and optical coherence tomography after 6 cycles of chemotherapy. Wide-field fundus photography shows absorption of dot-blot retinal hemorrhages in right eye (A) and left eye (B) after 6 cycles of chemotherapy. Optical coherence tomography images show the macular edema and subretinal fluid is remaining in both eyes after the injection of the intravitreal bevacizumab in both eyes. After 2 cycles of chemotherapy, the subretinal fluid is absorbed and macular edema is slightly decreased and after 6 cycles of chemotherapy, macular edema is completely absorbed in right eye (C) and left eye (D).
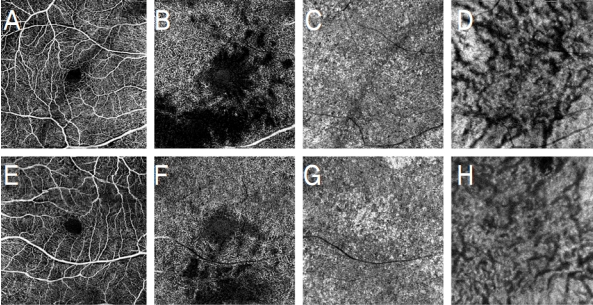
Optical coherence tomography angiography of the right eye (A-D) and left eye (E-H) after 6 cycles of chemotherapy. Optical coherence tomography angiography shows restored vascular density of superficial capillary plexus (A, E) and decreased damage of deep capillary plexus (B, F) of retina and also decreased damage of choriocapillaris (C, G). The dilation of the large choroidal vessels was also restored in right eye (D) and left eye (H).
고 찰
발덴스트룀고분자글로불린혈증은 악성 혈액 질환의 약 2%를 차지하며, 50대 이상에서 인종 및 성별에는 상관없이 발병하는 것으로 알려져 있다. 이 질환으로 인하여 단클론성항체인 면역글로불린M이 과생성되면 말초 혈액도말검사에서 적혈구들의 응집체인 적혈구염주가 관찰되며, 면역글로불린M이 혈액 내의 다양한 성분들과 결합함으로써 이들의 결합체가 부착한 세포의 기능과 생존 능력을 제한하여 백혈구감소증, 혈소판감소증 및 빈혈 등 이차적인 혈액 질환을 유발한다. 또한 면역글로불린M이 과생성되어 발생하는 과점도증후군은 발덴스트룀고분자글로불린혈증 환자의 약 17%에서 보인다. 발덴스트룀고분자글로불린혈증 환자들 중 진단 시 약 8%가 시각의 장애를 보이며 그중 37%에서 과점도증후군 연관 망막병증을 보이는 만큼, 안과적으로 드물게 보고되어 왔다.1,3-6 발덴스트룀고분자글로불린혈증에서 과점도증후군 연관 망막병증은 혈장의 거대글로불린의 농도가 증가하고 면역글로불린M이 오량체(pentamer)를 형성함에 따라 망막으로의 혈류가 감소하고, 순환되는 망막정맥혈관 내 압력이 증가하면서 미세혈관의 정체와 순환장애가 발생하면서 유발된다.7 가장 흔히 보이는 망막 소견은 산발된 양상으로 보이는 출혈 및 미세동맥류, 혈관의 확장과 구불거림의 증가, 시신경유두부종, 망막하액 등이 있다.3,4 한편 Ferreira Santos da Cruz et al7은 다발골수종(multiple myeloma) 환자에서 산발된 양상의 망막출혈과 혈관 구불거림의 증가, 빛간섭단층촬영에서 황반부종을 보이는 과점도증후군 연관 망막병증에 대하여 보고한 바가 있고, 이는 증례의 환자의 망막병증의 특징과 유사한 것을 확인할 수 있었다. 따라서 과점도증후군 연관 망막병증에서는 원인이 되는 전신 질환이 다르더라도 망막병증의 양상은 유사한 것으로 생각된다.
발덴스트룀고분자글로불린혈증 환자의 빛간섭단층촬영 혈관조영술에서는 표층 및 심층모세혈관망의 손상으로 인한 저반사도 증가 및 맥락막혈관의 확장이 관찰되며, 본 증례에서도 이러한 결과를 확인할 수 있었다.8,9 이와 같은 특징적인 소견은 중심망막정맥폐쇄 환자의 빛간섭단층촬영혈관조영술의 소견과 유사한데, 특히 심층모세혈관망의 손상이 두드러지는 특징을 나타낸다.10 이는 표층모세혈관망의 경우 망막동맥과 직접적으로 결합되어 있어 상대적으로 혈액의 관류압이 훨씬 크고 산소 공급이 원활하나, 반면 심층모세혈관망은 주로 정맥 집결로(venous collecting channel)로 구성되어 손상에 취약하기 때문이다.10,11 또한 맥락막모세혈관의 손상 및 큰 맥락막혈관의 확장의 특징적인 소견은 맥락막모세혈관 밀도의 감소가 맥락막의 울혈을 발생시키기 때문이라고 알려져 있다.12 하지만 발덴스트룀고분자글로불린혈증에서 망막혈관의 혈류는 중심망막정맥폐쇄만큼 감소하지 않는다는 것이 큰 차이점으로 알려져 있다. 그리고 중심망막정맥폐쇄 환자에서 표층모세혈관망의 망막중심오목무혈관부위(foveal avascular zone) 영역의 증가가 관찰되지만, 발덴스트룀고분자글로불린혈증 환자에서는 뚜렷한 증가가 관찰되지 않았다는 특징적인 차이가 있다.10 반면 Leskov et al13은 발덴스트룀고분자글로불린혈증 환자에서 시행한 빛간섭단층촬영혈관조영술에서 망막 및 맥락막혈관의 이상 소견은 관찰되지 않았다고 보고하였다. 이와 같은 검사 결과의 차이는 같은 발덴스트룀고분자글로불린혈증이라도 혈장 점도와 그에 따른 망막의 허혈 정도 등에 따라 망막 및 혈관에 미치는 영향이 달라짐으로써 안과적 임상 양상이 다르게 나타난 것으로 추정할 수 있다.2
발덴스트룀고분자글로불린혈증 환자에서 시행한 형광안저혈관조영술에서는 비관류 영역이 관찰되지 않고, 그 대신 망막의 주변부 혈관의 누출을 보인다는 점도 중심망막정맥폐쇄와 구분된다. 중심망막정맥폐쇄에서 발생하는 망막의 저산소증은 혈관내피성장인자(vascular endothelial growth factor) 및 interleukin-6의 상향조절(upregulation)을 일으켜 혈액-망막장벽(blood-retina barrier)을 파괴하고 그 투과성을 증가시킴으로써 망막의 비관류와 망막허혈을 유발하고, 황반부종을 악화시킨다. 이와 같은 기전은 발덴스트룀고분자글로불린혈증에서 망막의 비관류가 보이지 않는 점과 구별된다는 것을 알 수 있다.14
발덴스트룀고분자글로불린혈증에서 유발된 혈장의 과점도는 드물게 장액성 황반박리를 유발하기도 한다. 하지만 이때 동반되는 망막하액은 형광안저혈관촬영에서 플루오레신형광의 누출이 보이지 않는 “silent macula”를 보인다. “silent macula”의 발생에 대한 기전은 완전히 밝혀지지 않았으나, 체내의 면역글로불린M의 상승된 수치가 지속되는 것과 연관이 있을 수 있다는 보고가 있다. 높은 수치의 면역글로불린M에 의해 발생한 국소적인 망막의 허혈 상태는 외망막(outer retina)의 결함을 유발할 수 있으며, 이로 인해 면역글로불린M이 망막하 공간으로 누출됨으로써 삼투압 차이가 발생하면서 그 결과 망막부종 및 망막하액이 발생하는 것이다. 이와 같은 기전은 높은 면역글로불린M 수치가 장액성 황반박리의 병태생리에 있어 중요한 역할을 한다는 점을 시사한다. 따라서 과점도증후군에 의한 망막병증에서 항암요법이나 혈장교환술(plasampheresis) 등을 통해 면역글로불린M의 수치를 정상화하는 것이 망막부종 및 망막하액 감소에 효과가 있을 것으로 생각된다.5,15
환자는 빛간섭단층촬영에서 망막하액을 동반한 장액성 황반박리가 확인되었다. 이에 대해 후테논낭하 트리암시놀론 주입술과 유리체 내 베바시주맙 주입술을 시행하였음에도 불구하고 황반부종 및 망막하액의 감소에 큰 효과가 없었다. 하지만 항암요법을 완료한 이후 혈액학적인 이상 소견이 정상화되고 면역글로불린M 수치가 감소함에 따라 빛간섭단층촬영에서 황반부종 및 망막하액이 모두 소실된 것이 확인되었다. 또한 빛간섭단층혈관조영술에서 망막의 손상된 표층 및 심층모세혈관망과 맥락막모세혈관이 회복되었고 큰 맥락막혈관의 확장도 호전되었다. 이처럼 발덴스트룀고분자글로불린혈증에 따른 과점도증후군 연관 망막병증은 망막정맥폐쇄 또는 당뇨망막병증 등의 다른 안과적 질환에서 동반되는 망막하액의 발생 기전과 차이가 있기 때문에, 유리체 내 주입술 등의 안과적 치료에 대한 효과가 떨어지는 반면 기저 질환의 치료가 망막하액의 흡수에 중요한 역할을 하였음을 알 수 있었다.
따라서 혈액학적 기저 질환이 있는 환자가 양안의 시력 저하를 호소하여 내원한다면 전신 질환에 의한 망막병증을 고려하여 내과적 검사를 시행해야 하며, 적절한 내과적 치료를 통하여 혈액학적 교정을 함으로써 망막병증을 호전시킬 수 있을 것으로 생각된다. 특히 형광안저혈관촬영에서 플루오레신형광의 누출이 없는 장액성 황반박리가 관찰된다면 면역글로불린 수치를 확인해보는 것이 진단에 도움이 될 수 있을 것으로 생각된다.5 또한 본 증례에서 빛간섭단층촬영혈관조영술을 시행함으로써 과점도증후군 연관 망막병증에서의 특징적인 망막 및 맥락막혈관의 변화를 확인할 수 있었다. 이와 같은 과점도증후군 연관 망막병증 환자에서 빛간섭단층촬영혈관조영술을 통해 망막 및 맥락막혈관의 변화를 확인하는 것이 진단과 더불어 경과 관찰에 도움이 될 수 있을 것으로 사료된다.
Acknowledgements
This work was supported by the Biomedical Research Institute grant, Kyungpook National University Hospital (2019).
Notes
Conflicts of Interest
The authors have no conflicts to disclose.
References
Biography
이혜진 / Hye Jin Lee
경북대학교 의과대학 안과학교실
Department of Ophthalmology, School of Medicine, Kyungpook National University
