

2019ļģäņŚÉ ļ░£ņāØĒĢśņŚ¼, Ēśäņ×¼Ļ╣īņ¦ĆļÅä ņżæļīĆĒĢ£ ĒīīņןņØä ļČłļ¤¼ņśżĻ│Ā ņ׳ļŖö Severe Acute Respiratory Syndrome-Coronavirus-2 (SARSCoV-2)ļŖö ļåÆņØĆ Ļ░ÉņŚ╝ļźĀ(infectivity)ņØä ļ│┤ņØ┤ļ®░, ĒśĖĒØĪĻĖ░ ņÖĖņŚÉļÅä ņŗĀĻ▓ĮĻ│ä ņ¦łĒÖś, ņŗ¼ĒśłĻ┤ĆĻ│ä ņ¦łĒÖś, ĒśłņĢĪĒĢÖņĀü ņØ┤ņāü, ņåīĒÖöĻĖ░ ļ░Å ļé┤ļČäļ╣äĻ│äņŚÉ Ļ▒Ėņ│Éņä£ ņ¦üņĀæ ļśÉļŖö Ļ░äņĀæņĀüņ£╝ļĪ£ ĒĢ®ļ│æņ”ØņØä ņĢ╝ĻĖ░ĒĢ£ļŗżĻ│Ā ļ│┤Ļ│ĀļÉśņŚłļŗż.1
SARS-CoV-2ļŖö ņĢłņ¦ĆņśżĒģÉņŗĀņĀäĒÖśĒÜ©ņåī-2 (angiotensin converting enzyme-2, ACE-2) ņłśņÜ®ņ▓┤ļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ ņØĖĻ░äņäĖĒżņŚÉ ņ╣©Ēł¼ĒĢ£ļŗżĻ│Ā ņĢīļĀżņĀĖ ņ׳ņ£╝ļ®░, ņØ┤ ņłśņÜ®ņ▓┤Ļ░Ć ĒÆŹļČĆĒĢśĻ▓ī ļ░£ĒśäļÉśņ¢┤ ņ׳ļŖö ĒśłĻ┤Ćļé┤Ēö╝ņäĖĒżņŚÉ ņ╣©Ēł¼ĒĢśņŚ¼, ļé┤Ēö╝ņäĖĒżņØś ņŚ╝ņ”Ø ļ░Å ĻĖ░ļŖźļČĆņĀä(endothelial dysfunction)ņØä ņ£Āļ░£ĒĢśļŖö Ļ▓āņØ┤ COVID-19 Ļ░ÉņŚ╝ņ”ØņØś ņŻ╝ņÜö ļ│æņØĖņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż.1
SARS-CoV-2 ļ░öņØ┤ļ¤¼ņŖżņÖĆ Ļ┤ĆļĀ©ļÉ£ ĒØöĒĢ£ ņĢłĻĄ¼ ĒĢ®ļ│æņ”Øņ£╝ļĪ£ļŖö 7.6%ņŚÉņä£ Ļ▓░ļ¦ēņČ®ĒśłņØ┤ ļÅÖļ░śļÉśņŚłļŗżĻ│Ā ĒĢśļ®░, COVID-19 ņ”ØņāüņØ┤ ņŗ¼ĒĢĀņłśļĪØ ņĢłĻĄ¼ ĒĢ®ļ│æņ”Ø Ļ░ĆļŖźņä▒ņØ┤ ļåÆļŗżĻ│Ā ņĢīļĀżņĀĖ ņ׳ļŗż.2 ņØ┤ļ¤¼ĒĢ£ ņĢłĻ│╝ņĀü ĒĢ®ļ│æņ”ØņØĆ ņé¼ļ×īņØś Ļ░üļ¦ē ļ░Å Ļ▓░ļ¦ēņŚÉ ļåÆĻ▓ī ļ░£ĒśäļÉśņ¢┤ ņ׳ļŖö ACE-2 ņłśņÜ®ņ▓┤ļĪ£ ņäżļ¬ģĒĢĀ ņłś ņ׳ļŗż.3 ņŗżņĀ£ļĪ£ ĒÖśņ×ÉņØś Ļ▓░ļ¦ē swabņØä ņŗ£Ē¢ēĒĢśņśĆņØä ļĢī, ĒÖśņ×ÉņØś 3.9%ņŚÉņä£ SARSCoV-2 ļ░öņØ┤ļ¤¼ņŖż ņ¢æņä▒ ņåīĻ▓¼ņØä ļ│┤ņśĆņ£╝ļ®░,2 ļ¼┤ņ”Øņāü COVID-19 ĒÖśņ×ÉņØś ļłłļ¼╝ ļ░Å ļ░®ņłś, ņ£Āļ”¼ņ▓┤ņŚÉņä£ļÅä ļ░öņØ┤ļ¤¼ņŖżĻ░Ć Ļ▓ĆņČ£ļÉśņŚłļŗżĻ│Ā ļ│┤Ļ│ĀļÉ£ ļ░ö ņ׳ļŗż.4
ļ│Ė ņ”ØļĪĆņŚÉņä£ļŖö COVID-19 ĒÅÉļĀ┤ ĒÖśņ×ÉņŚÉņä£ ļ░£ņāØĒĢ£ ļŗ©ņĢłņä▒ Ļ░üļ¦ēļé┤Ēö╝ņŚ╝ ļ░Å Ļ│ĀņĢłņĢĢņä▒ ņĢ×ĒżļÅäļ¦ēņŚ╝ņØä Ļ▓ĮĒŚśĒĢśņŚ¼ ņØ┤ļź╝ ĻĄŁļé┤ņŚÉ ņĄ£ņ┤łļĪ£ ļ│┤Ļ│ĀĒĢśĻ│Āņ×É ĒĢ£ļŗż.
ņ”ØļĪĆļ│┤Ļ│Ā
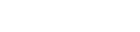
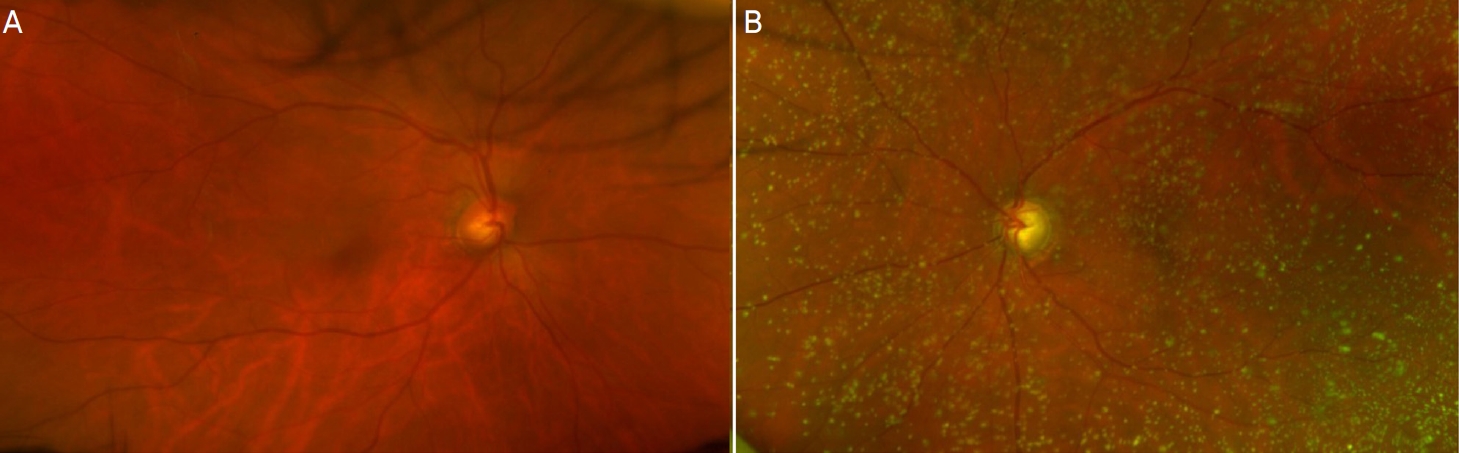
71ņäĖ ļé©ņ×É ĒÖśņ×ÉļĪ£ ļé┤ņøÉ 10ņØ╝ ņĀä SARS-CoV-2 ļ░öņØ┤ļ¤¼ņŖż Ļ░ÉņŚ╝ ĒÖĢņ¦äļ░øņØĆ Ēøä COVID-19 ĒÅÉļĀ┤ņ£╝ļĪ£ ņ×ģņøÉ ņ╣śļŻī ņżæ, ĒÖĢņ¦äļÉ£ 2ņØ╝ ĒøäļČĆĒä░ ņ¦ĆņåŹļÉ£ ņÜ░ņĖĪ ņŗ£ļĀźņĀĆĒĢś, ļłłĒåĄņ”Ø, ļłłĻ║╝ĒÆĆ ļČĆņóģ ļ░Å ļæÉĒåĄņØä ņŻ╝ņåīļĪ£ ļé┤ņøÉĒĢśņśĆļŗż. Ļ│╝Ļ▒░ļĀźņāü ļŗ╣ļć© ļ░Å Ļ│ĀĒśłņĢĢņ£╝ļĪ£ ņĢĮļ¼╝ ļ│ĄņÜ® ņżæņØ┤ņŚłņ£╝ļ®░, 6ļģä ņĀä ņóīņĢł ĒżļÅäļ¦ēņŚ╝ņä▒ ļģ╣ļé┤ņן ņ¦äļŗ©ĒĢś 2% dorzolamide/0.5% timolol (Cosopt┬«, Santen Pharmaceutical Co.,Ltd., Seoul, Korea), 0.15% brimonidine tartrate (Alphagan┬«, Allergan Korea Ltd., Seoul, Korea)ļź╝ ņĀÉņĢłĒĢśļŗżĻ░Ć Ļ▓ĮĻ│╝ Ļ┤Ćņ░░ņØ┤ ņżæļŗ©ļÉśņŚłļŹś ĻĖ░ņÖĢļĀźņØ┤ ņ׳ņŚłļŗż. 2016ļģä ļ¦łņ¦Ćļ¦ē ņ¦äļŻī ļŗ╣ņŗ£ ņÜ░ņĢł ļéśņĢłņŗ£ļĀź 1.0, ņóīņĢł ļéśņĢłņŗ£ļĀź 0.8ņØ┤ņŚłņ£╝ļ®░, ņĀäļ░®ņØś ņŚ╝ņ”ØņØĆ ņŚåņŚłĻ│Ā, Ļ░üļ¦ēļé┤Ēö╝ņäĖĒżļ░ĆļÅäļŖö ņÜ░ņĢł 2,324 cells/mm2 , ņóīņĢł 2,544 cells/mm2ļĪ£ ĒŖ╣ņØ┤ ņåīĻ▓¼ņØĆ ņŚåņŚłļŗż(Fig. 1A).
ļé┤ņøÉ ņŗ£ ņĢłĻ│╝Ļ▓Ćņé¼ņāü ļéśņĢłņŗ£ļĀźņØĆ ņÜ░ņĢł 0.04, ņóīņĢł 0.15ņśĆĻ│Ā ņ¢æņĢł ļ¬©ļæÉ ĻĄÉņĀĢļÉśņ¦Ć ņĢŖņĢśņ£╝ļ®░, ļ╣äņĀæņ┤ēņä▒ ņĢłņĢĢĻ│äĻ▓Ćņé¼ņŚÉņä£ ņÜ░ņĢł 16.2 mmHg, ņóīņĢł 19.2 mmHgļĪ£ ņĖĪņĀĢļÉśņŚłļŗż.
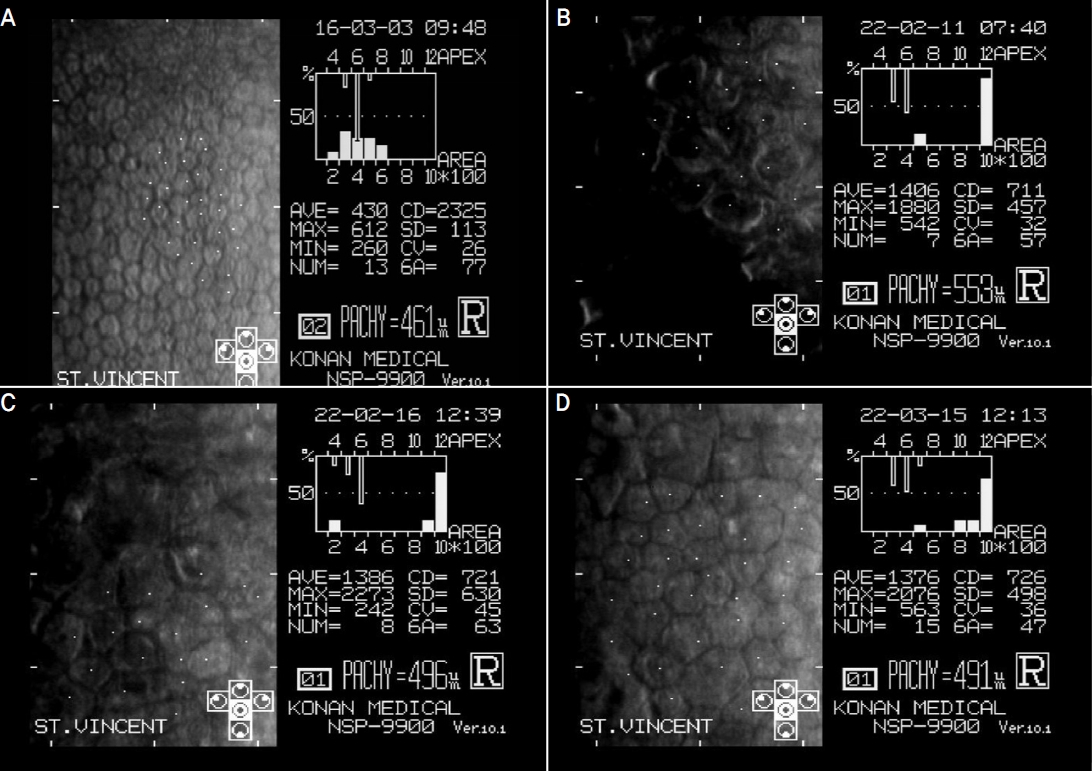
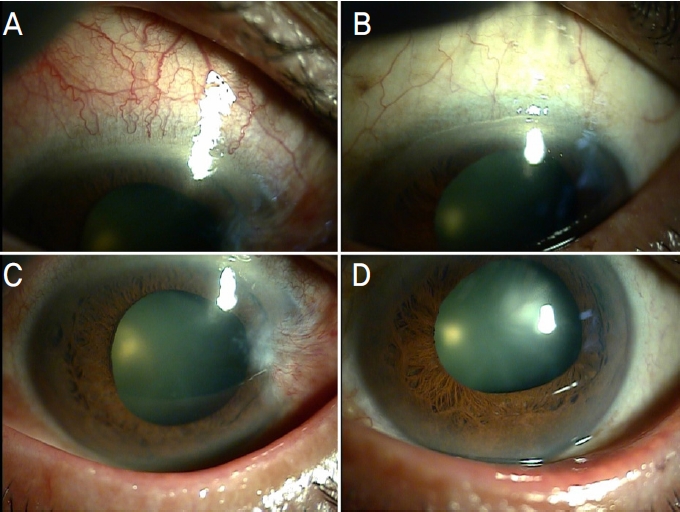
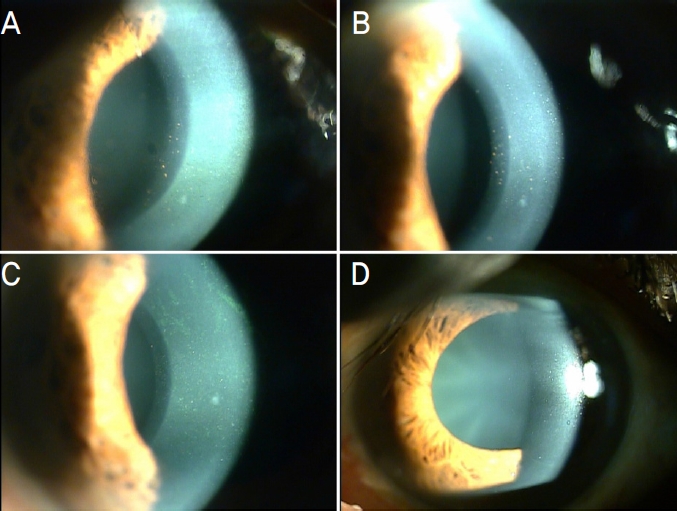
ņÜ░ņĖĪ ņĢłĻ▓ĆņØś Ļ▓ĮĒĢ£ ļČĆņóģĻ│╝ ĒĢ©Ļ╗ś ņäĖĻĘ╣ļō▒Ēśäļ»ĖĻ▓ĮĻ▓Ćņé¼ņāü ņóīņĢłņŚÉ ļ╣äĒĢśņŚ¼ ņÜ░ņĢł Ļ▓░ļ¦ēņØ┤ ņŗ¼ĒĢśĻ▓ī ņČ®ĒśłļÉśņ¢┤ ņ׳ņŚłņ£╝ļ®░(Fig. 2A, B), ņāüņĖĪņØś Ļ░üļ¦ēļČĆņóģĻ│╝ ņØ┤ņŚÉ ļÅÖļ░śļÉ£ ļŹ░ņŖżļ®öļ¦ē ņĀæĒלņØ┤ ĒÖĢņØĖļÉśņŚłļŗż(Fig. 3A). Ļ░üļ¦ēĒøäļ®┤ņ╣©ņ░®ļ¼╝ņØ┤ Ļ░üļ¦ēļé┤Ēö╝ ņĀäļ░śņŚÉ Ļ▒Ėņ│É Ļ┤Ćņ░░ļÉśņŚłņ£╝ļ®░, ņĀäļ░®ņŚ╝ņ”ØņäĖĒż 1+ļĪ£ Ļ▓ĮĒĢ£ ņŚ╝ņ”ØņØä ļ│┤ņśĆļŗż. ņ¢æņĢłņØś ļÅÖĻ│ĄņØĆ ņżæļō▒ļÅäļĪ£ ņé░ļÅÖļÉśņ¢┤ ņ׳ņŚłņ£╝ļ®░ ļÅÖĻ│Ąļ░śņé¼ļŖö Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśļŗż(Fig 2C, D). ņĢłņĀĆĻ▓Ćņé¼ņāü Ļ░üļ¦ēļČĆņóģņ£╝ļĪ£ ņØĖĒĢśņŚ¼ ĒØÉļ”¼Ļ▓ī ļ│┤ņśĆņ£╝ļéś, ņĀĆļ¬ģĒĢ£ ņŚ╝ņ”Ø ņåīĻ▓¼ņØĆ Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśļŗż. ņØ┤ņŚÉ ņÜ░ņĢł ņĢ×ĒżļÅäļ¦ēņŚ╝ ļ░Å Ļ░üļ¦ēļé┤Ēö╝ņäĖĒżņŚ╝ ņ¦äļŗ©ĒĢś ņÜ░ņĢł 0.5% levofloxacin hydrate (Cravit┬«, Santen Pharmaceutical Korea Co., Ltd., Seoul, Korea) 4ĒÜī, 1% prednisolone acetate (Predbell┬«, Chong Kun Dang Pharmaceutical, Seoul, Korea) 2ņŗ£Ļ░ä Ļ░äĻ▓®, Cosopt┬« 2ĒÜī ņĀÉņĢłĒĢśļÅäļĪØ ĒĢśņśĆļŗż.
2ņØ╝ Ēøä ņŗ£Ē¢ēĒĢ£ Ļ▓Ćņé¼ņāü ņŗ£ļĀźņØĆ Ļ│äņåŹ ņĀĆĒĢśļÉ£ ņāüĒā£ņśĆņ£╝ļ®░, ļ╣äņĀæņ┤ēņä▒ ņĢłņĢĢĻ│äĻ▓Ćņé¼ņŚÉņä£ ņÜ░ņĢłņØś ņĢłņĢĢņØĆ 16 mmHgļĪ£ ņĖĪņĀĢļÉśņŚłļŗż. ņĀäņĢłļČĆĻ▓Ćņé¼ņāü ņÜ░ņĢłņØś Ļ░üļ¦ēĒøäļ®┤ņ╣©ņ░®ļ¼╝ņØ┤ ņ¦ĆņåŹņĀüņ£╝ļĪ£ Ļ┤Ćņ░░ļÉśņŚłĻ│Ā(Fig. 3B), Ļ░üļ¦ē Ļ▓Įļ®┤Ēśäļ»ĖĻ▓ĮĻ▓Ćņé¼ņāü ņÜ░ņĢł Ļ░üļ¦ēļé┤Ēö╝ņäĖĒżļ░ĆļÅäĻ░Ć 711 cells/mm2ļĪ£ 6ļģäņĀä ļ¦łņ¦Ćļ¦ē Ļ▓Ćņé¼ņŚÉ ļ╣äĒĢśņŚ¼ ĒśäņĀĆĒ׳ Ļ░ÉņåīļÉśĻ│Ā Ļ░üļ¦ēļæÉĻ╗śĻ░Ć ņ”ØĻ░ĆĒĢśņśĆņ£╝ļ®░(Fig. 1B), ņ¢┤ļæÉņÜ┤ ņØīņśüņØś ĒĢĄņØä Ļ░Ćņ¦ä ņäĖĒż ļ░Å ņĀäļ░śņĀüņ£╝ļĪ£ ņäĖĒżņØś Ēü¼ĻĖ░Ļ░Ć ņ╗żņ¦ä ņåīĻ▓¼ņØ┤ Ļ┤Ćņ░░ļÉśņŚłļŗż(Fig. 1B). ņóīņĢł Ļ░üļ¦ēļé┤Ēö╝ņäĖĒżĻ▓Ćņé¼ Ļ▓░Ļ│╝ ņłśņÖĆ ļ¬©ņ¢æņØ┤ ņĀĢņāü ļ▓öņ£äņŚÉ ņåŹĒĢśņśĆļŗż.
5ņØ╝ Ēøä ņČöņĀü Ļ┤Ćņ░░ ņŗ£ ņÜ░ņĢł ļéśņĢłņŗ£ļĀź 0.3ņ£╝ļĪ£ ĒśĖņĀäļÉśņŚłņ£╝ļéś ĻĄÉņĀĢļÉśņ¦Ć ņĢŖņĢśņ£╝ļ®░, ņÜ░ņĢł ņĢłņĢĢņØĆ 28 mmHgĻ╣īņ¦Ć ņāüņŖ╣ĒĢśņśĆļŗż. Ļ░üļ¦ē Ļ▓Įļ®┤Ēśäļ»ĖĻ▓ĮĻ▓Ćņé¼ņāü ņ¢┤ļæÉņÜ┤ ņØīņśüņØś ĒĢĄņØä Ļ░Ćņ¦ä ņäĖĒżĻ░Ć ņĪ░ĻĖł ļŹö ņżäņ¢┤ļō£ļŖö ņåīĻ▓¼ņØä ļ│┤ņśĆĻ│Ā Ļ░üļ¦ēļæÉĻ╗śļÅä ļ│┤ļŗż Ļ░ÉņåīĒĢśņśĆļŗż(Fig. 1C). ņĢłņĀĆĻ▓Ćņé¼ņāü ļÆżĒżļÅäļ¦ēņŚ╝ ņåīĻ▓¼ņØĆ Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśļŗż(Fig. 4). ņØ┤ņŚÉ ņÜ░ņĢł Ļ░üļ¦ēļé┤Ēö╝ņŚ╝(endotheliitis of cornea) ļ░Å Ļ│ĀņĢłņĢĢņä▒ ņĢ×ĒżļÅäļ¦ēņŚ╝(hypertensive anterior uveitis)ņ£╝ļĪ£ ņ¦äļŗ©ĒĢś, ņøÉņØĖ Ļ░Éļ│äņØä ņ£äĒĢśņŚ¼ ņĀäļ░®ņ▓£ņ×Éļź╝ ņŗ£Ē¢ēĒĢśņŚ¼ ļ░®ņłśļź╝ ņ▒äņĘ©ĒĢ£ Ēøä Ļ▒░ļīĆņäĖĒżļ░öņØ┤ļ¤¼ņŖż(cytomegalovirus)ņŚÉ ļīĆĒĢ£ polymerase chain reaction (PCR) Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢśņśĆņ£╝ļ®░, Ļ▓░Ļ│╝ļŖö ņØīņä▒ņ£╝ļĪ£ ĒÖĢņØĖļÉśņŚłļŗż. ņĢłņĢĢ ņĪ░ņĀłņØä ņ£äĒĢśņŚ¼ Alphagan┬«(Allergan Korea Ltd.) ļ░Å 0.005% latanoprost (Xalatan┬«, Viatris Korea, Seoul, Korea)ļź╝ ņČöĻ░ĆĒĢśņśĆļŗż.
1ļŗ¼ Ēøä ņÜ░ņĢł ļéśņĢłņŗ£ļĀźņØĆ 0.5Ļ╣īņ¦Ć ĒÜīļ│ĄļÉśņŚłņ£╝ļ®░, ļŹ░ņŖżļ®öļ¦ē ņĀæĒל ļ░Å Ļ░üļ¦ēĒøäļ®┤ņ╣©ņ░®ļ¼╝ņØ┤ ņĀÉņ░© ĒśĖņĀäļÉśņŚłļŗż(Fig. 3C). Cosopt┬« (Santen Pharmaceutical Korea Co., Ltd) ļ░Å Alphagan┬« (Allergan Korea Ltd.)ņØä ņé¼ņÜ®ĒĢśļ®░ ņĢłņĢĢņØĆ 21 mmHgļĪ£ ņ£Āņ¦ĆļÉśņŚłĻ│Ā, Ļ░üļ¦ēļé┤Ēö╝ņäĖĒżļ░ĆļÅäļŖö 726 cells/mm2ļĪ£ ņŚ¼ņĀäĒ׳ Ļ░ÉņåīļÉśņ¢┤ ņ׳ņŚłņ£╝ļéś, ņ¢┤ļæÉņÜ┤ ņØīņśüņØś ĒĢĄņØä Ļ░Ćņ¦ä ņäĖĒżĻ░Ć Ļ▒░ņØś ņŚåņ¢┤ņ¦ĆĻ│Ā, Ļ░üļ¦ēļé┤Ēö╝ņäĖĒżņØś Ļ▓ĮĻ│äĻ░Ć ļ¬ģĒÖĢĒĢ┤ņ¦ĆļŖö ņ¢æņāüņØä ļ│┤ņśĆļŗż(Fig. 1D). ņØ┤ņŚÉ Predbell┬« (Chong Kun Dang Pharmaceutical) ņĀÉņĢł Ēܤņłśļź╝ 2ņŗ£Ļ░ä Ļ░äĻ▓®, 4ĒÜī, 2ĒÜī, 1ĒÜīļĪ£ 2.5Ļ░£ņøöņŚÉ Ļ▒Ėņ│É Ļ░Éļ¤ēĒĢśņśĆļŗż. 4Ļ░£ņøö Ēøä ļŗżņŗ£ ļé┤ņøÉĒĢśņśĆņØä ļĢī ņÜ░ņĢł Ļ░üļ¦ēņØś Ēł¼ļ¬ģņä▒ņØ┤ ĒÜīļ│ĄļÉśĻ│Ā ņĢ×ĒżļÅäļ¦ēņŚ╝ ļ░Å Ļ░üļ¦ēļé┤Ēö╝ņŚ╝ņØ┤ ņ×¼ļ░£ĒĢśņ¦Ć ņĢŖņØīņØä ĒÖĢņØĖĒĢśņśĆļŗż(Fig. 3D). ĻĘĖļ¤¼ļéś ņ¢æņĢłņØś ņżæļō▒ļÅäļĪ£ ņé░ļÅÖļÉ£ ļÅÖĻ│ĄņØĆ ĻĘĖļīĆļĪ£ ņ£Āņ¦ĆļÉśĻ│Ā ņ׳ļŖö ņåīĻ▓¼ņØä ļ│┤ņśĆļŗż.
Ļ│Ā ņ░░
SARS-CoV-2ļ░öņØ┤ļ¤¼ņŖżņØś ņäĖĒżĒæ£ļ®┤ņØś ņłśņÜ®ņ▓┤ ņżæ ĒĢśļéśņØĖ ACE2ļŖö ņĀĢņāüņĀüņ£╝ļĪ£ ĒÅÉ ņĀÉļ¦ē, ņåīĒÖöĻĖ░ ļ░Å Ļ▓░ļ¦ē ļō▒ņŚÉ ņĪ┤ņ×¼ĒĢ£ļŗżĻ│Ā ņĢīļĀżņĪīļŗż.1 ĒŖ╣Ē׳ ņé¼ļ×ī Ļ░üļ¦ēņāüĒö╝ ļ░Å Ļ▓░ļ¦ēņāüĒö╝ņŚÉļŖö ļ░öņØ┤ļ¤¼ņŖżņØś ņ╣©Ēł¼ ļ¦żĻ░£ņ▓┤Ļ░Ć ļÉśļŖö ACE2ņØś ĒÖ£ņä▒ņØ┤ ļåÆņĢä ņ┤łĻĖ░ Ļ░ÉņŚ╝ Ļ▓ĮļĪ£ļĪ£ņä£ ļ░öņØ┤ļ¤¼ņŖżĻ░Ć Ļ░üļ¦ēĒæ£ļ®┤ņØä ĒåĄĒĢ┤ ņ╣©Ēł¼ĒĢĀ Ļ░ĆļŖźņä▒ļÅä ņĀ£ĻĖ░ļÉśņŚłļŗż.3
Zhou et al3ņØĆ ņĀĢņāü ņĢłĻĄ¼ņŚÉņä£ ļ░öņØ┤ļ¤¼ņŖżņØś ņäĖĒż ņłśņÜ®ņ▓┤ņØĖ ACE2 ļ░Å ļ░öņØ┤ļ¤¼ņŖżņÖĆ ACE2ņØś Ļ▓░ĒĢ®ņØä ļÅĢļŖö ĒÜ©ņåīņØĖ transmembrane protease serine subtype 2ņØś ļČäĒżļź╝ ņŚ░ĻĄ¼ĒĢśņśĆņØä ļĢī ļæÉ ļŗ©ļ░▒ņ¦ł ļ¬©ļæÉ Ļ░üļ¦ēņāüĒö╝ņäĖĒżņÖĆ ļÅÖņØ╝ĒĢ£ Ļ░ĢļÅäļĪ£ Ļ░üļ¦ēļé┤Ēö╝ņäĖĒżņŚÉņä£ļÅä ļ░£ĒśäļÉ©ņØä ļ│┤Ļ│ĀĒĢśņśĆļŗż. Sawant et al5ņØĆ COVID-19 ĒÖśņ×ÉņØś ņé¼Ēøä ņĢłĻĄ¼ņŚÉņä£ SARS-CoV-2ņŚÉ ļīĆĒĢ£ PCR Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢśņśĆņØä ļĢī, ļ░öņØ┤ļ¤¼ņŖż RNAĻ░Ć Ļ░Ćņן ĒØöĒ׳ ļ░£Ļ▓¼ļÉśļŖö ņĪ░ņ¦üņØĆ Ļ░üļ¦ēĒøäļ®┤ņØ┤ļØ╝Ļ│Ā ļ│┤Ļ│ĀĒĢśņśĆļŗż. ļśÉĒĢ£ COVID-19ņØś ĻĖ░ņÖĢļĀźņØ┤ ņ׳ļŹś ĒÖśņ×ÉņØś Ļ▓░ļ¦ē ļ░Å ņä¼ņ£ĀņŻ╝ņäĖĒż, ĒÖŹņ▒äņŚÉņä£ SARS-CoV-2ļŗ©ļ░▒ņ¦łņØ┤ ļ░£Ļ▓¼ļÉśņŚłļŗż.6
ņŗżņĀ£ļĪ£ COVID-19 ĒÖśņ×ÉļōżņŚÉņä£ Ļ░üļ¦ēļé┤Ēö╝ņäĖĒżļź╝ Ļ┤Ćņ░░ĒĢśņśĆņØä ļĢī, ņĀĢņāüņØĖņŚÉ ļ╣äĒĢśņŚ¼ ņäĖĒż ņłś ļ░Å ņ£ĪĻ░üĒśĢ ņäĖĒżņØś ļ╣äņ£©ņØ┤ ļ¢©ņ¢┤ņĀĖ ņ׳ņŚłļŗż.7 ņŗżņĀ£ ļ¼┤ņ”ØņāüņØś ĒÖśņ×ÉņØś ļ░▒ļé┤ņןņłśņłĀ ņŗ£ ņłśņ¦æĒĢ£ ņĀäļ░® ļ░®ņłśņŚÉņä£ SARS-CoV-2ņŚÉ ļīĆĒĢ£ PCR Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢśņśĆņØä ļĢī ņĢĮ 19%ņŚÉņä£ ļ░öņØ┤ļ¤¼ņŖżĻ░Ć Ļ▓ĆņČ£ļÉśņŚłļŗż.4 ņØ┤ļ¤¼ĒĢ£ Ļ▓░Ļ│╝ļŖö ļ░öņØ┤ļ¤¼ņŖżĻ░Ć ĒśłĒ¢ēņä▒ņ£╝ļĪ£ ĒśłņĢĪ-ļ░®ņłś ņןļ▓ĮņØä ĒåĄĻ│╝ĒĢśņŚ¼ ņĀäļ░®ņŚÉ ņ£Āņ×ģļÉ£ Ēøä ļ®┤ņŚŁĒŖ╣ĻČī ņ¦ĆņŚŁņØĖ ņĀäļ░®ņŚÉņä£ ļ®┤ņŚŁļ░śņØæņ£╝ļĪ£ļČĆĒä░ ļ│┤ĒśĖļÉ©ņ£╝ļĪ£ņŹ©, ņåīļ®ĖļÉśņ¦Ć ņĢŖĻ│Ā ņ¦ĆņåŹņĀüņ£╝ļĪ£ ņĪ┤ņ×¼ĒĢĀ Ļ░ĆļŖźņä▒ņØä ņŗ£ņé¼ĒĢ£ļŗż.
SARS-CoV-2ļŖö ļé┤Ēö╝ņäĖĒżņŚÉ ņ╣©Ēł¼ĒĢśņŚ¼ ļé┤Ēö╝ņäĖĒżņØś ņןļ▓Į ĻĖ░ļŖźņØä ņåīņŗżņŗ£ņ╝£, ļé┤Ēö╝ņäĖĒżņØś ņŚ╝ņ”Ø ļ░Å ĻĘĖļĪ£ ņØĖĒĢ£ ļ¦īņä▒ņĀü ļé┤Ēö╝ņäĖĒż ĻĖ░ļŖźļČĆņĀäņØä ņ£Āļ░£ĒĢśļ®░ ņØ┤ļŖö COVID-19ņØś ņŻ╝ņÜö ļ│æņØĖņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż.1 ļ│Ė ņ”ØļĪĆļŖö Ļ░üļ¦ēļé┤Ēö╝ņäĖĒżņØś ņŚ╝ņ”Ø ļ░Å Ļ▓ĮĒĢ£ ņŚ╝ņ”Ø ļ░Å Ļ│ĀņĢłņĢĢņØä ļ│┤ņśĆļŗż. ņä¼ņ£ĀņŻ╝ņäĖĒżļŖö ņŗĀĻ▓ĮļŖź(neural crest)ņŚÉņä£ ņ£ĀļלĒĢśņśĆņ£╝ļ®░, ļŗżņ¢æĒĢ£ ņäĖĒżņØś ĒŖ╣ņ¦Ģ ņżæ ļé┤Ēö╝ņäĖĒżņØś ĒŖ╣ņ¦ĢņØä ļ│┤ņ£ĀĒĢśĻ│Ā ņ׳ļŗż. ļö░ļØ╝ņä£ ļ░®ņłśņŚÉ ņ╣©ņ×ģĒĢ£ ļ░öņØ┤ļ¤¼ņŖżĻ░Ć Ļ░üļ¦ēļé┤Ēö╝ņäĖĒż ļ░Å ņä¼ņ£ĀņŻ╝ņäĖĒżņŚÉ Ļ░ÉņŚ╝ļÉ©ņ£╝ļĪ£ņŹ© ļ®┤ņŚŁ ņĪ░ņĀł ņןņĢĀ ļ░Å ņŚ╝ņ”Øļ░śņØæņØä ņ£Āļ░£ĒĢśņŚ¼, Ļ░üļ¦ē ĻĖ░ļŖźļČĆņĀä ļ░Å Ļ│ĀņĢłņĢĢņØä ņ£Āļ░£ĒĢśņśĆņØä Ļ░ĆļŖźņä▒ņØ┤ ņ׳ļŗż.
Ļ▒░ļīĆņäĖĒżļ░öņØ┤ļ¤¼ņŖżļŖö Ļ░üļ¦ēļé┤Ēö╝ņäĖĒżņŚ╝ņØä ļÅÖļ░śĒĢśĻ│Ā ĒÖŹņ▒äļź╝ ņ╣©ļ▓öĒĢśļŖö ņĢ×ĒżļÅäļ¦ēņŚ╝ņØś Ļ▓ĮņÜ░ Ļ░Ćņן ĒØöĒĢ£ ņøÉņØĖņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż.8 Mazzotta and Giancipoli9ļŖö COVID-19 ĒÖśņ×ÉņŚÉņä£ ĻĖ░ņĪ┤ ĒżļÅäļ¦ēņŚ╝ņØś ņ×¼ļ░£ņØä ļ│┤Ļ│ĀĒĢ£ ļ░ö ņ׳ļŗż. ļśÉĒĢ£ ĒŚżļź┤ĒÄśņŖżļ░öņØ┤ļ¤¼ņŖżĻ│╝ņØś ļ░öņØ┤ļ¤¼ņŖż Ļ░ÉņŚ╝Ļ│╝ Ļ┤ĆļĀ©ļÉ£ Ļ░üļ¦ēļé┤Ēö╝ņäĖĒżņŚ╝ņØĆ ņŻ╝ļĪ£ ļŗ©ņĢłņä▒ņ£╝ļĪ£ ļ░£ņāØĒĢ£ļŗżĻ│Ā ņĢīļĀżņĀĖ ņ׳ļŗż.8 ļö░ļØ╝ņä£ ļ│Ė ņĀĆņ×ÉļōżņØĆ Ļ▒░ļīĆņäĖĒżļ░öņØ┤ļ¤¼ņŖżņŚÉ ņØśĒĢ£ ņøÉņØĖņØä ļ░░ņĀ£ĒĢśĻĖ░ ņ£äĒĢśņŚ¼ ņŚ╝ņ”ØņØ┤ ņ׳ļŖö ņāüĒā£ņŚÉņä£ ņĀäļ░®ņ▓£ņ×Éļź╝ ĒåĄĒĢśņŚ¼ ļ░®ņłśļź╝ ņ▒äņĘ©ĒĢśņŚ¼ Ļ▒░ļīĆņäĖĒżļ░öņØ┤ļ¤¼ņŖżņŚÉ ļīĆĒĢ£ PCR Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢśņśĆņ£╝ļéś, ļ░öņØ┤ļ¤¼ņŖżļŖö Ļ▓ĆņČ£ļÉśņ¦Ć ņĢŖņĢśļŗż. ļ│Ė ņ”ØļĪĆņŚÉņä£ ļéśĒāĆļé£ Ļ░üļ¦ēļé┤Ēö╝ņäĖĒżņŚ╝ ļ░Å Ļ│ĀņĢłņĢĢņä▒ ņĢ×ĒżļÅäļ¦ēņŚ╝ņØ┤ SARS-CoV-2ļ░öņØ┤ļ¤¼ņŖżņØś ņ¦üņĀæ Ļ░ÉņŚ╝ņ£╝ļĪ£ ņØĖĒĢ£ Ļ▓āņØĖņ¦Ć ļśÉļŖö ĒżļÅäļ¦ēņŚ╝ņØś ņ×¼ļ░£ņØĖņ¦ĆņØś ņŚ¼ļČĆļŖö ņĀĢĒÖĢĒ׳ ņĢī ņłś ņŚåļŗż. ĻĘĖļ¤¼ļéś ļ│Ė ņ”ØļĪĆ ĒÖśņ×ÉņØś Ļ▓ĮņÜ░ 2016ļģäĻ╣īņ¦ĆņØś Ļ▓Ćņé¼ ĻĖ░ļĪØ ļ░Å ļ¼Ėņ¦äņāü ņÜ░ņĢłņØś ĒżļÅäļ¦ēņŚ╝ Ļ│╝Ļ▒░ļĀźņØ┤ ņŚåņ£╝ļ®░, ļ░śļīĆņĢłņØś ĒżļÅäļ¦ēņŚ╝ Ļ│╝Ļ▒░ļĀźņØ┤ ņ׳ņŚłņ£╝ļéś ļé┤Ēö╝ņäĖĒżņŚ╝ņØä ļÅÖļ░śĒĢśņ¦Ć ņĢŖņĢśņ£╝ļ®░, ņØ┤ļ▓ł COVID-19 ĒÖĢņ¦ä ĒøäņŚÉļŖö ņóīņĢłņØś ņ×¼ļ░£ņØĆ ņŚåņŚłļŗż. ļö░ļØ╝ņä£ ĻĖ░ņĪ┤ ĒżļÅäļ¦ēņŚ╝ņØś ņ×¼ļ░£ļ│┤ļŗżļŖö SARSCoV-2ļ░öņØ┤ļ¤¼ņŖżņŚÉ ņåŹļ░£ļÉ£ ĒĢ®ļ│æņ”ØņØś Ļ░ĆļŖźņä▒ņØ┤ ļåÆļŗżĻ│Ā ņé¼ļŻī ļÉ£ļŗż.
Jiang et al10ņØĆ SARS-CoV-2ļ░öņØ┤ļ¤¼ņŖż Ļ░ÉņŚ╝ Ēøä ļ░£ņāØĒĢ£ ņ¢æņĢłņä▒ņØś Ļ░üļ¦ēļé┤Ēö╝ ļČĆņĀäņØä ļ│┤Ļ│ĀĒĢśņśĆļŗż. COVID-19 ĒÖĢņ¦ä ĒÖśņ×É 672ļ¬ģņØś ņ×äņāü ņ¢æņāüņØä ļČäņäØĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ Ļ▓░ļ¦ēņŚ╝ņØä ļ│┤ņśĆļŹś Ļ▓ĮņÜ░ ņżæ ņĢĮ 78%ņŚÉņä£ļŖö ļŗ©ņĢłņä▒ņ£╝ļĪ£ ņ╣©ļ▓öĒĢśņśĆĻ│Ā, 22%ņŚÉņä£ ņ¢æņĢłņä▒ņØś ņ╣©ļ▓öņØä ļ│┤ņśĆļŗżĻ│Ā ĒĢśņśĆļŗż.11 ļö░ļØ╝ņä£ ņĀäņŗĀņĀü ļ░öņØ┤ļ¤¼ņŖż Ļ░ÉņŚ╝ ņØ┤ĒøäņŚÉ ņ¢æņĢłņä▒ņ£╝ļĪ£ ņĢłĻĄ¼ļź╝ ņ╣©ļ▓öĒĢĀ ņłśļÅä ņ׳ņ£╝ļéś, ļŗ©ņĢłņä▒ņ£╝ļĪ£ ņ×äņāü ņ¢æņāüņØ┤ ļéśĒāĆļé¼ļŗżĻ│Ā ĒĢśņŚ¼ SARS-CoV-2ļ░öņØ┤ļ¤¼ņŖżņŚÉ ņåŹļ░£ļÉ£ ĒĢ®ļ│æņ”ØņØś Ļ░ĆļŖźņä▒ņØä ļ░░ņĀ£ĒĢśļŖö ņåīĻ▓¼ņØĆ ņĢäļŗłļØ╝Ļ│Ā ņāØĻ░üļÉ£ļŗż.
ļ│Ė ņ”ØļĪĆņØś Ļ░üļ¦ē Ļ▓Įļ®┤ņäĖĒżĻ▓Ćņé¼ņŚÉņä£ ļé┤Ēö╝ņäĖĒż Ēü¼ĻĖ░ņØś ņ”ØĻ░Ć ļ░Å ņ¦äĒĢ£ ņØīņśüņØś ĒĢĄ(dark-reflecting nuclei), ņäĖĒż Ļ▓ĮĻ│äņØś ļČłļ¬ģĒÖĢņä▒(loss of cell boundary)ņØ┤ ņ”ØĻ░ĆļÉ£ ņåīĻ▓¼ņØ┤ ļéśĒāĆļé¼ļŗż. ĒŚżļź┤ĒÄśņŖżļ░öņØ┤ļ¤¼ņŖżĻ│╝ņØś ļ░öņØ┤ļ¤¼ņŖżļōżņŚÉ Ļ░ÉņŚ╝ļÉ£ Ļ░üļ¦ēļé┤Ēö╝ņäĖĒżņØś ĒśĢĒā£ļź╝ ļČäņäØĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ ņŚŁņŗ£ ĒĢĄņØś ņØīņśü ņ”ØĻ░Ć ļ░Å ņäĖĒż Ļ▓ĮĻ│äņØś ļČłļ¬ģĒÖĢņä▒ ļō▒ņØś ņåīĻ▓¼ņØä Ļ┤Ćņ░░ļÉśņŚłļŗż.12 COVID-19 ĒÖśņ×ÉņØś ĒśłĻĄ¼ņäĖĒżļź╝ Ļ┤Ćņ░░ĒĢśņśĆņØä ļĢī, ļ░öņØ┤ļ¤¼ņŖż Ļ░ÉņŚ╝ņŚÉ ņØśĒĢśņŚ¼ ļŗ©ĒĢĄĻĄ¼, ņżæņä▒ĻĄ¼ņØś ņäĖĒż Ēü¼ĻĖ░ ņ”ØĻ░Ć ļ░Å ļ”╝ĒöäĻĄ¼ņØś Ļ▓Įņä▒ļÅä ņ”ØĻ░Ć ņåīĻ▓¼ņØ┤ ļ│┤ņśĆļŗżĻ│Ā ļ│┤Ļ│ĀļÉśņŚłņ£╝ļéś13 SARS-CoV-2ļ░öņØ┤ļ¤¼ņŖż Ļ░ÉņŚ╝ņŚÉ ņØśĒĢ£ Ļ░üļ¦ēļé┤Ēö╝ņäĖĒż ļ¬©ņ¢æ ļ│ĆĒÖöņŚÉ ļīĆĒĢ┤ņä£ļŖö ņĢäņ¦ü ļ│┤Ļ│ĀĻ░Ć ņŚåĻĖ░ņŚÉ ņČöĒøä ņŚ░ĻĄ¼Ļ░Ć ļŹö ĒĢäņÜöĒĢĀ Ļ▓āņ£╝ļĪ£ ņé¼ļŻīļÉ£ļŗż.
ĒÖśņ×ÉļŖö ņ¢æņĢł ļÅÖĻ│ĄņØś ņé░ļīĆ ļ░Å ļ╣øļ░śņØæ ņåīņŗżņØä ļ│┤ņØ┤ļŖö ļō▒ ĻĖ┤ņןņä▒ ļÅÖĻ│Ą(tonic pupil) ņåīĻ▓¼ņØ┤ ļÅÖļ░śļÉśņŚłļŗż(Fig. 2). ĻĖ┤ņןņä▒ ļÅÖĻ│ĄņØĆ ņŗĀĻ▓Įņ╣£ĒÖöņĀüņØĖ ļ░öņØ┤ļ¤¼ņŖżņŚÉ ņØśĒĢ┤ ņ£Āļ░£ļÉ£ļŗżĻ│Ā ņĢīļĀżņĀĖ ņ׳Ļ│Ā,14 SARS-CoV-2ļ░öņØ┤ļ¤¼ņŖżļŖö ņŗĀĻ▓ĮĒĢÖņĀü ĒĢ®ļ│æņ”ØņØä ņ┤łļלĒĢśļ®░, ņØ┤ņĀä Ļ▓Ćņé¼ņŚÉņä£ ļÅÖĻ│ĄņØ┤ ņĀĢņāü ņåīĻ▓¼ņØ┤ņŚłņ£╝ļ»ĆļĪ£, ļ│Ė ņ”ØļĪĆņØś ĻĖ┤ņןņä▒ ļÅÖĻ│ĄņØĆ COVID-19ņŚÉ ņØśĒĢ£ ĒĢ®ļ│æņ”Øņ£╝ļĪ£ ņé¼ļŻīļÉ£ļŗż.15 ņØ┤ņÖĆ Ļ┤ĆļĀ©ĒĢśņŚ¼ denervation sensitivity ļō▒ ļŗżļźĖ ņŗĀĻ▓ĮĻ│╝ņĀü ņ”ØņāüļōżņŚÉ ļīĆĒĢ£ ĒÅēĻ░ĆļŖö ļ│Ė ņ”ØļĪĆņŚÉņä£ļŖö ņØ┤ļŻ©ņ¢┤ņ¦Ćņ¦Ć ņĢŖņĢśļŗż.
SARS-CoV-2ļ░öņØ┤ļ¤¼ņŖż Ļ░ÉņŚ╝ ĒÖśņ×ÉņŚÉņä£ ļŗżņ¢æĒĢ£ ņĢłĻĄ¼ ĒĢ®ļ│æņ”ØļōżņØ┤ ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ņ£╝ļéś ņĢäņ¦üĻ╣īņ¦Ć ļŗ©ņĢłņä▒ ņĢ×ĒżļÅäļ¦ēņŚ╝ ļ░Å Ļ░üļ¦ēļé┤Ēö╝ņäĖĒżņŚ╝Ļ│╝ ļ╣äĻ░ĆņŚŁņĀüņØĖ ļé┤Ēö╝ņäĖĒż ņåÉņāüņŚÉ ļīĆĒĢ£ ļ│┤Ļ│ĀļŖö ņŚåņŚłļŗż. ĒŖ╣Ē׳ ĒĢ┤ļŗ╣ ņ”ØļĪĆļŖö ļ░£ļ│æ ņĀäĒøäņØś Ļ░üļ¦ēļé┤Ēö╝ņäĖĒż ņåÉņāü ņĀĢļÅäļź╝ ņ¦üņĀæņĀüņ£╝ļĪ£ ļ│┤ņŚ¼ņŻ╝ņŚłļŗżļŖö ņĀÉņŚÉņä£ ĻĘĖ ņØśņØśĻ░Ć Ēü¼ļŗżĻ│Ā ĒĢĀ ņłś ņ׳Ļ▓Āļŗż. COVID-19 ĒÖśņ×ÉņŚÉņä£ ņĢłĻĄ¼ ļé┤ ņŚ╝ņ”ØņØ┤ ņ׳ņØä ļĢī Ļ░üļ¦ēļé┤Ēö╝ņäĖĒżņŚÉ ļīĆĒĢ£ Ļ▓Ćņé¼Ļ░Ć Ļ│ĀļĀżļÉśņ¢┤ņĢ╝ ĒĢśĻ▓Āļŗż.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






