교감안염 환자의 수상안에서 무세포 사람 보존각막을 이용한 구조적 각막이식술
Tectonic Keratoplasty Using Acellular Preserved Human Cornea for the Inciting Eye in Sympathetic Ophthalmia
Article information
Abstract
목적
교감안염의 수상안에서 무세포 사람 보존각막을 이용한 구조적 각막이식술을 통해 시력을 개선시킨 치료 경험을 공유하고자 한다.
증례요약
68세 남자 환자가 2개월 전, 못에 좌안을 수상한 뒤 최근 악화된 양안 시력저하를 주소로 내원하였다. 최대교정시력 우안 0.32, 좌안 0.16이었다. 검진상 좌안 상측부 주변부 각막에 전방수 유출 없이 홍채마개를 동반한 각막천공이, 우안 각막내피에 굳기름 침착물과 함께 전방 내 섬유소모양 띠가 관찰되었다. 빛간섭단층촬영상, 양안 모두 삼출성 망막박리와 맥락막주름들이 보였다. 익일, 전신 스테로이드와 함께 좌안의 괴사 홍채절제, 홍채유착 박리 및 천공 부위에 무세포 보존각막을 이용한 구조적 각막이식을 시행하였다. 삼출성 망막박리는 양안 모두 호전되었고, 수술 4개월째 수상안 백내장수술을 시행하였으며, 내원 21개월 후 좌안 나안시력 1.0으로 개선되었고 양안 모두 시신경위축이나 맥락망막염의 재발 없이 저녁노을안저 소견을 보였다.
결론
주변부 각막천공이 동반된 교감안염의 수상안에서, 내과적 항염증 치료와 더불어 무세포 보존각막을 이용한 구조적 각막이식술을 효과적으로 시도해볼 수 있겠다.
Trans Abstract
Purpose
We report a case of sympathetic ophthalmia in which the inciting eye was treated with a tectonic keratoplasty using acellular preserved human cornea.
Case summary
A 68-year-old man whose left eye was injured by a nail visited our institute complaining of a recent decrease in bilateral vision. The best corrected visual acuity was 0.32 for the right eye and 0.16 for the left. On slit-lamp examination, a superior peripheral corneal perforation with no wound leakage due to iris plugging was seen in the left eye (i.e., the inciting eye). The right eye (i.e., the sympathizing eye) had mutton-fat keratic precipitates and copious fibrinoid strands in the anterior chamber. Bilateral exudative retinal detachment with choroidal folds was prominent in both eyes. The next day, the necrotic iris lump was removed from the inciting eye and adhesiolysis of the iris and tectonic keratoplasty using acellular preserved human cornea were performed. Systemic steroid was started immediately postoperatively. The exudative retinal detachment improved in both eyes and cataract surgery was undertaken for the inciting eye 4 months later. Twenty-one months after the initial visit, the uncorrected visual acuity was 1.0 in the inciting eye, and both eyes had a sunset glow fundus appearance, without optic atrophy or recurrent chorioretinitis.
Conclusions
Tectonic keratoplasty using acellular preserved human cornea with anti-inflammatory treatment may be a favorable therapeutic option for the inciting eye with peripheral corneal perforation in sympathetic ophthalmia.
교감안염(sympathetic ophthalmia)은 한 쪽 눈의 외상 또는 수술 이후에 수상안(inciting eye)과 반대안인 교감안(sympathizing eye) 모두에서 육아종성 포도막염이 발생하는 질환으로1 외상 후 교감안염의 발생률은 0.1%에서 3%로서 비교적 드물게 발생한다.2-4 안구의 면역특권이 유지되던 조직이 외상이나 수술 후 외부에 노출되어 면역특권이 깨지면서 발생하게 되며, T세포가 매개하는 일종의 지연성 면역 과민반응이다.5 이 때문에 교감안염은 선행 원인이 발생한 후 대개 수일에서 수년 후에 발생하는데, 약 90%에서는 외상 후 1년 이내에 발생한다고 보고되었다.1
일단 교감안염이 발생하게 되면, 시력소실을 최대한 방지하기 위해 우선적으로 전신 스테로이드와 면역억제제를 투여하는 것이 일차적인 치료로 알려져 있다.6 교감안염 환자에서 수상안의 수술적 치료는 이제껏 드물게 보고되었으며, 특히 각막이식을 시행한 예는 국외에서 보고된 전층각막이식 3예가 유일하며7-9 무세포 보존각막을 이용하여 수상안을 치료한 예는 보고된 바 없었다.
본 증례에서는 수상 후 환자가 치료를 받지 않은 상태에서 천공된 주변부 각막이 홍채마개로 자연 폐쇄된 다음 수 개월 후 발생한 교감안염에서 전신 스테로이드 치료와 더불어 괴사 홍채절제, 주변부 홍채유착박리술 및 무세포 보존각막을 이용한 구조적 각막이식(tectonic keratoplasty)으로 성공적으로 치료한 증례를 최초 보고하고자 한다.
증례보고
특이 안과적 과거력이 없는 68세 남자 환자가 2개월 전 작업 중 튕겨 나온 못에 좌안을 수상한 후 양안 시력저하가 발생하였으나 치료 없이 지내다 본원 내원 5일 전부터 양안 시력저하가 악화되어 내원하였다. 이전에 안과를 방문한 적은 없었다고 하였다. 본원 초기 내원 시, 최대교정시력 우안 0.32, 좌안 0.16이었다. 세극등현미경검사상, 좌안 12시 방향의 윤부 각막에 홍채탈출이 동반된 약 3.0 mm 길이의 전층 각막열상 창상이 있었고 홍채마개 위로 상피화가 이루어져 있었기 때문에 전방수의 외부 누출은 없었다(Fig. 1A, B). 좌안의 홍채후유착이 저명하였다(Fig. 1C). 반대안인 우안은 전방 내 염증성 섬유소모양(fibrinoid) 띠가 있었고, 하측부 각막내피에 굳기름침착물(mutton fat keratic precipitate)이 관찰되었다(Fig. 1D). 양안 각막은 전반적으로 투명하였으며, 경면현미경검사상 각막내피세포의 밀도는 우안 3,488개/mm2, 좌안 3,452개/mm2였다. 광각안저촬영상 양안 모두 삼출성 망막박리가 저명하였고 특히 좌안은 시신경유두부종이 관찰되었으며, 빛간섭단층촬영상 양안 모두 황반부 망막하액 및 맥락막주름이 뚜렷하였다(Fig. 1E, F). 종합하였을 때, 과거 좌안의 주변부 각막천공 이후 발생한 양안의 교감안염이라고 추정하였고, 좌안은 탈출된 홍채표면으로 상피화가 이미 이루어졌고 Seidel 음성이었으나 주변부 홍채탈출이 지속적으로 염증을 유발하거나 안구표면의 면역세포들을 통해 안구 면역특권을 회피하고 있다고 판단하였다.
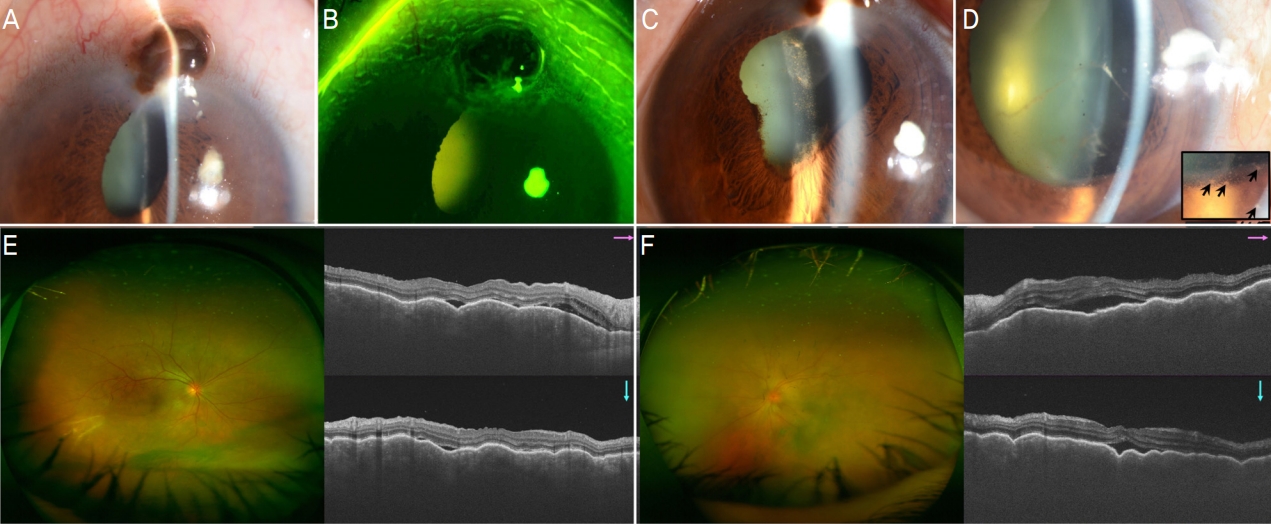
Slit-lamp, optical coherence tomography and wide fundus photographs of the bilateral sympathetic ophthalmia at his initial visit. (A-C) The iris plug through the peripheral corneal perforation without wound leakage and the prominent posterior iris synechiae were seen in the inciting eye (i.e. left eye). (D) In a sympathizing eye (i.e. right eye), copious fibrinoid strands were visible in the anterior chamber and the corneal endothelial mutton-fat keratic precipitates (arrows in a magnified rectangle) were seen. (E, F) In the posterior segment, exudative retinal detachment with multifocal choroiditis was seen in both eyes. For the left eye, optic disc swelling was also seen.
이에 초기 내원 익일, 좌안의 괴사 홍채절제, 홍채유착박리와 함께 천공 부위에 무세포 보존각막을 이용한 구조적 각막이식을 시행하였다. 수술은 전신마취로 시행하였으며, 탈출된 홍채마개 주위 결막을 박리한 후(Fig. 2A), 탈출된 괴사 홍채를 절제하여(Fig. 2B) 주변부 각막천공 부위를 노출시켰다(Fig. 2C). 천공된 각막 창상부 테두리의 염증성 각막 조직을 일부 절제한 후(Fig. 2D), 무세포 사람 보존각막(sterile full-sized and split thickness cornea; Halo, Eversight, Ann Arbor, MI, USA)을 4.0 mm 직경의 원형으로 절제하여 10-0 나일론 봉합사로 고정 봉합하였다(Fig. 2E). 수술 부위 전방 형성을 돕기 위해 전방 내 공기를 주입하고(Fig. 2F) 수술을 종료하였다.
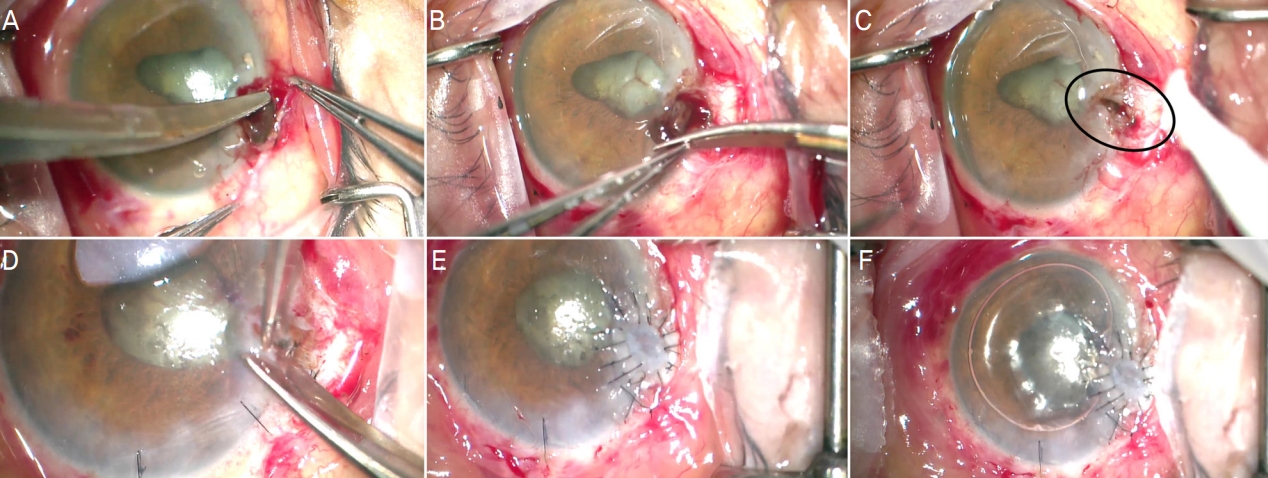
Intraoperative photographs of the inciting eye. After dissecting the conjunctiva (A), the prolapsed and necrotic iris lump was excised (B). The corneal perforated area was outlined (black oval, C) and the inflammatory friable wound margin was trimmed (D). Then, half-thickness of the acellular preserved human corneal tissue was transplanted using 10-0 nylon sutures (E). At the end of the surgery, the room air was injected in the anterior chamber (F).
혹시 모를 감염의 악화를 방지하고자 정맥 내 세파졸린(Cefazolin CKD Inj 1 g, Chong Kun Dang Parmaceutical Corp., Seoul, Korea) 및 겐타마이신 주사(Gentamicin Shinpoong Inj 80 mg/2 mL, Shin Poong Pharm Co., Ltd., Ansan, Korea)를 수술 전 투여하였다. 수술과 동시에 정맥 내 메틸프레드니솔론 주사(Salon Inj 500 mg, Halim Parm Co., Ltd., Seoul, Korea)를 하루 1 g씩 3일간 투여하였고, 정맥 내 항생제 투여는 5일간 유지하였다. 이후 경구 프레드니솔론(Solondo Tab, Yuhan Corporation, Seoul, Korea)으로 변경하여 지속 투여하였으며, 수술 직후부터 0.5% moxifloxacin (Vigamox®, Alcon, Fort Worth, TX, USA) 좌안 하루 6회, 1% prednisolone acetate (Predforte®, Allergan, Irvine, CA, USA) 양안 모두 2시간 간격, 1% atropine sulfate (Isopto atropine®, Alcon) 양안 하루 2회 점안하였다. 초기 내원 1달째 양안 모두 망막하액과 맥락막주름은 소실되었고, 나안시력 우안 0.4, 좌안 0.125로 호전되었으며 이식편의 상피화는 이루어졌고 이식 부위 벌어짐은 없었다. 초기 내원 3개월째 양안 맥락막주름이 재발하여 경구 프레드니솔론을 하루 20 mg으로 증량하고 서서히 감량하면서 지속 복용하여 재호전되었다. 점안 1% 프레드니솔론은 좌안은 3개월간 유지한 후 중단하였고 우안은 지속적으로 하루 6회 점안하였다.
초기 내원 4개월째 Lens Opacities Classification III 기준상 좌안 피질 혼탁 2단계, 핵경화 4단계로 악화되어 초음파 수정체유화술 및 인공수정체 후방 삽입술을 시행하였다. 백내장수술 1개월째, 각막은 투명하고 주변부 홍채 재유착은 없었고 무세포 각막이식 부위는 편명하고 상피결손 없이 안정적으로 유지되었으며(Fig. 3), 나안시력 우안 0.5, 좌안 0.63으로 호전되었다. 초기 내원 5개월째, 양안 맥락막 두께가 경미하게 증가하고 맥락막주름이 재발하여 경구 프레드니솔론을 다시 20 mg으로 증량하여 서서히 감량하였으며 2주 만에 양안 모두 호전되었다.
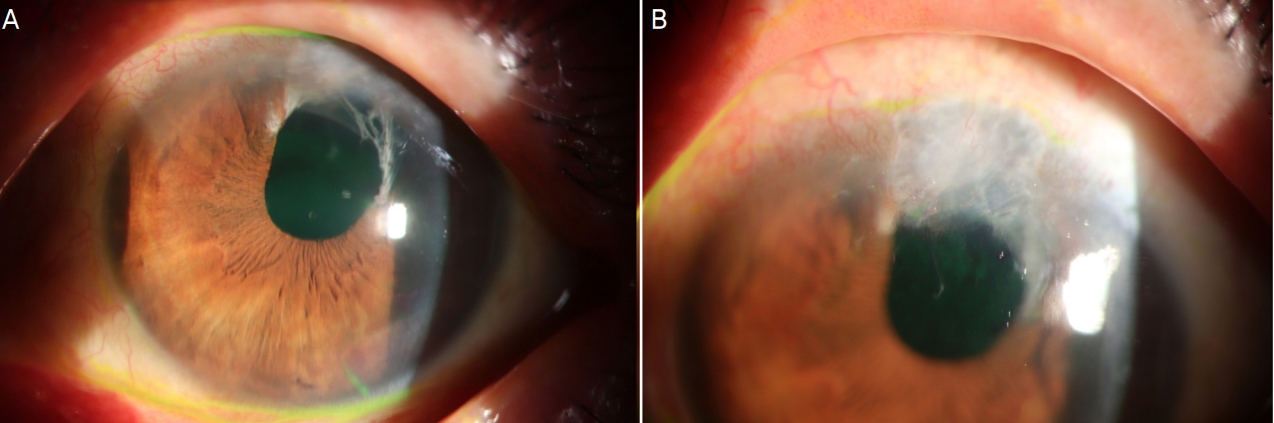
The slit-lamp photographs of the inciting eye 4 months after the tectonic keratoplasty. Most of the corneal area maintained clear (A) and the graft showed smooth surface with full epithelization (B).
이후 양안 모두 교감안염의 재발은 없었고 무세포 각막 이식 부위는 정상 유지되었다. 마지막 내원이었던 초기 내원 21개월째 교감안염의 재발 방지를 위해 경구 프레드니솔론은 하루 2.5 mg으로 유지한 상태였으며, 양안 모두 저녁노을안저(sunset glow fundus)를 보였고 빛간섭단층촬영상 양안 황반부 정상 소견 보였다(Fig. 4). 우안은 중심성 후낭하 백내장이 진행되어 나안시력 0.25로 감소하였으나, 좌안 나안시력은 1.0으로 호전되었다.

Wide fundus photographs and optical coherence tomography 21 months after the initial visit. The sunset glow fundus was seen without neurosensory detachment in both the sympathizing eye (A) and the inciting eye (B). There was no optic disc atrophy in both eyes.
고 찰
교감안염은 안구의 개방 손상, 백내장수술, 유리체망막수술, 녹내장수술, 섬모체파괴수술, 홍채섬모체 흑색종 제거술, 맥락막 종양의 양성자빔 치료, 사시수술 등 다양한 원인에 의해 발생할 수 있고, 손상 자극 후 발생까지의 기간 범위 역시 5일에서 66년까지 매우 넓은, 드물지만 독특한 질환이다.6 교감안염은 초기에 CD4 양성의 T도움세포(CD4+ helper T cell)가 포도막에 침윤하고 이후 CD8 양성의 세포독성 T세포가 뒤따라 침윤한다.10,11 그 결과 맥락막이 미만성으로 두꺼워지고 상피모양세포(epithelioid cell)와 다핵거대세포(multinuclear giant cell)들의 집락이 조직 내 관찰되며, 홍채 역시 두꺼워지면서 결절성 염증 침윤이 동반된다.12 이러한 면역반응이 병태생리의 중요한 축이기 때문에 초기 치료는 스테로이드와 면역억제제의 전신 투여가 일반적인데, 강력한 항염증 치료에도 불구하고 띠모양각막병증, 백내장, 각막부종, 수포성 각막병증, 각막내피손상, 홍채 위축, 모양체 위축, 이차성 녹내장, 맥락망막변성, 황반변성, 시신경위축 등 다양한 합병증을 초래할 수 있으며,8 나쁜 시력 예후로 이어지기 쉽다.
과거 교감안염 환자에서 수상안을 수술적으로 치료한 증례는 거의 없었고, 특히 혼탁해진 수상안의 각막을 치료하여 시력을 개선하기 위해서 3건의 전층각막이식술이 보고된 바 있었다. 이들은 각막혼탁, 띠모양각막병증으로 시력이 현저하게 저하된 환자들이었으며, 수술 전후로 전신 면역억제 치료를 동반하였었다.7-9 본 증례에서는 초기 내원 당시 양안 모두 각막의 투명도는 양호하였고 각막내피세포 밀도 역시 정상이었으며 창상 부위의 방수누출이 없이 홍채마개로 천공 부위가 자연 폐쇄되어 있었다. 하지만 천공 부위에 끼어 있는 홍채의 지속적인 자극이 안구 내 포도막염을 계속하여 조장할 수 있고 각막의 주변부에는 중심부와 달리 CD11b, CD11c, MHCII 양성의 성숙 수지상세포가 존재하기 때문에13 교감안염의 지속 및 악화 요인으로 작용할 수 있다고 판단하였다. 이에 내과적 치료와 더불어 본 증례에서는 홍채와 주변부 각막의 접촉을 없애서 후천적 면역 활성화를 방지하는 목적의 수술적 치료를 결정하였다. 과거 보고된 전층각막이식 시행 예들에서는 교감안염의 만성기 비특이적 면역반응을 억제하기 위해 지속적으로 전신 스테로이드를 사용하면서 이식편의 각막내피 거부반응 역시 억제하기 위해 mycophenolate mofetil과 azathioprine과 같은 T세포 억제제를 동반 투여하였다.7-9 반면, 본 증례에서는 T세포 억제제를 사용하지 않았고 수술 직후부터 전신 스테로이드만 사용하고도 이식편이 단기간 내 성공적으로 생착하고 거부반응이 발생하지 않았는데, 이는 이식 범위가 직경 4 mm로 작고 무세포 각막을 사용하였기 때문이라고 판단된다.
본 증례에서 사용한 무세포 보존각막은 원래 각막두께의 절반으로 분리한 9.5 mm 직경의 보존각막을 해외의 안은행에서 구입하여 사용하였다. 전자선 조사(electron beam irradiation; 15-21 KGy) 후 무세포화시켰기 때문에 이론적으로 거부반응의 위험을 줄일 수 있고, B형 간염, C형 간염, 매독, 에이즈에 대한 사전 선별검사를 거친 후 겐타마이신(gentamicin)과 스트렙토마이신(streptomycin)을 포함하는 보존액에서 조직 회복 과정을 거친 후, rice derived recombinant human serum albumin (rHSA) 용액이 든 포장 비닐 속에서 상온 보관되기 때문에 사용이 편리한 장점이 있다.
전통적으로 교감안염의 발생을 예방하기 위해 심한 안구 관통상 발생 이후 10일에서 2주 이내 수상안을 안구내용제거술이나 안구적출술로 제거하는 것이 중요하다고 알려져 있다.2 하지만 안구를 적출하는 것만이 능사는 아니며 환자의 입장에서도 쉬운 선택이 아닐 수 있다. 더군다나 때때로 교감안염 환자에서 수상안의 시력 예후가 교감안보다 더 낫기도 하다.9 교감안염이 발생한 이후에는 수상안의 안구 제거가 치료에 효과가 있는지는 논란이 있으며 Kilmartin et al3은 교감안염 발병 이후에 이차적으로 시행하는 수상안의 안구적출술이 교감안의 시력 예후나 내과적 약물 치료 감량에 도움이 되지 않는다고 보고하기도 하였다. 따라서 최근에는 안구 수상 시 빠른 시일 내에 일치적으로 해부학적 회복을 시키는 것이 바람직하다는 의견이 우세하며,9 교감안염이 발생한 이후에도 본 증례에서와 같이 적절한 내과적 및 외과적 약물 치료를 시행한다면 경우에 따라서 중증 합병증 없이 좋은 시력 예후를 가지고 올 수 있다.
비록 본 단일 증례로 천공 부위가 자연 폐쇄된 교감안염 환자에서 무세포 보존각막을 이용한 수복적 각막이식술을 동반 시행하는 것이 내과적 단일 치료보다 효과적일지, 또는 전층 기증각막을 이용하는 것보다 나을지는 알 수 없지만, 주변부 각막천공이 동반된 교감안염에서 무세포 보존 각막을 이용한 구조적 각막이식술을 내과적 스테로이드 치료와 더불어 시도해볼 수 있는 수술적 치료 중 하나로 고려해볼 수 있을 것이다.
Notes
Conflicts of Interest
The authors have no conflicts to disclose.
References
Biography
하동희 / Dong Hee Ha
중앙대학교 의과대학 중앙대학교병원 안과학교실
Department of Ophthalmology, Chung-Ang University Hospital, Chung-Ang University College of Medicine
