동맥염성 앞허혈시신경병증의 전형적인 임상 증상 없이 거대세포동맥염의 아형으로 진단된 1예
A Case of Subtype Giant Cell Arteritis Without Symptoms of Arteritic Anterior Ischemic Optic Neuropathy
Article information
Abstract
목적
동맥염성 앞허혈시신경병증의 전형적인 증상이 없는 시신경유두부종으로 내원하여 국내에서 이전에 보고된 바 없는 거대세포동맥염의 아형으로 진단된 1예를 보고하고자 한다.
증례요약
72세 남자가 1주 전부터 발생한 좌안의 시력저하로 내원하였다. 좌안의 시력은 0.02였고 시신경유두부종, 상대구심동공장애를 보였다. 시력저하 이외의 다른 임상 증상은 없었고 혈액검사에서 이상 소견을 보이지 않았으며 자기공명영상에서 특이 소견이 없어 앞허혈시신경병증으로 진단하였다. 이후 시력의 호전은 없었고 시신경위축이 발생하였다. 6개월 뒤 우안의 시력저하로 재내원하였고 좌안과 동일한 양상의 임상 소견이 확인되었다. 측두동맥의 조직검사를 진행하였고 거대세포동맥염의 아형으로 최종 진단되었다.
결론
본 증례는 거대세포동맥염의 전형적인 임상 증상이나 염증이 의심되는 혈액검사 소견이 없었음에도 불구하고 측두동맥 조직검사를 통해 거대세포동맥염의 아형으로 최종 진단된 경우이다. 한국에서는 드물게 보고 있지만 영구적인 실명을 일으킬 수 있어 두 눈에 발생한 시신경유두부종의 경우 항상 거대세포동맥염의 가능성을 고려하여야 한다.
Trans Abstract
Purpose
We report a case of papilledema without the typical symptoms of arteritic anterior ischemic optic neuropathy, ultimately diagnosed as a subtype of giant cell arteritis, which has not been reported previously in Korea.
Case summary
A 72-year-old man visited the hospital with decreased visual acuity in his left eye of 0.02 that had occurred 1 week prior. Optic disc swelling and relative afferent pupillary disorder were also evident in the left eye. Magnetic resonance imaging revealed no specific findings, leading to a diagnosis of anterior ischemic optic neuropathy. Afterwards, there was no improvement in visual acuity, and optic nerve atrophy occurred. Six months later, the patient complained of decreased visual acuity in the contralateral eye; the same clinical findings as in the left eye were confirmed. Temporal artery biopsy was performed, ultimately revealing a subtype of giant cell arteritis.
Conclusions
This case was finally diagnosed as a subtype of giant cell arteritis through temporal artery biopsy, despite the absence of typical clinical symptoms of this condition. Although giant cell arteritis is rare in Korea, it can cause permanent blindness. Therefore, the possibility of giant cell arteritis should always be considered with optic disc swelling in both eyes.
거대세포동맥염(giant cell arteritis)은 중간 및 큰 크기의 혈관에서 발생하는 자가면역 혈관염으로 측두동맥염(temporal arteritis)으로도 알려져 있다.1 이는 주로 대동맥과 그 분지혈관들에 호발하고 일반적으로 50세 이상의 고령에서 발생하며 두통, 두피 압통, 턱 파행, 권태감, 신경성 식욕부진, 체중감소, 염증 수치 증가 등의 특징적인 임상 양상을 보인다.2 거대세포동맥염으로 인한 동맥성 염증은 혈관 손상을 일으켜 협착, 폐색 및 동맥류를 유발할 수 있으며, 이들 중 50-70%에서는 눈으로 침범하여 심각한 시력상실을 초래할 수 있다.2,3 따라서 거대세포동맥염은 임상적으로 응급질환으로 고려되며, 빠른 진단과 치료가 이루어지지 않은 경우에는 빠르고 비가역적이며 반대눈까지 침범할 수 있는 시력저하를 일으킬 가능성이 있다.1-5
동맥염성 앞허혈시신경병증(arteritic anterior ischemic optic neuropathy)은 거대세포동맥염과 관련된 가장 흔한 안과적 합병증으로 비가역적인 시력저하를 일으킬 수 있는데 이는 시신경유두(optic nerve head)에 혈액을 공급하는 뒤 섬모체동맥의 폐색에 의해 발생한다고 알려져 있다.1,6,7 일반적인 거대세포동맥염의 치료는 영구적인 시력저하와 반대눈으로의 침범을 예방하기 위해 고농도 스테로이드 정맥주사가 알려져 있으며,6 여러가지 진단 방법들 중 하나로 측두동맥 조직검사가 유용하게 사용되고 있다.
거대세포동맥염의 특징적인 조직검사 소견은 림프구, 상피화 조직구(다핵거대세포), 대식세포와 섬유아세포 등의 염증세포들이 동맥혈관의 내막-중막 접합부에 주로 침윤하여 육아종성 염증을 나타내는 것으로 알려져 있으며 일부에서는 다핵거대세포가 관찰되지 않는 경우도 있다.8,9 하지만 거대세포동맥염이 의심되는 환자의 측두동맥 조직검사에서 측두동맥은 정상 소견이나 혈관외막 주위의 작은 혈관들에 염증이 국한되어있는 케이스들이 거대세포동맥염의 아형으로 보고되고 있다.9
거대세포동맥염은 북미와 서유럽 지역에서는 비교적 흔한 혈관염이지만2 아시아에서는 매우 드물게 나타난다.10-12 서양의 연구에 따르면 거대세포동맥염은 고령의 여성에서 호발하는 것으로 알려져 있는데, 동양인들을 대상으로 한 중국, 일본, 인도의 연구에 따르면 여성 호발이 뚜렷하지 않고 발병 연령이 낮으며(평균 43세), 시력저하와 턱 파행과 같은 전형적인 증상의 빈도는 낮으나 두통과 측두동맥 이상 소견은 자주 나타나는 것으로 보고되고 있다.13,14
한국에서의 발병률은 잘 알려져 있지 않으며 드물게 케이스들이 보고된 바 있으나,6,8,15,16 대부분의 경우 거대세포동맥염의 전형적인 임상 양상들이 나타난 경우이다. 하지만 거대동맥세포염 환자들 중 시력상실이 있었으나 다른 전형적인 임상 양상들이 나타나지 않는 경우가 21.2% 정도에서 보고된 바 있으며,8,10,12 이 보고들에서 적혈구침강속도와 C반응단백질 수치는 높게 보고되었다. 이에 저자들은 전형적인 거대세포동맥염의 다른 증상 없이 두 눈에 차례로 발생한 시신경유두부종과 시력저하로 내원한 환자에서 측두동맥 조직검사를 시행하여 거대세포동맥염의 아형으로 진단된 1예를 보고하고자 한다.
증례보고
72세 남자가 1주 전 오전부터 갑자기 발생한 좌안의 전반적인 시야 흐림 및 시력저하가 지속되어 내원하였다. 1주일 동안 시력저하는 점차 심해졌으며 두통이나 눈운동 시 통증은 없었고 그 외 특별한 이상 소견도 없었다. 과거력에서 혈압이나 당뇨 등 기저 질환은 없었으며 코골이나 수면무호흡증이 없는 비흡연자로 가족력이나 외상, 약물 복용력에서도 특이 사항이 없었다. 8년 전 양안 백내장수술을 시행받은 것 외에 안과적으로도 특별한 과거력은 없었다. 초진 시 나안시력은 우안 0.8, 좌안 0.02였고, 교정시력은 우안 1.0, 좌안은 교정되지 않았으며, 안압은 정상이었고 세극등현미경검사에서 특이 소견이 없었다. 안저검사에서 우안은 시신경유두함몰비 0.25로 정상이었고 좌안은 시신경유두부종이 확인되었다(Fig. 1A). 좌안의 상대구심동공장애가 관찰되었으며 좌안은 심한 시력저하로 색각검사 및 시야검사의 정확한 평가가 어려웠으나 우안은 색각검사와 시야검사 모두 정상이었다. 망막신경섬유층 광간섭단층촬영에서는 시신경유두 주변 망막신경섬유층 두께가 263 µm로 증가된 것을 보였다(Fig. 1B).
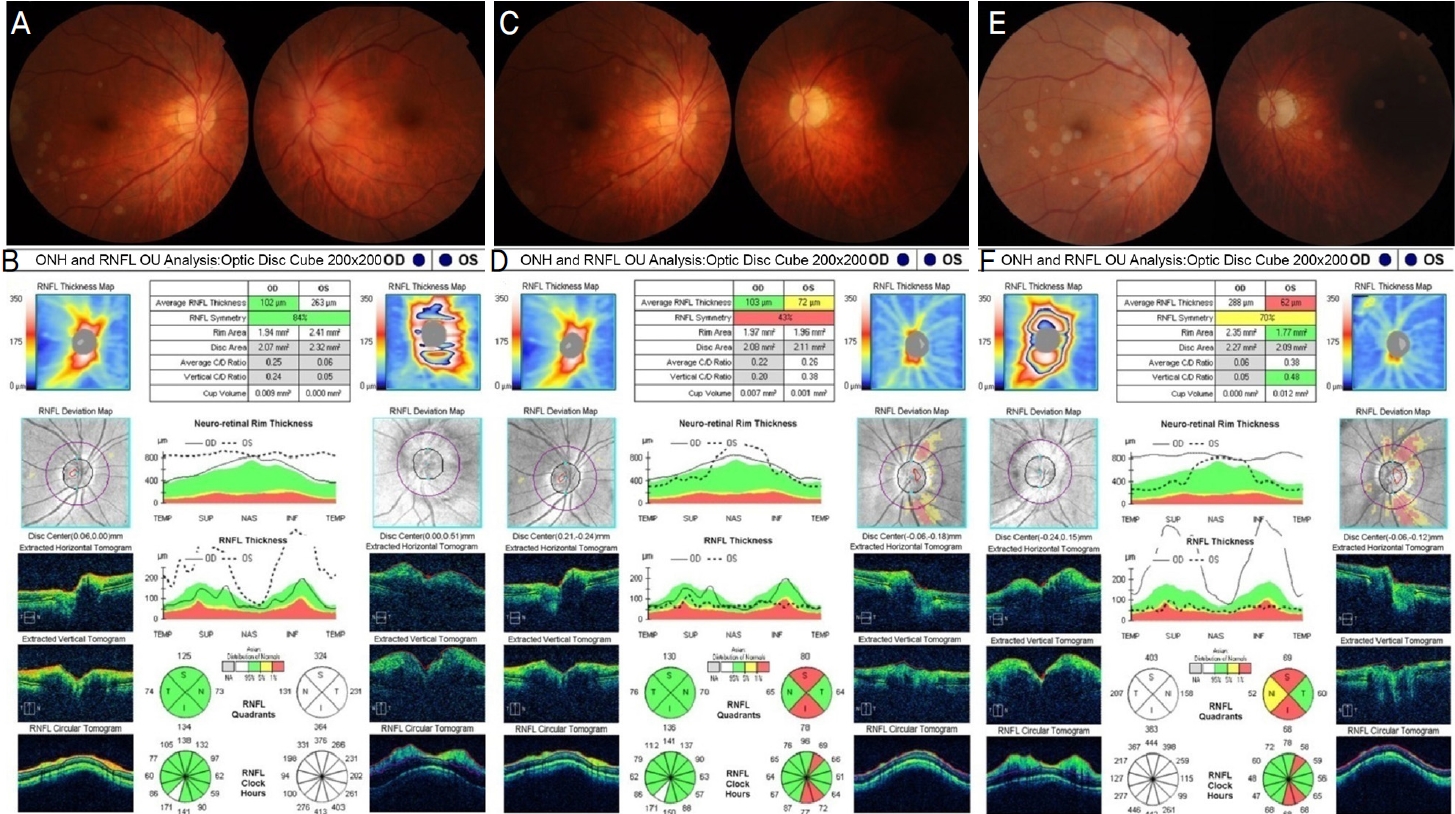
Fundus photographs and optical coherence tomography findings at the initial visit, after steroid treatment, and at revisitation after 9 months. (A) At the initial presentation, optic disc swelling was prominent in the left eye. (B) There was severe swelling of the peripapillary retinal nerve fiber layer (RNFL) in the left eye at the initial visit. (C) After 3 months, left optic disc swelling was improved but it became pale and atrophic, and (D) diffuse RNFL thinning of the left eye was observed after steroid treatment. (E) After 9 months, there was optic disc swelling with disc hemorrhage in the right eye and atrophic pale optic disc in the left eye. (F) Severe swelling of the peripapillary RNFL in the right eye was observed at the revisitation. OHN = optic newe head; OD = oculus dexter; OS = oculus sinster.
안와 자기공명영상검사에서 특이 소견은 보이지 않았고(Fig. 2A), 혈액검사에서 적혈구침강속도, C반응단백질, 전체 혈구 계산은 정상 수치였으며, 혈청검사에서 매독균, B형간염바이러스, C형감염바이러스, 인체면역결핍바이러스 감염 소견은 없었다. 또한 자가면역항체와 항아쿠아포린4항체도 음성이었으며, 흉부방사선검사에서 특이 소견은 없었다. 이에 앞허혈시신경병증 진단 후 시신경유두부종의 빠른 감소를 목적으로 경구 프레드니솔론(Solondo®, Yuhan Medical Corp., Seoul, Korea)을 하루 50 mg 7일, 30 mg 7일, 20 mg 21일, 10 mg 21일, 5 mg 30일 투여하였다. 좌안 시력저하 발생으로부터 3개월이 지난 후 좌안 시신경유두부종은 점차 호전되었으나 시신경유두는 위축되었으며(Fig. 1C) 시신경유두 주변 망막신경섬유층 두께는 72 µm로 감소하였고(Fig. 1D), 시력은 호전 없이 0.02로 유지되었다.
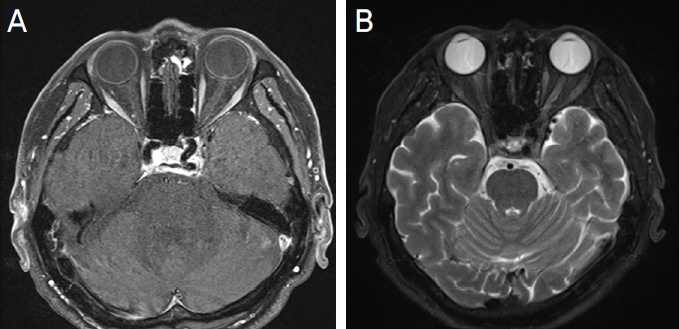
Orbital magnetic resonance imaging at the initial and at the revisitation after 9 months. (A) At the initial visit, axial contrast-enhanced T1 weighted image shows unremarkable findings in both optic nerves. (B) At the revisitation, axial fat suppressed T2 weighted image shows high signal intensity at the left optic nerve and subtle perineural enhancement at the right optic nerve.
그로부터 6개월 뒤 3일 전부터 갑자기 발생한 우안 시력 저하와 바깥쪽 시야 절반이 흐려보이는 증상이 점차 진행하여 재내원하였다. 안구통 및 두통은 없었으며 나안시력 우안 0.2, 좌안 안전수지 50 cm였고, 두 눈 모두 더이상 교정되지 않았다. 안저검사에서 우안의 시신경유두부종 및 11시 방향에 시신경유두출혈이 관찰되었고 좌안의 창백하고 위축된 시신경유두가 확인되었다(Fig. 1E). 광간섭단층촬영에서 시신경유두 주변 망막신경섬유층 두께가 우안은 288 µm로 증가, 좌안은 62 µm로 감소된 소견이 관찰되었다(Fig. 1F). 안와 자기공명영상검사에서 우측 시신경 주위로 미세한 조영증강이 확인되어(Fig. 2B) 우안의 시신경염을 의심하여 3일간 정맥 주사로 메틸프레드니솔론(Predisol®, Reyon Pharm, Ltd., Seoul, Korea)을 하루 1 g 투여를 시작하였으나 우안의 시신경유두부종은 호전되지 않았고, 우안 시력은 0.1로 저하되었다.
고농도 스테로이드 치료에도 호전되지 않아 앞허혈시신경병증의 재발을 다시 고려하였고 고령의 나이와 우안의 작은 시신경유두함몰비를 근거로 먼저 허혈시신경병증에 대한 위험인자 평가를 위해 순환기내과에 의뢰하여 경흉부 심장초음파, 관상동맥혈관조영 컴퓨터단층촬영, 뇌/경부혈관조영 자기공명영상검사들을 시행하였으나 모두 정상 소견이었다. 동맥염성 원인 감별을 위해 우측 측두동맥 조직 검사를 시행하였고, 최종적으로 거대세포동맥염의 조직학적 스펙트럼의 일부로 알려진 혈관외막 주위 작은 혈관에 혈관염이 동반된 염증이 없는 측두동맥을 보이는 측두동맥염(temporal arteritis showing uninflamed temporal artery with periadventitial small-vessel vasculitis)으로 진단되었다(Fig. 3). 우안 시신경유두부종이 계속 호전되지 않아 고용량 스테로이드 치료를 재개하였고 5일간 정맥 주사로 메틸프레드니솔론(Predisol®, Reyon Pharm, Ltd., Seoul, Korea)을 하루 1 g 투여하였다. 류마티스 내과로 전과하여 면역억제치료를 고려하였으나 전신 상태 악화로 진행하지 못하였고 장기간 고농도 스테로이드 치료 유지하기 어려워 경구 스테로이드로 변경하여 점차 복용량을 줄여나갔다. 우안 재발로부터 1개월 뒤 우안 시신경유두는 위축되었고, 시신경유두 주변 망막신경섬유층 두께는 98 µm로 감소하였으며, 우안 시력은 안전수지 50 cm로 저하되었다.
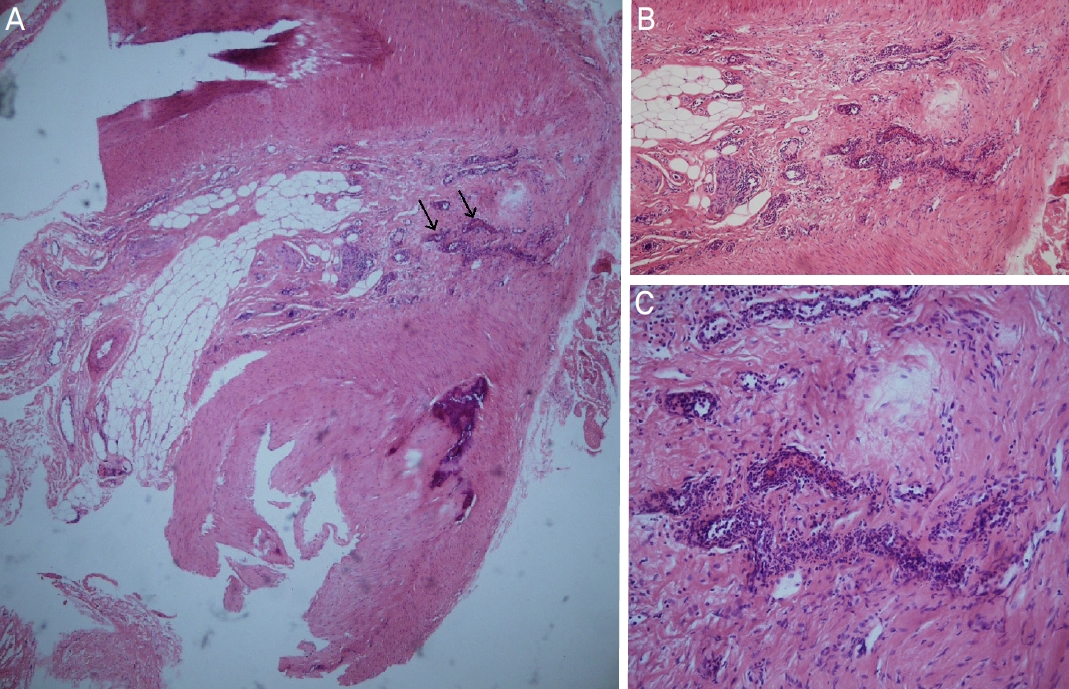
Histopathologic features of the right superficial temporal artery biopsy. Transverse sections of temporal artery specimens is shown. (A) Vasculitis involving periadventitial small vessels (arrows) adjacent to an uninflamed temporal artery (Hematoxylin and Eosin [H&E] stain, original magnification ×40). (B, C) inflamed periadventitial small vessels (B: H&E stain, ×100; C: H&E stain ×200).
고 찰
본 증례는 동맥염성 앞허혈시신경병증의 뚜렷한 임상 증상을 보이지 않았지만 측두동맥의 조직검사에서 혈관외막주위의 작은 혈관들에만 국한된 염증 소견을 보여 거대세포동맥염의 아형으로 진단되었던 경우를 소개하고 있다. 거대세포동맥염의 일반적인 임상 증상 없이 갑작스러운 시신경유두부종과 시력저하를 일으키는 거대세포동맥염 환자들의 경우 정확한 진단이 어렵고 적절한 치료를 빨리 시작하지 못해 급격히 진행하는 시력저하와 반대안으로의 파급을 예방하지 못할 수 있다.10
전형적인 거대세포동맥염의 조직검사 소견으로는 림프구, 다핵거대세포, 대식세포와 섬유아세포 등의 염증세포들이 동맥혈관의 내막-중막 접합부에 주로 침윤하여 나타난 육아종성 염증이 있으며, 일부에서는 다핵거대세포 없이 림프단핵구와 호중구, 호염구 등의 염증세포들이 동맥혈관의 전층에 침범한 범동맥염으로 나타나기도 한다고 알려져 있다. 하지만 거대세포동맥염 환자들에서 시행한 총 455건의 측두동맥 조직검사를 분석한 연구에 따르면, 일부 환자에서 염증 소견이 측두동맥에서는 관찰되지 않으나 혈관외막 주위의 작은 혈관들에 국한되어 나타난 경우가 있었고 이러한 환자들을 전형적인 거대세포동맥염 환자들과 비교해 보면 두통, 두피 압통, 턱 파행, 신경성 식욕부진, 체중감소 등 임상 양상들의 빈도가 유의미하게 적었으며, 염증 수치와 스테로이드의 총 투여량도 적게 나타났다.9
거대세포동맥염 환자들에서 시행한 285건의 측두동맥 조직검사를 분석한 연구에 따르면 주된 조직학적 양상으로 1) 염증세포들이 혈관외막에만 존재하고 중막과 내막은 침범하지 않은 혈관외막염 양상, 2) 내막은 침범하지 않고 국소적인 근육층 침범과 함께 외막의 염증세포 침윤이 있는 혈관외막침윤염 양상, 3) 염증세포들이 중막은 침범하지 않고 외막과 내막의 침윤을 보이는 혈관이중막염 양상, 4) 동맥혈관의 전층에 염즘세포 침윤이 나타난 전층동맥염 양상이 보고되었다. 기타 조직학적 양상으로는 1) 정상 측두동맥 조직이 비정상 조직과 섞여 있는 양상, 2) 측두동맥은 정상이나 혈관외막 주위의 작은 혈관에 혈관염이 동반된 양상, 3) 내막과 중막의 섬유화가 나타나는 양상들이 있었다.17
본 증례의 환자도 측두동맥의 조직검사 결과에서 측두동맥은 정상이었으나 혈관외막 주위의 작은 혈관들에만 국한된 염증 소견을 보여 거대세포동맥염의 아형으로 진단내릴 수 있었다. 하지만 좌안의 시력저하로 내원했던 초진 당시 검사 결과와 임상 증상만으로는 동맥염성 앞허혈성시신경병증을 의심하기 어려웠고 결과적으로 반대안으로의 침범이 발생하게 되었다. 반대안에 시신경병증이 발생 시에 고농도 스테로이드 정주 치료를 시도하였음에도 크게 호전되지는 않았다. 거대세포동맥염에 합당한 다른 임상 증상이나 혈액검사 소견이 없는 경우 일반적으로 측두동맥 조직검사를 진행하지 않으나, 이 증례에서와 같이 거대세포동맥염의 아형인 경우에는 전형적인 증상이나 검사 소견이 나타나지 않을 수 있어 주의가 필요하다. 다만 시신경병증 외의 다른 증상이나 검사 이상이 없는 모든 환자에서 조직검사를 시행하는 것에는 무리가 있어 향후 이러한 비특이적인 거대세포동맥염의 임상 양상과 치료에 대한 추가적인 연구들이 필요할 것으로 보인다.
Notes
Conflicts of Interest
The authors have no conflicts to disclose.
References
Biography
정삼영 / Sam Young Jung
가톨릭대학교 의과대학 서울성모병원 안과학교실 및 시과학교실
Department of Ophthalmology and Visual Science, Seoul St. Mary’s Hospital, College of Medicine
