체위에 따른 시력 변화를 보인 낭내 혈종 환자 1예
Visual Acuity Changes with a Position Shift in a Patient with an Endocapsular Hematoma
Article information
Abstract
목적
체위에 따른 시력 변화를 보인 낭내 혈종 환자를 유리체절제술로 치료한 증례를 보고하고자 한다.
증례요약
92세 여자 환자로 좌안이 기립 시 잘 보이나 누워있을 시 잘 보이지 않는, 체위에 따른 시력 변화가 있어 내원하였다. 기저질환으로 고혈압, 당뇨, 심부전이 있어 아스피린을 복용 중이었으며 15년 전 좌안 백내장수술을 받은 과거력이 있었다. 내원 시 최대교정시력은 좌안 0.5였으며, 안압은 23 mmHg였다. 전안부 세극등현미경검사상 좌안에서 안저를 일부 가리는 낭내 혈종이 관찰되었다. 3개월간 경과를 관찰하였으나, 낭내 출혈에 변화가 없고 체위에 따른 시력 변화가 지속되어 유리체절제술, 수정체후낭절개술, 전방세척술을 시행하였다. 수술 1달 후 좌안 시력은 0.4였으며 수술 전 호소하였던 체위에 따른 시력 변화는 관찰되지 않았다.
결론
낭내 혈종 환자는 체위에 따른 시력 변화가 있을 수 있으며, 유리체절제술도 하나의 치료 방법으로 고려해볼 수 있겠다.
Trans Abstract
Purpose
To report a vitrectomy performed on a patient with an endocapsular hematoma whose visual acuity changed with her position.
Case summary
A 92-year-old woman visited our hospital complaining of a visual acuity change in her left eye with good visibility while standing but poor visibility when lying. She was taking aspirin, had underlying hypertension, diabetes, and heart failure, and underwent left eye cataract surgery 15 years previously. At presentation, her best-corrected visual acuity in the left eye was 0.5, with an intraocular pressure of 23 mmHg. An endocapsular hematoma that partially covered the fundus in the left eye was found. The left eye was observed for 3 months. However, there was no change in the endocapsular hematoma and the discomfort persisted with the position shift; therefore, a vitrectomy, posterior capsulotomy, and anterior chamber irrigation were performed. One month postoperatively, the visual acuity in the left eye was 0.4 and there was no longer a change in the visual acuity with position.
Conclusions
A patient with an endocapsular hematoma may have changes in visual acuity with position, and a vitrectomy can be used to treat the endocapsular hematoma.
낭내 혈종(endocapsular hematoma)은 백내장수술 후 발생할 수 있는 출혈로 인공수정체 후면과 수정체 후낭 사이의 낭내 공간(endocapsular space)에 발생한 출혈이 흡수되지 않고 지속되는 상태를 말한다.1-3 낭내 혈종은 1989년 Thomas에 의해 처음 보고되었으며,1 1991년 Hegan에 의해 그 용어가 정립되었다.3 수술 후 발생할 수 있는 전방출혈과 비교하여, 낭내 혈종은 출혈의 양이 적고 전방출혈의 유무와 별개로 발생할 수 있으며 대개 유리체출혈은 동반하지 않는다.3 또한 낭내 혈종은 전방출혈에 비해 느리게 흡수되거나 흡수되지 않는 경우도 있다.2 이러한 낭내 혈종의 발생은 비교적 드물지만 적은 양이라도 시축을 침범하는 경우 시력저하를 일으키기 때문에 치료하는 것이 필요하다.2
낭내 혈종으로 인한 시력저하로 환자가 불편을 호소하거나 수개월 후에도 호전되지 않은 경우에는 대개 neodymiumdoped yttrium aluminium garnet (Nd:YAG) 레이저를 이용한 후낭절개술을 시행하여 성공적으로 치료해왔다.3-10 드물지만 수술로써 치료한 경우도 보고되었으나,8,11,12 현재까지 국내에서는 체위에 따라 시력이 변화하는 낭내 혈종의 치료에 대해 보고된 바가 없어 저자들은 낭내 혈종 환자를 유리체절제술로 치료하였기에 이를 증례로 보고하고자 한다.
증례보고
만 92세 여자 환자가 누운 자세에서 잘 보이지 않고 직립 시 잘 보이는, 체위 변화에 따른 좌안의 시력 변화를 주소로 내원하였다. 좌안의 증상 발생 시기는 정확히 기억하지 못하였으며, 고혈압, 당뇨, 심부전 등의 기저 질환으로 저용량 아스피린(100 mg, 1일 1회)을 복용 중이었다. 좌안의 경우 15년 전 백내장수술을 받은 바 있었으며, 내원 당시 최대교정시력은 좌안 0.5로 저하되어 있었으며 안압은 23 mmHg였다. 전안부 세극등현미경검사상 좌안에서 인공수정체 후방으로 혈종이 관찰되었다(Fig. 1A). 전방의 깊이나 전방각은 정상이었으며, 홍채의 이상은 관찰되지 않았고, 광각안저촬영상 출혈에 의해 안저가 일부 가려보였다(Fig. 1B). 출혈 경향을 확인하기 위한 혈액검사상 프로트롬빈시간(prothrombin time)은 11.3초, 활성화부분트롬보플라스틴시간(activated partial thromboplastin time)은 33.4초 등으로 이상 소견을 보이지 않았다.
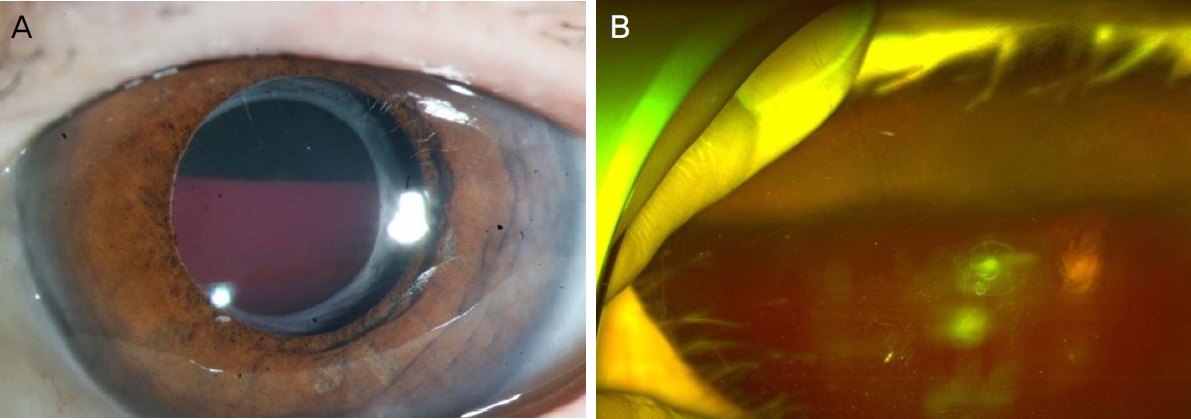
Preoperative findings at initial visit. (A) Anterior segment photography of the patient's left eye shows endocapsular hematoma. (B) Wide fundus photography of the patient's left eye shows hematoma which obscures the fundus and changes depending on postural change.
환자가 직립 시 시력저하를 호소하지 않아 우선 경과 관찰하였다. 그러나 3개월 후에도 낭내 혈종에는 변화가 없었으며, 지속적으로 체위 변화에 따른 좌안의 불편함을 호소하였다. 치료로 Nd:YAG 레이저를 우선적으로 고려하였으나, 레이저 시행 후 발생할 수 있는 유리체출혈에 대해 환자가 거부감이 있어 낭내 혈종을 빠르고 완전하게 제거할 수 있는 구후마취 하에 평면부유리체절제술을 계획하였다. 수술과 연관된 출혈을 예방하기 위해 아스피린 복용을 5일간 중단하였다.
낭내 혈종은 인공수정체와 후낭 사이에서 관찰되었다(Fig. 2A). 먼저 유리체절제기로 후낭절개술을 시행하여 일차적으로 혈종을 제거하였으나(Fig. 2B) 수정체낭 주변부에 남은 출혈이 있어 평형염액을 이용하여 전방세척술을 시행하였고(Fig. 2C) 앞의 과정에서 유리체강 내로 넘어간 출혈이 있어 평면부 유리체절제술을 시행한 후 완전히 출혈이 제거된 것을 확인하였다(Fig. 2D). 수술 중 경한 망막 전막이 관찰되었으나 시력에 영향이 미미할 것으로 판단하여 제거하지 않았다.
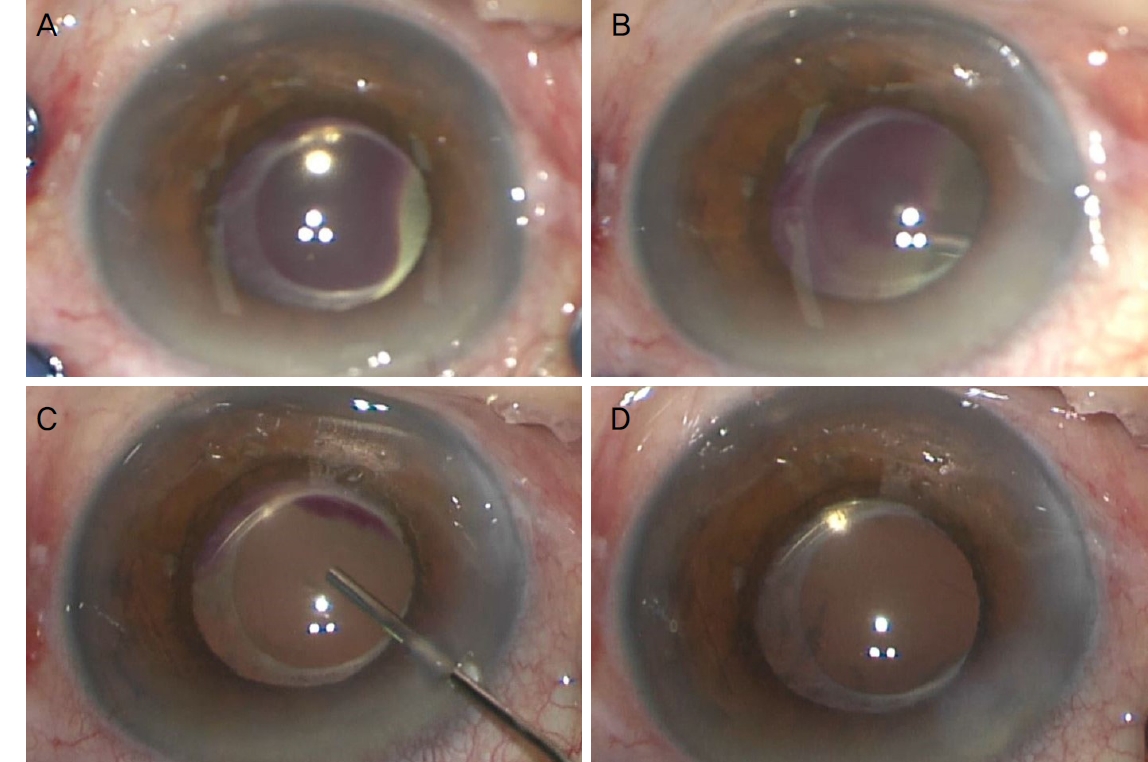
Intraoperative findings. (A) Endocapsular hematoma. (B) Endocapsular hematoma was removed after posterior capsulotomy using vitrectomy cutter. (C) Anterior chamber irrigation using vitrectomy cutter was done to remove hematoma at periphery posterior capsule. (D) Hematoma was completely removed after vitrectomy aiming to remove vitreous hemorrhage.
수술 한 달 경과 후 좌안에서 낭내 출혈은 관찰되지 않았으며(Fig. 3A), 좌안의 최대교정시력은 0.4, 안압은 16 mmHg였고 환자는 수술 전 있었던 체위 변화에 따른 시력 변화는 호소하지 않았다. 수술 당시 관찰되었던 망막전막은 변화가 없어 경과 관찰하기로 하였다(Fig. 3B-D).

Postoperative findings of the left eye one month after vitrectomy. (A) Anterior segment photography of the patient's left eye. Hematoma completely resolved. (B) Wide fundus photography of the patient's left eye shows well observed fundus and epiretinal membrane. Epiretinal membrane was noted on horizontal (C) and vertical (D) optical coherence tomography images of left eye.
고 찰
낭내 혈종은 비교적 드문 질환으로, 고령의 환자에서 백내장단독수술 또는 백내장과 녹내장병합수술 시 발생할 수 있는 것으로 알려져 있다.1-15 백내장 제거 방식과는 무관하게, 백내장낭외적출술,2-6,13 수정체유화술7-11,14 모두에서 발생할 수 있다. 평면볼록렌즈(plano-convex) 형태의 인공수정체를 사용했던 보고에 따르면 양면볼록렌즈(biconvex)를 사용할 경우 인공수정체의 광학부 후면 잠재적 공간을 폐쇄하거나 세포 이동을 차단하여 낭내 혈종을 방지할 수 있을 것으로 생각되었으나2,3 이후 보고에서 양면볼록렌즈 형태의 인공수정체를 사용했던 경우에서도 낭내 혈종이 발생하였다.2
발생 시기에 대해서 이전에 보고된 증례에서는, 수술 후 수일에서 약 12주 후, 즉 수술 3개월 이내로 발생되었던 경우가 대부분이다.15 본 증례의 환자는 15년 전 좌안 백내장 수술을 하였으며 기립 자세에서는 시력저하가 나타나지 않아 좌안의 시력저하를 환자가 즉시 인지하지 못했을 것으로 보인다. 때문에 수술 직후 혈종이 발생하였는지 이후 발생하였는지는 정확히 추정할 수 없었다.
낭내 혈종의 발생 원인은 명확하지 않으나 인공수정체에 의한 홍채 마찰, 인공수정체 지지부에 의한 모양체 미란(erosion), 포도막염녹내장출혈증후군, 외상,3 공막절개 및 윤부절개 시 혈관파열 발생, 전방각과 홍채, 유리체강으로부터의 유입,15 투명각막절개 시 섬유소 응집의 형성7 등이 제시된 바 있다. 발생된 출혈은 연속곡선수정체낭원형절개의 구축으로 인하여 인공수정체의 후면과 수정체 후낭 사이의 공간인 낭내 공간에 고립되고 섬유소분해 효소가 방수로부터 유입되지 않아 흡수가 일어나지 않는다.4
항응고제 및 항혈전제의 복용도 낭내 혈종의 발생에 기여하는 것으로 보인다. 승모판 역류로 진단된 후 와파린과 아스피린을 복용하였던 환자에서 백내장수술 5년 후 낭내 혈종이 발생된 바 있으며,6 급성심근경색으로 스트렙토키나아제와 아스피린을 복용하였던 환자에서 백내장수술 2년 후 낭내 혈종이 발생되었다는 보고가 있다.8 본 증례에서는 92세의 고령, 기저 질환으로 복용 중이던 아스피린이 낭내 혈종의 발생과 관련이 있을 것으로 생각된다.
낭내 혈종은 일단 발생하여도 시축을 가리지 않고 환자가 시력저하를 호소하지 않는다면 특별한 치료가 필요하지 않고,2,3 자연호전 되는 경우도 있으며13,14 체위배출을 시도하였던 바도 있다.1,5 그러나 낭내 혈종으로 인해 저하된 시력으로 인하여 환자가 일상생활에 불편함을 호소하고 나아가 백내장수술에 대한 만족도가 하락할 수 있기 때문에 시력저하를 유발하는 낭내 혈종에 대한 치료로는 Nd:YAG 레이저를 이용한 후낭절개술이 시행되어 왔으며3-10 드물게 유리체절제술를 비롯한 수술적 치료가 시행된 증례도 보고되었다. 백내장과 녹내장병합수술을 하였던 환자에서 발생한 낭내 혈종에 대해서 유리체절제술을 시행하여 효과적으로 치료하여 보고되었고,11 수정체 후낭을 따라 인공수정체까지 생성된 홍채신생혈관을 동반한 낭내 혈종에서도 유리체절제술을 성공적으로 시행한 바 있다.12 또한 각막윤부로 접근하여 수술적으로 낭내 혈종을 제거한 증례도 있다.8
본 증례에서 환자는 고령으로 혈종의 즉각적인 제거를 원하였다. 또한 저자들은 Nd:YAG 레이저를 이용한 후낭절개술은 시행 후 유리체출혈의 발생 가능성이 있어 환자의 만족도가 저하될 수 있다고 판단하였다. 이에 빠르고 완전한 회복을 위해 유리체절제술을 시행하여 혈종을 완전하게 제거하였고 후낭 절개를 통해 낭내 출혈의 재발을 예방할 수 있었다. 상기 증례를 통해 드문 증상인 체위에 따라 시력 변화가 있는 낭내 혈종을 보고하였으며 이는 유리체절제술로 치료할 수 있음을 알 수 있었다. 낭내 혈종으로 진단된 환자의 경우 유리체절제술을 하나의 치료 방법으로 생각해 볼 수 있겠다.
Notes
Conflicts of Interest
The authors have no conflicts to disclose.
References
Biography
황규은 / Gyu Eun Hwang
순천향대학교 의과대학 천안병원 안과학교실
Department of Ophthalmology, Soonchunhyang University Cheonan Hospital, Soonchunhyang University College of Medicine
