눈모음부족형 외사시에서 양안 외직근 후전 및 하방전위술과 양안 외직근 근경사후전술의 비교
Comparison between Down Transposition and Slanted Surgery for Bilateral Lateral Rectus Recession in Convergence Insufficiency-Type Exotropia
Article information
Abstract
목적
눈모음부족형 외사시에서 양안 외직근 후전 및 하방전위술과 양안 외직근 근경사후전술의 수술 결과를 비교하고자 한다.
방법
2012년 1월에서 2021년 1월까지 눈모음부족형 외사시로 양안 외직근 후전 및 하방전위술 또는 양안 외직근 근경사후전술을 시행받고 1년 이상 경과 관찰한 환아들을 대상으로 하였다. 성별, 나이, 수술 전 최대교정시력, 구면렌즈대응치, 안축장길이, 수술량, 수술 전, 수술 직후, 1주 후, 6개월 후, 1년 후의 사시각, 수술 전, 수술 6개월 후, 1년 후의 입체시, 그리고 수술 성공률을 후향적으로 비교분석하였다.
결과
하방전위술군 45명과 근경사후전술군 40명이 포함되었고 수술 1년 후 하방전위술군에서 원거리사시각은 1.96 ± 8.77 prism diopter (PD), 근거리사시각은 5.53 ± 9.09 PD로 감소하였고, 근경사후전술군에서 원거리사시각은 4.60 ± 4.99 PD, 근거리사시각은 9.03 ± 9.09 PD로 감소하였다. 근-원거리 사시각 차이는 수술 1년 후 하방전위술군에서 3.58 ± 5.26 PD, 근경사후전술군에서 4.43 ± 5.32 PD였다. 수술 1년 후 수술 성공률은 하방전위술군에서 55.6%, 근경사후전술군에서 52.5%이며 두 군 간의 유의한 차이는 없었다(p=0.778).
결론
눈모음부족형 외사시에서 양안 외직근 후전 및 하방전위술과 양안 외직근 근경사후전술 모두 원거리 및 근거리외사시 및 근-원거리사시각 차이를 교정하는데 효과적이었으므로 두 방법 모두 눈모음부족형 외사시의 일차수술로써 고려해 볼 수 있으리라 생각된다.
Trans Abstract
Purpose
We compared bilateral lateral rectus recession with down transposition and slanted bilateral lateral rectus recession as surgical methods for convergence insufficiency-type exotropia.
Methods
We included patients who underwent bilateral lateral rectus recession with down transposition or slanted bilateral lateral rectus recession for convergence insufficiency-type exotropia from January 2012 to January 2021 and observed them for more than 1 year. We retrospectively analyzed sex, age, preoperative best-corrected visual acuity, spherical equivalent, axial length, amount of surgery, and deviation angle before surgery and after surgery (immediately, 1 week, 6 months, and 1 year). We also examined surgical success and stereopsis before surgery and after 6 months and 1 year.
Results
The down transposition group included 45 patients and the slanted group included 40. The deviation angle of distance, deviation angle of near and the near-distance disparity (NDD) all decreased in the down transposition group and slanted group 1 year after surgery (1.96 ± 8.77 prism diopter [PD] and 4.60 ± 4.99 PD, respectively; 5.53 ± 9.09 PD and 9.03 ± 9.09 PD, respectively; and 3.58 ± 5.26 PD and 4.43 ± 5.32 PD, respectively). Surgical success after 1 year was 55.6% in the down transposition group and 52.5% in the slanted group, and there was no significant difference between the two groups.
Conclusions
In convergence insufficiency-type exotropia, both bilateral lateral rectus recession with down transposition and slanted bilateral lateral rectus recession were effective to correct the deviation angle of near, distance, and NDD. Both are suitable primary surgical methods for convergence insufficiency-type exotropia.
간헐외사시는 근거리 및 원거리 사시각에 따라 기본형, 눈벌림과다형, 거짓눈벌림과다형, 눈모음부족형으로 분류될 수 있다[1]. 눈모음부족형 외사시는 근거리사시각이 원거리사시각에 비해 10프리즘디옵터(prism diopter, PD) 이상 큰 경우이며, 특히 근거리에서의 눈모음이 부족하므로 학습능력의 저하, 두통, 간헐적 복시, 눈물 흘림, 흐려보임, 눈 피로 등을 호소한다[1,2]. 시기능 훈련이나 프리즘 안경 착용과 같은 비수술적 치료를 통해 증상을 경감시킬 수는 있으나 심한 경우에서는 수술적 치료가 필요하다[3].
기존의 외사시 수술 방법으로는 단안 외직근후전술 및 내직근절제술, 양안 내직근절제술, 양안 외직근후전술이 있으나 눈모음부족형 외사시에서는 근거리 부족교정 및 원거리 과교정 가능성이 높고 수술 성공률도 기본형 외사시에 비해 낮아서 수술 성공률을 높이기 위하여 다양한 수술 방법들이 시도되고 있다[4-7]. 원거리사시각 기준으로 외직근을 후전하고 근거리사시각 기준으로 내직근을 절제하는 증량한 단안 외직근후전술 및 내직근절제술, 양안 외직근 근경사후전술, 양안 외직근 후전 및 하방전위술, 한 눈 가림 전의 근거리사시각과 한 눈 가림 후 원거리와 근거리사시각의 평균으로 보정한 수술량을 기준으로 한 양안 외직근후전술 등이 보고되었다[8-23].
양안 외직근 후전 및 하방전위술은 의도적으로 수술 후 V형 사시를 유도하여 주로 하방 주시하게 되는 근거리 작업 시 외사시가 상대적으로 감소하게 하는 효과가 있으며, 양안 외직근 근경사후전술은 근거리 및 하방 주시 시 위쪽보다 아래쪽 근섬유가 더 짧아지는 외직근에서 아래쪽 근섬유를 더 후전함으로써 근거리 주시 시 외사시를 감소시키는 효과가 있다고 알려져 있다[8,24].
본 연구에서는 눈모음부족형 외사시에서 양안 외직근 후전 및 하방전위술과 양안 외직근 근경사후전술의 수술 결과를 비교하고자 한다.
대상과 방법
2012년 1월에서 2021년 1월까지 본원에서 눈모음부족형 외사시로 양안 외직근 후전 및 하방전위술 또는 양안 외직근 근경사후전술을 시행받고 수술 후 1년 이상 경과 관찰한 20세 이하의 환아를 대상으로 의무기록을 후향적으로 분석하였다. 마비사시, 제한사시, 사근의 기능항진, 수직사시, 사시수술 병력, 눈떨림, 약시, 안구의 기질적 이상 또는 전신적 이상이 있는 경우는 제외하였다.
눈모음부족형 외사시의 기준은 근거리사시각이 원거리사시각보다 10 PD 이상 큰 경우로 정하였다. 안경 교정이 필요한 경우 안경을 착용하고 원거리(6 m) 및 근거리(30 cm)에서 프리즘교대가림검사로 사시각을 측정하였으며, 원거리에서는 제1안위뿐만 아니라 30도 상방주시 및 30도 하방주시 상태에서의 사시각을 측정하였고 근거리에서는 정위에서만 사시각을 측정하였다. 외편위는 양의 값으로, 내편위는 음의 값으로 하였다. V형 사시는 상방주시 수평사시각과 하방주시 수평사시각이 15 PD 이상 차이 나는 경우로 하였고, A형 사시는 상방주시 수평사시각과 하방주시 수평사시각이 10 PD 이상 차이 나는 경우로 하였으며, 상방-하방주시 사시각 차이가 V형 사시 양상인 경우를 양의 값으로 하였고 반대의 경우 음의 값으로 하였다. 시력은 굴절이상을 교정 후 최대교정시력을 Snellen 시력으로 측정하였으며 logarithm of minimum angle of resolution (logMAR)으로 변환하여 분석하였다. 입체시 검사는 굴절이상을 교정한 뒤 검사하였으며, 근거리 입체시는 티트무스 원(Stereo Optical Co. Inc., Chicago, IL, USA)을 이용하여 40 cm 거리에서 편광안경을 착용하게 한 후 검사하였다. 티트무스 원의 시차는 단계에 따라 800, 400, 200, 140, 100, 80, 60, 50, 40 seconds of arc (seconds)였으며, 입체시의 판정은 원의 위치를 계속해서 두 번 틀린 경우에 그전 것을 피검자의 입체시로 하였다. 입체시가 낮은 경우는 통계학적 처리를 위해 3,000 seconds로 하였고, 자연로그를 이용하여 LogArcsec를 비교하였다[25].
모든 수술은 전신마취로 시행하였으며 한 명의 술자에 의해 시행되었다. 결막절개는 결막구석절개를 하였고, 후전량은 Parks의 수술량을 따랐다. 외직근 후전 및 하방전위술은 원거리사시각을 기준으로 외직근을 후전하면서 근거리원거리사시각 차이가 15 PD 미만일 경우 1/2 근건폭으로, 15 PD 이상일 경우 양에 따라 1/2-1 근건폭으로 하방전위를 양안 동일하게 시행하였다. 외직근 근경사후전술을 시행한 경우 양안 외직근의 아래쪽은 근거리사시각을 기준으로 후전하였고 위쪽은 원거리사시각을 기준으로 후전하였다.
성별, 나이, 수술 전 최대교정시력, 구면렌즈대응치, 안축장길이 그리고 수술 전과 후 근거리 및 원거리사시각, 근-원거리사시각 차이, 상방-하방주시 사시각 차이, 입체시를 조사하였다. 사시각은 수술 전, 수술 직후, 1주 후, 6개월 후, 1년 후 측정하였고, 입체시는 수술 전, 수술 6개월 후, 1년 후 측정하였다. 수술 성공 기준은 수술 1년 후에 측정한 근거리와 원거리사시각이 10 PD 이내이며 근거리-원거리사시각 차이도 10 PD 이내인 경우로 정의하였다. 재발은 수술 1년 후 측정한 근거리 또는 원거리사시각이 10 PD 이상 외편위를 보이는 경우로 정하였고, 속발 내사시 또는 과교정은 수술 1년 후 측정한 근거리 또는 원거리사시각이 10 PD 이상 내편위를 보이는 경우로 정하였다.
본 연구는 인간 대상 연구를 위한 헬싱키 선언을 준수하였고, 생명윤리심의위원회(Institutional Review Board)로부터 승인을 받았다(승인 번호: 2204-011-114). 수술 방법에 따라 환자를 하방전위술군 및 근경사후전술군의 두 군으로 분류하여 비교분석하였다. 통계학적인 분석은 SPSS version 18.0 (SPSS Inc., Chicago, IL, USA)을 이용하였고, 두 군 간의 비교에 Student t-test 또는 Mann-Whitney U test, 각 군에서 수술 전, 수술 후 결과 비교에 paired t-test 또는 Wilcoxon signed-rank test를 사용하였으며 수술 성공, 재발과 과교정 비교에서는 Pearson chi-square test를 사용하였다. p-value가 0.05미만일 경우 통계학적으로 유의하다고 정의하였다.
결 과
총 환자 수 85명이 포함되었으며, 하방전위술군 45명과 근경사후전술군 40명이었다. 두 군에서 수술 시 나이, 성별 그리고 수술 전 최대교정시력, 구면렌즈대응치, 안축장길이, 원거리 및 근거리사시각과 근-원거리사시각 차이, 상방-하방주시 사시각 차이, 입체시는 통계적으로 유의한 차이를 보이지 않았다(Table 1).

Preoperative clinical characteristics of the patients in the two groups
수술 1년 후 하방전위술군에서 원거리사시각은 1.96 ± 8.77 PD, 근거리사시각은 5.53 ± 9.09 PD였고, 근경사후전술군에서 원거리사시각은 4.60 ± 4.99 PD, 근거리사시각은 9.03 ± 9.09 PD였으며, 두 군 간의 유의한 차이는 없었다(p=0.088, p=0.081, respectively) (Table 2). 근-원거리사시각 차이는 수술 1년 후 하방전위술군에서 3.58 ± 5.26 PD, 근경사후전술군에서 4.43 ± 5.32 PD로 두 군 간의 유의한 차이는 없었다(p=0.463) (Fig. 1). 수술 전에 비해 수술 1년 후의 원거리 및 근거리사시각, 근-원거리사시각 차이는 유의한 감소를 보였다(모두 p<0.001). 상방-하방주시 사시각 차이의 수술 전과 수술 1년 후 차이는 하방전위술군에서 수술 후 V형 사시 방향으로 0.35 ± 4.43 PD만큼, 근경사후전술군에서 수술 후 A형 사시 방향으로 1.37 ± 4.40 PD만큼 변화하는 양상을 보였고 그 차이는 유의하지는 않았다(p=0.875, p=0.117, respectively). 상방-하방주시 사시각 차이가 15 PD 이상인 유의한 V형 사시 및 10 PD 이상인 유의한 A형 사시는 관찰되지 않았다.

Postoperative ocular deviation and stereopsis
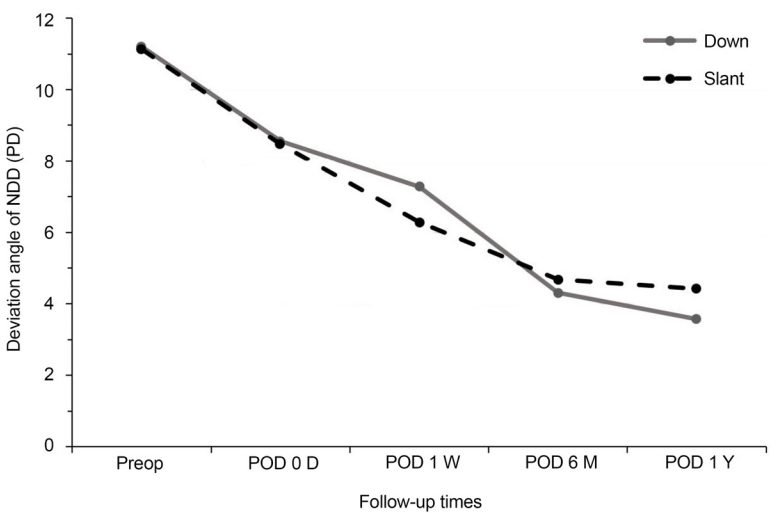
Changes of mean near-distance disparity in two groups during follow-up period. Mean near-distance disparity in two groups showed no significant difference according to the follow-up times. Down: group of patients who underwent bilateral lateral rectus recession with down transposition; slant: group of patients who underwent slanted bilateral lateral rectus recession. NDD = near-distance disparity; PD = prism diopter; Preop = preoperative; POD = postoperative day; D = day; W = week; M = month(s); Y = year.
입체시는 하방전위술군에서 수술 전 176.51 ± 471.54 seconds, 수술 1년 후 65.78 ± 63.12 seconds였고, 근경사후전술군에서 수술 전 109.17 ± 181.40 seconds, 수술 1년 후 48.38 ± 28.34 seconds였다(Table 2). 자연로그를 이용하여 계산한 LogArcsec 값은 수술 전에 비해 수술 1년 후 호전되었고 하방전위술군에서는 유의한 차이가 없었으나(p=0.053) 근경사후전술군에서는 그 차이가 유의하였다(p=0.014). 수술전과 수술 1년 후 logArcsec 값은 두 군 간의 유의한 차이는 없었다(p=0.498, p=0.054, respectively) (Table 2).
수술 1년 후 하방전위술군에서 수술 성공은 45명 중 25명으로 수술 성공률은 55.6%였고, 재발은 17명(37.8%), 과교정은 3명(6.7%)이었다. 근경사후전술군에서 수술 성공은 40명 중 21명으로 수술 성공률은 52.5%였고, 재발은 18명(45.0%), 과교정은 1명(2.5%)이었으며 두 군 간의 수술 성공률은 유의한 차이는 없었다(p=0.778) (Table 3). 두 군 모두에서 경과 관찰 기간 중에 회선사시, 수직사시, 안구운동 제한 등의 합병증은 발생하지 않았다.
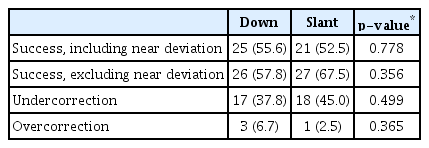
Surgical outcomes at 1 year after surgery
고 찰
눈모음부족형 외사시는 근거리사시각이 원거리사시각에 비해 10 PD 이상 큰 경우이며 시기능 훈련이나 프리즘 안경 착용과 같은 비수술적 치료를 통해 증상을 경감시킬 수는 있으나 심한 경우에서는 수술적 치료가 필요하다[1-3]. 기존의 외사시 수술 방법으로는 근거리 부족교정 및 원거리 과교정 가능성이 높고 수술 성공률도 만족스럽지 못하였고, 이후 다양한 수술적 방법들이 시도되고 있다[4-7].
Choi and Hwang [9]은 원거리사시각 기준으로 외직근을 후전하고 근거리사시각 기준으로 내직근을 절제하는 증량한 단안 외직근후전술 및 내직근절제술 시행 시 평균 27개월 후 43%의 수술 성공률을 보였다고 보고하였다. 한 눈 가림 전의 근거리사시각과 한 눈 가림 후 원거리와 근거리사시각의 평균으로 보정한 수술량을 기준으로 한 양안 외직근후전술도 소개된 바 있으며 수술 후 12개월째의 수술 성공률이 70.8%로 증량한 단안 외직근후전술 및 내직근절제술과 유사한 수술 성공률을 보였다[10].
Scott [24]은 제1안위에서는 외직근의 위아래 근섬유 길이가 같으나 근거리 및 하방 주시시에는 아래쪽 근섬유가 위쪽 근섬유에 비하여 더 수축된 상태가 되므로, 외직근의 아래쪽 근섬유를 위쪽 근섬유보다 더 후전시키면 근거리외사시를 줄일 수 있다는 가설을 제기하였다. Snir et al [11]은 단안 또는 양안 외직근 근경사후전술 시 91.6%의 수술 성공률을 보였고, 저자들의 이전 보고에서는 단안 외직근 근경사후전술 시 86.7%의 수술 성공률을 보였다[12]. 최근 보고에 따르면, Kwon and Lee [13]는 양안 외직근 근경사후전술 후 평균 24개월째에 58.5%의 수술 성공률을 보였고, Ren et al [14]은 양안 외직근 근경사후전술 후 평균 16개월째에 70.6%의 수술 성공률을 보였다고 보고하였다. 양안 내직근 근경사절제술은 처음 시도될 당시에는 효과적이라고 하였으나 이후 국내 보고에 따르면 부족교정 가능성이 많다고 보고하였다[15-17].
Buckley [8]는 기존에 A형 또는 V형 사시수술에서 시행했던 수평직근의 하방 또는 상방전위술을 이용하여 외직근후전술 또는 내직근절제술을 시행하였고 의도적으로 수술 후 V형 사시를 유도하여 주로 하방 주시를 하게 되는 근거리 작업 시 외사시가 상대적으로 감소하게 할 수 있다고 보고하였다. Kushner [18] 또한 동일한 방법으로 7명의 환자를 대상으로 6-7 PD의 V형 사시를 유발하여 근거리사시각을 감소시켰다고 보고하였다.
본 연구에서는 수술 전에 비해 수술 1년째에 원거리 및 근거리사시각과 그 차이의 유의한 감소를 보였고, 수술 1년 후 수술 성공률은 하방전위술군에서 55.6%, 근경사후전술군에서 52.5%로 두 수술 방법 간의 유의한 차이는 없었다. 상방-하방주시 사시각 차이는 하방전위술군에서 수술 후 V형 사시 방향으로, 근경사후전술군에서는 수술 후 A형 사시 방향으로 변화하는 양상을 보였으며 그 차이는 통계적으로 유의하지는 않았고, A, V형 사시의 정의에 합당할 정도로 진행한 경우는 없었다. 수술 성공 기준에서 근거리사시각을 제외한 수술 성공률은 하방전위술군에서 57.8%, 근경사후전술군에서 67.5%로 유의한 차이를 보이지는 않지만(p=0.356), 근거리사시각을 포함한 수술 성공률과 달리 하방전위술군보다 근경사후전술군에서 더 높은 수술 성공률을 보였다. 근경사후전술군에서 수술 1년 후 근거리사시각이 9.03 ± 9.09 PD로 수술 성공 기준치에 가까웠기에 이러한 결과를 보인 것으로 생각된다.
근경사후전술시 제1안위에서 아래쪽 근섬유가 정상적인 수축 상태를 유지하지 못하고 과도하게 이완된 상태가 되고 이 경우 수술 후 수주 이내에 일어나는 근섬유분절의 재형성(sarcomere remodeling)으로 외직근의 위쪽과 아래쪽에 가해지는 근육 긴장도가 같아져 근경사후전술의 효과가 감소될 수 있고 하방전위술의 경우에는 제1안위에서는 정상적인 수축 상태를 유지하지만 하방주시 시 아래쪽 근섬유가 과도하게 이완된 상태가 되기에 근경사후전술에 비해서는 근섬유분절의 재형성이 일어나지 않을 것이라고 보고된 적이 있다[18,26]. 본 연구에서도 차이가 유의하지는 않았지만 근경사후전술보다 하방전위술군에서 근-원거리사시각 차이가 더 많이 감소하는 양상을 보였고 수술 1년 후의 상방-하방주시 사시각 차이도 하방전위술군에서 더 V형에 가깝게 나타난 것으로 보아 근섬유분절의 재형성에 따른 두 수술 방법 간의 예후 차이가 있을 것으로 생각된다.
본 연구의 제한점으로는 후향적 연구 및 단일기관 연구로의 제한점이 있고 수술 후 경과 관찰 기간이 1년이므로 더 장기간의 대규모 연구가 필요할 것으로 생각된다.
결론적으로 눈모음부족형 외사시에서 양안 외직근 후전 및 하방전위술과 양안 외직근 근경사후전술 모두 원거리 및 근거리외사시, 근-원거리사시각 차이를 교정하는데 효과적이었으므로 두 방법 모두 눈모음부족형 외사시의 일차 수술로써 고려해 볼 수 있으리라 생각된다.
Acknowledgements
This work was supported by a 2-year Research Grant of Pusan National University.
Notes
Conflicts of Interest
The authors have no conflicts to disclose.
References
Biography
김성준 / Sung Joon Kim
부산대학교 의과대학 안과학교실
Department of Ophthalmology, Pusan National University School of Medicine
