유리체강 내 브롤루시주맙 주입술 후 발생한 망막색소상피파열
Tearing of the Retinal Pigment Epithelium after Intravitreal Injection of Brolucizumab
Article information
Abstract
목적
망막색소상피박리가 동반된 결절맥락막혈관병증에서 유리체강 내 브롤루시주맙 주입술 후 망막색소상피파열이 발생하여 이를 보고하고자 한다.
증례요약
68세 남자 환자가 1주 전부터 시작된 좌안 시력저하를 주소로 내원하였다. 좌안의 최대교정시력은 0.2였다. 안저촬영과 빛간섭단층촬영에서 망막색소상피박리와 망막하액이 관찰되었다. 형광안저 혈관조영술에서 과형광 병변이 관찰되었고 인도사이아닌그린 혈관조영술에서 방사상으로 분지하는 선형의 혈관과 그 끝에 확장된 결절모양의 과형광 병변이 확인되어 결절맥락막혈관병증으로 진단하고 유리체강 내 브롤루시주맙 주입술을 시행하였다. 주사 2주 후 망막색소상피박리와 망막하액은 감소하였으나 망막색소상피파열이 관찰되었고 시력의 호전은 보이지 않았다. 이후 유리체강 내 브롤루시주맙 주입술을 추가로 2회 시행하였으며, 망막하액은 전부 호전되었고 망막색소상피박리는 감소하였으나, 최대교정시력은 0.2로 호전없이 유지되었다.
결론
망막색소상피파열은 삼출성 황반변성 환자에서 기존 항혈관내피성장인자 주입술 후 드물게 발생하는 합병증으로, 비교적 최신 약제인 브롤루시주맙에서도 발생할 수 있음을 염두에 두어야 한다.
Trans Abstract
Purpose
To report tearing of the retinal pigment epithelium (RPE) that occurred after intravitreal injection of brolucizumab for polypoidal choroidal vasculopathy (PCV) with pigment epithelial detachment (PED).
Case summary
A 68-year-old man presented to our clinic with a 1-week history of decreased visual acuity in the left eye. His best-corrected visual acuity (BCVA) was 0.2 in the left eye. Fundus photography and optical coherence tomography (OCT) revealed PED and subretinal fluid (SRF). PCV was diagnosed based on the fluorescein angiography finding of a nonspecific hyperfluorescent lesion; indocyanine green angiography revealed a branching vascular network with a dilated polypoidal hyperfluorescent lesion at the end. Thus, the patient underwent intravitreal injection of brolucizumab. At the 2-week follow-up, PED and SRF were both reduced but a tear was present in the RPE; the patient’s visual acuity had not improved. After two further intravitreal injections of brolucizumab, OCT showed decreases in SRF and PED; BCVA remained stable at 0.2 without improvement.
Conclusions
Tearing of the RPE is a rare complication that can occur after intravitreal injection of current anti-vascular endothelial growth factor agents. Clinicians should carefully consider the potential for tearing of the RPE after intravitreal injection of brolucizumab.
비교적 최근 출시한 항혈관내피성장인자 약제인 브롤루시주맙(Beovu®, Novartis, Basel, Switzerland)은 단클론 단일 사슬 단편으로 분자량이 작아 조직의 침투가 빠르고 1회 주입 시 상대적으로 많은 양의 약물을 주입할 수 있다[1]. 또한 베바시주맙(Avastin®; Genentech, South San Francisco, CA, USA)에 비하여 혈관내피성장인자 A 동형에 더 높은 결합 효능을 보이고[2], 애플리버셉트(Eylea®; Regeneron, Tarrytown, NY, USA)와 비교하여 48주의 주사 치료 후 최대교정시력 호전에서 비열등성이 확인되었고, 중심구역황반두께 감소에서 더 우수한 것이 확인되었다[3].
망막색소상피파열은 망막색소상피층이 기저막과 함께 브루크막에서 박리되며 그 파열로 인해 망막색소상피가 안으로 말려 들어가는 것으로 삼출성 황반변성에 동반된 망막색소상피박리에서 자연 경과로 생기기도 하며 그 외에 유리체강 내 항혈관내피성장인자 주입술, 레이저광응고술, 광역학치료 등의 치료 과정 중에도 발생할 수 있다[4-7]. 아직까지 국내에서 결절맥락막혈관병증으로 유리체강 내 브롤루시주맙 주입술 후 망막색소상피파열이 발생한 사례는 보고된 바가 없다. 이에 저자들은 문헌 고찰과 함께 보고하고자 한다.
증례보고
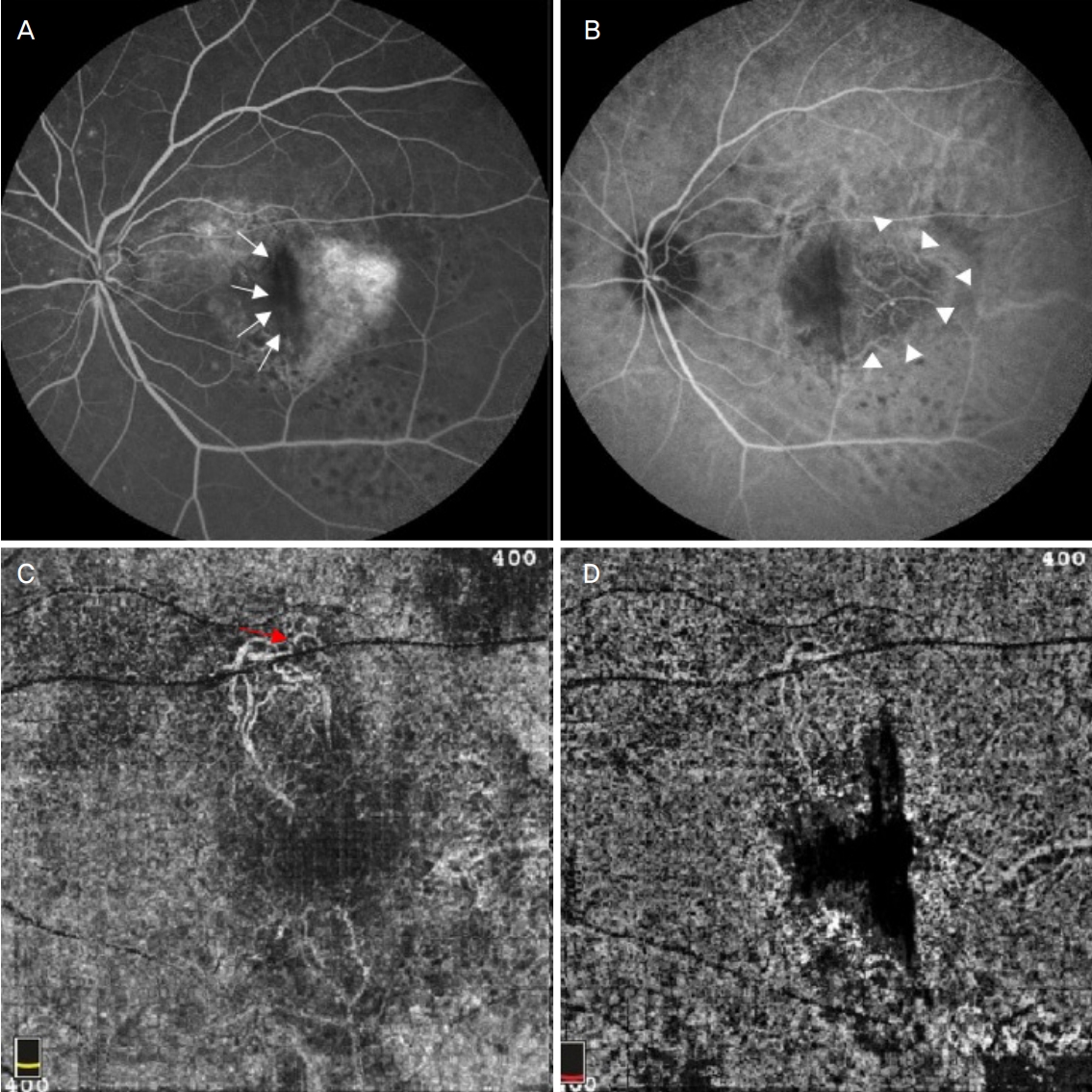
68세 남자 환자가 좌안 시력저하를 주소로 내원하였다. 좌안의 최대교정시력은 0.2였으며 안저촬영에서 황반부에 망막하출혈과 망막색소상피박리가 관찰되었다(Fig. 1A). 빛간섭단층촬영에서 망막색소상피박리와 망막하액이 관찰되었으며(Fig. 1B), 형광안저혈관조영술에서 망막하출혈로 인한 광범위한 저형광과 국소적인 형광누출이 확인되었고, 인도사이아닌그린 혈관조영술에서는 방사상으로 분지하는 선형의 혈관망과 그 끝에 결절모양의 과형광 병변이 확인되었다(Fig. 1C, D). 결절맥락막혈관병증으로 진단 후 유리체강 내 브롤루시주맙(6 mg/0.05 mL) 주입술을 시행하였다. 경과 관찰을 위해 2주 후 내원하여 시행한 빛간섭단층촬영에서 망막색소상피박리와 망막하액은 감소하였으나, 망막색소상피결손 아래에 노출된 브루크막과 그 옆으로 말린 망막색소상피층이 보이는 망막색소상피파열이 관찰되었고, 안저촬영과 빛간섭단층촬영에서도 망막색소상피파열이 확인되었다(Fig. 2A, B). 이후 2회의 추가 유리체강 내 브롤루시주맙 주입술 시행 후 망막색소상피박리는 감소하고 망막하액은 호전되었으나, 망막색소상피파열로 인해 좌안 최대교정시력은 0.2로 호전없이 유지되었다(Fig. 2C, D). 첫 번째 주사 6개월 후 망막색소상피박리의 증가와 망막내액이 확인되어 4번째 유리체강 내 브롤루시주맙 주입술을 시행하였으며(Fig. 2E, F), 첫 번째 주사 9개월까지 좌안 최대교정시력은 0.2로 유지되었다(Fig. 2G, H, 3).

Images of 68-year-old male with polypoidal choroidal vasculopathy at first visit. (A) Pigment epithelial detachment and subretinal hemorrhage were noticed in fundus photography. (B) Pigment epithelial detachment and subretinal fluid were noticed in optical coherence tomography. (C) Focal leakage and extensive hypofluorescence due to subretinal hemorrhage were noticed in fluorescein angiography. (D) Branching vascular network terminating in polypoidal lesions were noticed in indocyanine green angiography.

Two weeks after the first intravitreal brolucizumab injection (A) Retinal pigment epithelial (RPE) tear was noticed in fundus photography. (B) Exposed bruch’s membrane under the RPE defect, the rolled RPE layer, decreased pigment epithelial detachment (PED) and subretinal fluid (SRF) were noticed in optical coherence tomography (OCT). After three loading injections (C) RPE tear was prominent in fundus photography. Red arrows mark RPE tear. (D) After the reduction of SRF, nasaly rolled RPE (white arrowheads) and RPE defect with exposed bruch’s membrane (white arrows) were more prominent in OCT. Six months after the first intravitreal brolucizumab injection (E) RPE tear was noticed in fundus photography. (F) OCT showed increase in PED and presence of intraretinal fluid. Nine months after the first intravitreal brolucizumab injection (G) RPE tear was maintained in fundus photography. (H) OCT showed abscence of intraretinal fluid.
Nine months after the first intravitreal brolucizumab injection. (A) Hyperfluorescence in the area of the retinal pigment epithelial (RPE) tear and hypofluorescence in the region of rolled RPE (white arrows) were noticed in fluorescein angiography. (B) Hypofluorescence and more prominent underlying choroidal vessels in the area of PRE tear (white arrowheads) were noticed in indocyanine green angiography. (C) In outer retinal layer en face image of optical coherence tomography (OCT) angiography, hyperreflective vascular network (red arrow) was noticed, but there was no abnormal reflectivity in the area of the RPE tear. (D) In choriocapillaris en face image of OCT angiography, hyporeflective lesion due to rolled RPE was noticed.
고 찰
비교적 최근 출시된 브롤루시주맙은 단클론 단일 사슬 단편 인간화항체로 혈관내피성장인자 A 동형을 표적으로 하는 약제로 분자량이 26 kDa로, 115 kDa인 애플리버셉트나 48 kDa인 라니비주맙보다 분자량이 작고, 0.05 mL 부피인 6 mg의 브롤루시주맙은 동일 부피의 애플리버셉트 2 mg의 12배, 라니비주맙 0.5 mg의 22배에 해당하는 분자가 들어있다[8]. 또한 브롤루시주맙은 분자량이 작기 때문에 조직으로의 침투가 용이하여 약효가 빨리 나타나며, 농도가 높기 때문에 약효가 더 오래 지속된다[9]. Holz et al [9]은 유리체강 내 브롤루시주맙 주입술 이후 다음 주입술까지 기간을 라니비주맙과 비교하면 30일 연장된 것을 보고하였다. 브롤루시주맙은 애플리버셉트와 비교하여 치료 16주 이후 낮은 질병 활성도를 보였고, 48주 이후 최대교정시력 호전에서 비열등성을 보였으며, 망막하액의 감소는 보다 우수하였다[3].
망막색소상피파열은 Hoskin et al [10]이 1981년 삼출성 황반변성에 동반된 망막색소상피박리의 합병증으로 처음 보고한 이후 황반변성의 자연 경과나 유리체강 내 항혈관내피성장인자 주입술을 비롯한 황반변성의 치료 중에 발생한다고 알려져 있다[4-7]. 삼출성 황반변성 환자에서 자연적으로 망막색소상피파열이 발생할 확률은 9.4-11.5%, 유리체강 내 항혈관내피성장인자 주입술 이후 생길 확률은 3-15%로 보고되고 있다[4,11-13]. 이러한 망막색소상피파열은 전형적 삼출성 황반변성보다 결절맥락막혈관병증에서 더 낮은 빈도로 발생하는데, Pauleikhoff et al [11]은 장액성 망막색소상피 박리의 자연 경과 중 망막색소상피파열을 보인 12예 중 비혈관성 망막색소상피박리 1예, 혈관성 망막색소상피박리 9예, 결절맥락막혈관병증 2예로 보고하였고, Shin et al [13]은 유리체강 내 라니비주맙 주입술 이후 발생한 망막색소상피파열의 빈도는 전형적 삼출성 황반변성에서 3.5%, 결절맥락막혈관병증에서 0.62%로 결절맥락막혈관병증에서 낮다고 보고하였다. Yang and Kim [14]은 유리체강 내 항혈관내피성장인자 주입술 이후 발생한 망막색소상피파열 9예 중에서 전형적 삼출성 황반변성 5예, 망막혈관종증식 3예, 결절맥락막혈관병증 1예로 보고하였고, Kim and Chae [15]는 유리체강 내 베바시주맙 혹은 라니비주맙 주입술 후 발생한 망막색소상피파열 8예에서 전형적 삼출성 황반변성 6예, 결절맥락막혈관병증을 2예로 보고하였다.
유리체강 내 항혈관내피성장인자 주입술 후 발생한 망막색소상피파열의 정확한 발생 기전은 알려져 있지 않으나 문헌에 따라 다양한 보고가 있다. Chan et al [12]은 맥락막신생혈관의 수축에 의해 파열이 발생한다고 하였고, Gamulescu et al [16]은 주입술 직후 발생하는 안압 상승에 의한 것이라 하였으며, Meyer et al [17]은 유리체강 내 주입술 자체에 의한 안구 변형 및 유리체 액화와 감돈으로 야기된 유리체망막 견인력을 그 원인으로 제안하였다. Gass [5]는 맥락막신생혈관 누출로 망막색소상피박리의 정수압이 상승하여 망막색소상피가 파열된 것이라고 하였다.
브롤루시주맙을 대상으로 한 제3상 임상시험인 HAWK & HARRIER 연구에 따르면 망막색소상피파열은 브롤루시주맙을 6 mg 용량으로 주입한 730안 중 18안(2.5%)에서 발생하였고, 3 mg 용량으로 주입한 358안 중 5안(1.4%)에서 발생하여 3 mg군에서 더 낮은 빈도를 보였다[3]. Chakraborty et al [18]은 유리체강 내 브롤루시주맙 6 mg을 주입한 94안에서 망막색소상피파열은 1안(0.79%) 발생하였다고 보고하였다. 유리체강 내 베바시주맙이나 라니비주맙 주입술 후 망막색소상피파열이 발생하기까지는 평균 4-8주의 시간이 걸린다[6,14]. 본 연구에서는 유리체강 내 브롤루시주맙 주입술 후 2주 이내에 망막색소상피파열이 발생하였는데, 이는 망막색소상피의 크기가 커서 상대적으로 높은 정수압과 기저부의 높은 경사 각도가 망막색소상피층을 취약하게 만들어서일 가능성이 있으며, 브롤루시주맙의 망막하액 및 망막색소상피하액의 흡수가 다른 약제들보다 우수하여 다른 약제를 이용한 기존의 연구보다 조기에 발생하였을 가능성이 있다[5,6,9].
본 증례에서는 브롤루시주맙 6 mg 1회 주사만으로 망막색소상피파열이 발생하였지만 치료를 중단하지 않고 유리체강 내 브롤루시주맙 주입술을 3회 로딩하였다. Kim and Chae [15]는 망막색소상피파열 발생 후 추가적인 치료를 하더라도 초기 평균 4개월 정도는 시력이 유지되나 1년 경과 관찰 시 모두 불량한 시력 예후를 보였다고 하였지만, Park et al [19]은 삼출성 황반변성에서 발생한 망막색소상피파열 후 29.2개월동안 추적 관찰한 13안 중 3안(23.1%)에서는 시력이 호전되었고, 7안(53.8%)에서는 시력이 유지되었으며, 3안(23.1%)에서는 시력이 악화되었다고 보고하며, 치료를 지속하면 파열 직후보다 시력 호전은 없으나 해부학적 지표들이 호전되는 경과를 보인다 하였다. 또한 다른 연구들에서도 망막색소상피파열 발생 후 치료를 시행하지 않으면 섬유혈관성 반흔으로 진행하지만, 치료를 지속하면 망막색소상피가 파열된 부위는 위축형으로 진행되고, 시력 예후는 위축형이 섬유혈관성보다 양호하기 때문에 망막색소상피가 발생하여도 주사 치료를 지속해야하는 근거가 된다고 하였다[20,21].
본 증례는 비교적 최근에 출시된 약제인 브롤루시주맙의 유리체강 내 주입술 후 발생한 망막색소상피파열의 국내 첫 보고로서의 의미를 가지며, 유리체강 내 브롤루시주맙 주입술 후 망막색소상피파열이 발생할 수 있음을 염두에 두어야 한다.
Notes
Conflicts of Interest
The authors have no conflicts to disclose.
Acknowledgements
This study was presented as an e-poster at the 122th Annual Meeting of the Korean Ophthalmological Society 2019.
References
Biography
박준영 / Joon Young Park
대구파티마병원 안과
Department of Ophthalmology, Daegu Fatima Hospital
