위소뇌동맥류에 의한 도르래신경마비 환자
Trochlear Nerve Palsy Caused by a Superior Cerebellar Artery Aneurysm
Article information
Abstract
목적
뇌수막종으로 오인된 위소뇌동맥류에 의한 동측 도르래신경마비를 경험하였기에 보고하고자 한다.
증례요약
34세 여자 환자가 내원 7일 전부터 발생한 원거리 복시와 우측 두통을 주된 소견으로 내원하였다. 문진상 다른 전신질환이나 외상의 과거력은 없었다. 나안시력은 양안 모두 1.0이고, 상대구심동공운동장애는 없었으며, 전안부와 안저 진찰상 이상 소견을 보이지 않았다. 환자는 좌측 머리 기울임을 보이며 원거리에서 우안 상사시를 보였고, 이는 우측 머리 기울임 시 더 심해지는 양상을 보였다. 뇌자기공명영상에서 뇌수막종이 의심되는 소견을 보여 신경외과에 의뢰 후 경과 관찰이 결정되었다. 하지만 진료 1시간 후 구토를 동반한 심한 두통으로 응급실에 재내원하여 시행한 뇌혈관 전산화단층촬영상 우측 위소뇌동맥류파열로 인한 지주막하출혈 소견을 보여 응급으로 코일색전술을 시행하였다. 4주째 상사시는 약간 호전되었으나 복시가 지속되었고, 4개월째 상사시를 포함한 복시 증상이 호전되었다.
결론
위소뇌동맥류는 그 발생률이 매우 낮으며 이로 인한 도르래신경마비는 드물어 영상의학적 검사에서도 타 질환과 오인될 수 있어 복시와 두통을 동반한 경우에서 감별해야 한다.
Trans Abstract
Purpose
We report a case of trochlear nerve palsy caused by a superior cerebellar artery (SCA) aneurysm.
Case summary
A 34-year-old woman visited our clinic complaining of distance diplopia and a temporal headache 7 days in duration. She had no previous relevant medical or trauma history. Her visual acuity; intraocular pressure; and pupil, anterior segment, and fundus evaluations were unremarkable. Extraocular muscle examination (EOM) revealed six prism diopters (PD) of right hypertropia in the primary gaze; this worsened when the head was tilted to the right. Brain magnetic resonance imaging revealed a round solid nodule between the temporal lobe and pons; we thus suspected a petrous ridge meningioma. She was referred to our neurosurgery department for meningioma treatment. However, 1 hour later, she visited our emergency room with severe headache and nausea. Brain computed tomography angiography revealed a subarachnoid hemorrhage and a ruptured SCA aneurysm. Emergency coil embolization was successfully performed. Four weeks after surgery, the right hypertropia was slightly decreased. Four months later, the diplopia had disappeared and EOM revealed orthotropia.
Conclusions
SCA aneurysms are rare and can be misdiagnosed even after radiological examination. Our case emphasizes that an SCA aneurysm should be considered during the differential diagnosis of patients with diplopia and headache.
위소뇌동맥류(superior cerebellar artery aneurysm)는 소뇌동맥에 발생하는 뇌동맥류로 전체의 0.2% 정도로 낮은 발생 빈도를 보인다[1,2]. 위소뇌동맥(superior cerebellar artery)은 해부학적으로 뇌저동맥(basilar artery)에서 기원하여 중뇌와 연수 사이를 지나 소뇌로 흐르는 동맥으로 이 혈관에 발생한 동맥류는 주위 조직을 직접 압박하거나 지주막하출혈을 발생시켜 동안신경, 도르래신경, 삼차신경 등을 포함한 여러 신경학적 증상을 유발할 수 있다고 알려져 있다[1,3-5]. 국내에서는 아직까지 위소뇌동맥류로 인한 뇌신경 마비 환자의 예는 보고된 바가 없으며, 저자들은 초기에 영상의학 검사에서 뇌수막종으로 오인된 위소뇌동맥류로 인한 도르래신경마비 1예를 경험하였기에 이를 보고하고자 한다.
증례보고
34세 여자가 1주일 전부터 시작된 우측 측두부의 두통이 동반된 양안 복시를 주소로 내원하였다. 병력 청취상 전신의 기저질환, 약물 복용력, 외상, 수술 및 안과 질환의 과거력은 없었다. 초진 시 나안시력은 양안 모두 1.0이었으며 비접촉안압계를 이용해 측정한 안압은 우안 15 mmHg, 좌안 15 mmHg였다. 상대구심동공운동장애는 없었으며 세극등현미경을 통한 전안부 진찰 및 안저검사에서 회선 편위를 포함한 이상 소견을 보이지 않았다. 내원 당시 환자는 머리를 좌측으로 기울이고 있었다. 이학적 검사상 두통을 제외한 전신 증상 및 안구돌출은 보이지 않았으나 안구운동검사에서 정면 주시 시 원거리에서 6 prism diopter (PD) 의 우안 상사시, 근거리에서 4 PD의 외사위를 보였으며, 좌측 주시 시 6 PD의 우안 상사시, 우측 주시 시 2 PD의 우안 상사시를 보였다. 머리기울임검사에서 우측으로 고개를 기울이면 10 PD의 우안 상사시로 증가하였고, 좌측으로 고개를 기울이면 정위 소견을 보였다(Fig. 1). 이향운동에서는 특이 소견을 보이지 않았다. 타 병원에서 촬영된 조영제를 사용한 안와 자기공명영상에서 중등도의 부비동염 소견 외에 안와는 정상 소견을 보였으나, 우측 측두엽과 다리뇌 사이에 9.0 × 8.0 × 8.0 mm 크기의 둥근 결절이 관찰되었으며 영상의학적 판독상 추체융기의 뇌수막종이 의심되었다(Fig. 2). 다른 마비사시의 원인을 감별하기 위해 시행한 항아세틸콜린 수용체 항체, 갑상선기능검사 및 갑상선 항체, 항GD1B항체를 포함한 전신 혈액검사와 반복신경자극검사의 결과에 이상은 없었다. 임상적 증상, 혈액검사 결과 및 영상의학적 소견을 토대로 뇌수막종으로 인한 도르래신경 마비의 가능성이 높다고 판단하여 신경외과 진료를 의뢰하였으며, 뇌수막종 의증에 대해 3개월 뒤 경과 관찰을 권고 받았다. 하지만 1시간 뒤 발생한 극심한 두통과 오심, 구토로 응급실에 재내원하였다. 내원 시 동공반사는 정상이었고 수축기 혈압이 210 mmHg였으며, 의식 수준은 점점 혼미해져 응급으로 시행한 머리 뇌혈관 전산화단층촬영상 우측 위소뇌동맥류파열에서 발생한 지주막하출혈(subarachnoid hemorrhage) 소견이 보여 응급으로 뇌혈관조영술(digital subtraction angiography)을 시행하였고, 중복 위소뇌동맥 (duplication of superior cerebellar artery) 소견 및 이중에서 아래쪽 분지(inferior branch)의 박리성 뇌동맥류(dissecting aneurysm) 파열이 확인되었다. 위소뇌동맥의 위쪽 분지 및 전하소뇌동맥(anterior inferior cerebellar artery)에서의 측부순환(collateral circulation)이 충분하다고 판단되어, 동맥 류가 발생한 위소뇌동맥의 아래쪽 분지의 기시부를 포함하여, 코일색전술(coil embolization) 및 근위부혈관포착술 (proximal trapping)을 시행하였고, 시술 후 박리된 동맥류 에서의 출혈은 멈춘 것을 확인하였으며, 소뇌 부위로의 혈류 폐색도 없음을 확인한 뒤(Fig. 3), 중환자실에서 경과 관찰하였다. 치료 4주째 외래로 내원하였으며, 정면 주시 시 4 PD의 우안 상사시로 감소하고 근거리에서 정위를 보였으며 복시 증상은 여전히 지속되었다. 또한 안저검사상 우안 망막내 출혈 소견을 보였다. 추가 촬영된 뇌전산화단층 촬영에서 지주막하출혈이 현저히 감소하였고, 기존 동맥류 내로의 혈류 차단(obliteration)은 잘 유지되고 있었으며, 소뇌 및 뇌간부의 경색(infarction) 소견은 없었다. 치료 4개월뒤 원거리와 근거리에서 모두 정위로 회복되어 복시 증상은 사라졌으며, 망막출혈 소견도 호전되었다.(Fig. 4).
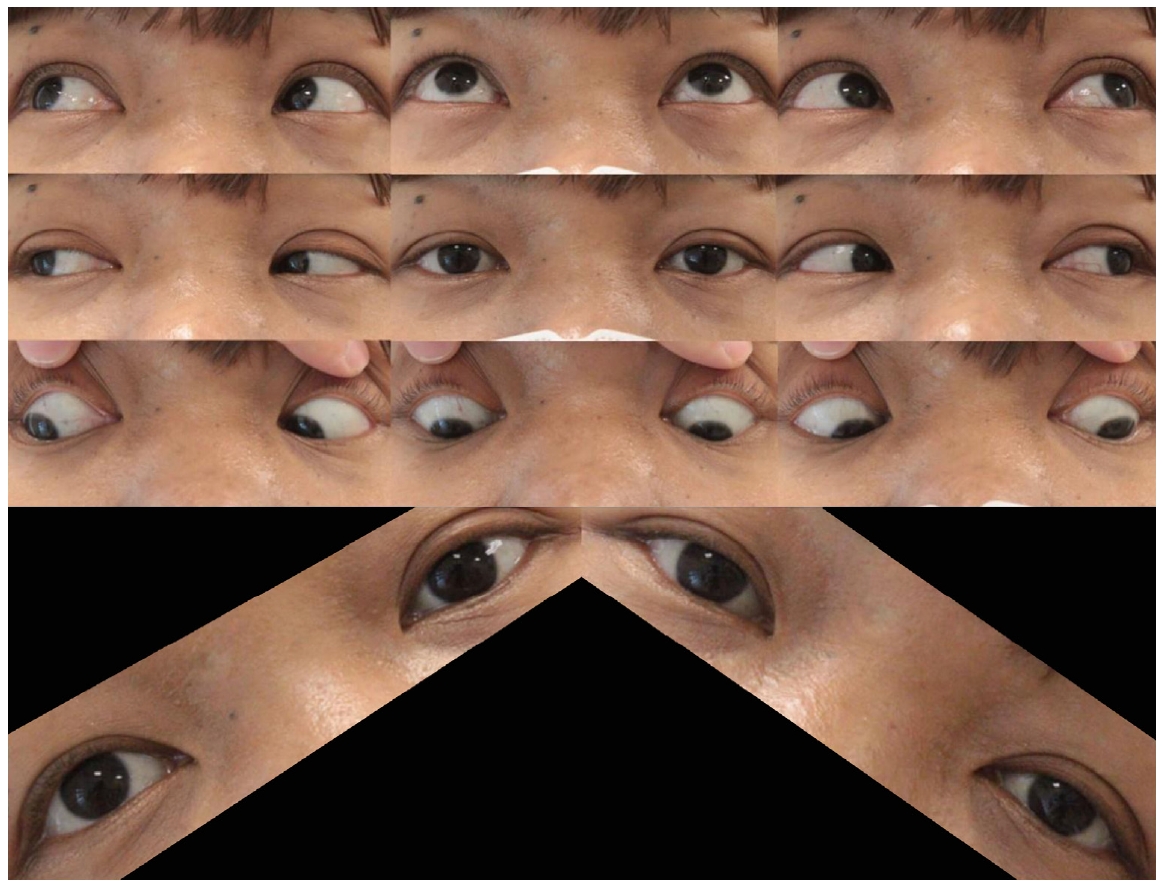
Nine gaze photo shows larger amount of right hypertropia with right head tilt.
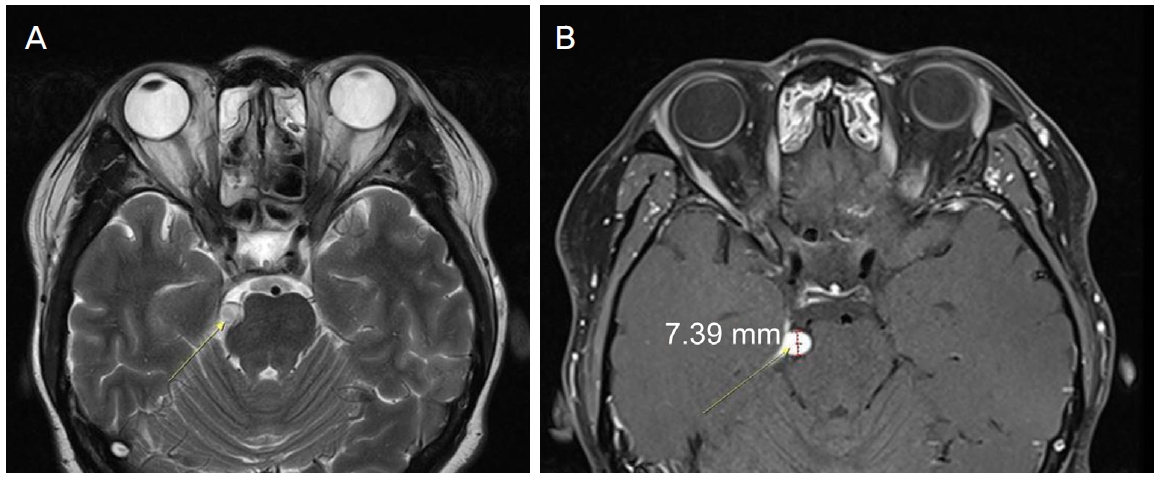
T2 weighted enhanced image (A), and T1 weighted enhanced image (B) of axial plane. Homogenous enhanced nodular lesion (about 7 mm) on the right tentorium with mild compression to anterolateral pons is shown.
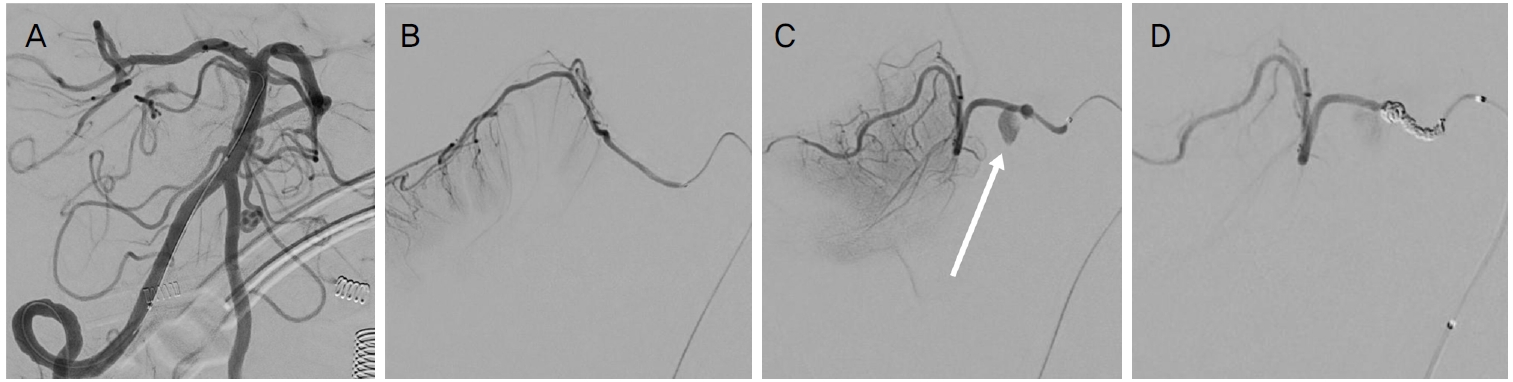
Right-sided vertebral angiogram. (A) Digital subtraction Angiography revealed duplication of superior cerebellar artery (SCA) from the right side of basilar artery. (B) Superior branch of SCA. (C) Suspected ruptured dissecting aneurysm was confirmed from inferior branch of SCA (arrow). (D) Post-operative image shows successful flow disruption into the ruptured dissecting aneurysm.
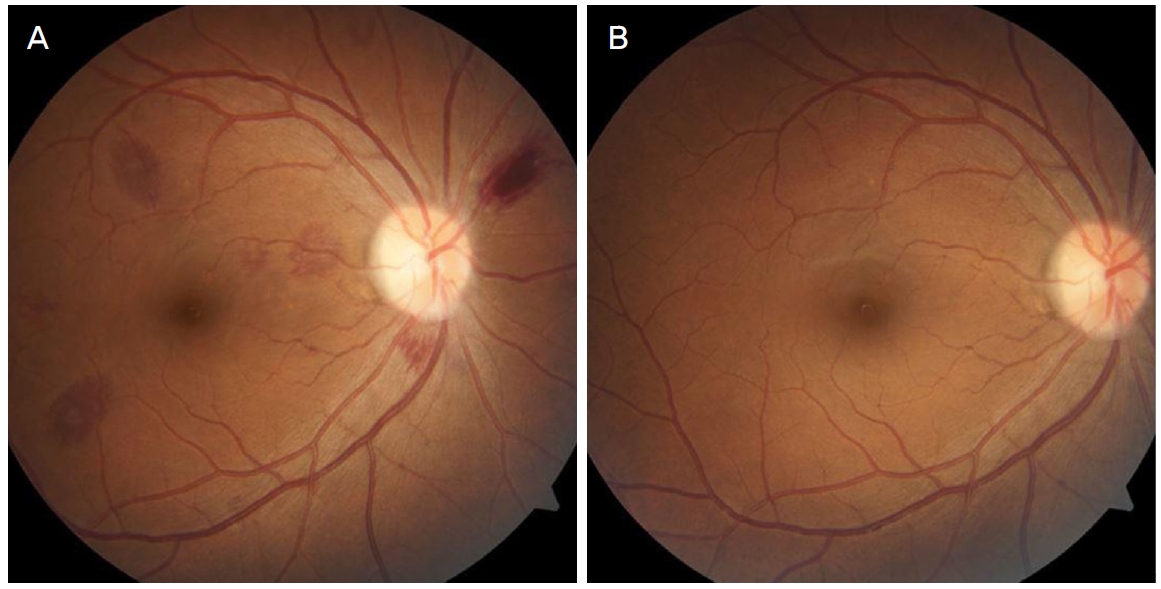
Fundus photography of the right eye of the patient, 1 month (A) and 4 months (B) after the surgery. Multiple retinal hemorrhage appeared 1 month after coil embolization but spontaneously regressed after 4 months.
고찰
위소뇌동맥은 뇌바닥동맥에서 기시하여 큰 2개의 분지를 통해 교중뇌 접합부(pontomesencephalic junction)를 지나 소뇌 상부영역에 혈액을 공급하는 혈관이다. 도르래신경은 중뇌의 도르래신경핵에서 시작해 중뇌수도회색질(periaqueductal grey)을 지나며 교차해 등쪽의 하구(inferior colliculus)를 통해 나가는 뇌간의 등쪽에서 기시하는 유일한 뇌신경이다. 이후 동안신경(oculomotor nerve) 밑으로 해면정맥동(cavernous sinus)의 이측벽을 따라 통과하여 동측의 상사근(superior oblique)을 지배한다. 위소뇌동맥은 주로 동안신경 아래로 뇌간을 감싸며 지나가고 도르래신경의 천막하 부분(infratentorial segment)과 삼차신경(trigeminal nerve)의 기시부 사이를 지나 소뇌천막(cerebellar tentorium)으로 진행한다[6,7].
도르래신경마비는 동측 상사근마비로 인해 수직복시, 회선편위, 머리기울임 등의 증상을 유발하며 그 원인을 선천적, 후천적 원인으로 나눌 수 있다. 후천적 도르래신경마비는 외상, 종양, 뇌졸중, 뇌혈관기형 및 특발성 원인 등 다양한 원인이 있으나 그중 가장 흔한 것은 두부 외상으로 알려져 있다[8].
뇌동맥류 중 위소뇌동맥류는 전체의 0.2% 정도로 유병 률이 매우 드물며, 본 증례에서와 같이 젊은 환자에서 발생한 뇌혈관박리(dissection) 등이 원인이 될 수 있다[9]. 해부학적인 위치와 동맥류의 위치에 따라 위소뇌동맥류는 동안신경, 도르래신경, 삼차신경을 압박하여 증상을 유발할 수 있다고 알려져 있다. 그중 도르래신경의 압박으로 인한 동측 도르래신경마비를 동반한 복시가 발생할 수 있으며, 일부에서는 오심과 구토를 동반한 두통이 동반될 수 있다. 이에 대해 Rusu et al [7]은 위소뇌동맥의 다양한 해부학적 이형과 도르래신경과의 연관성을 분석하여 도르래신경마비 환자에서 위소뇌동맥의 이상을 감별할 것을 권고하였다. Agostinis et al [3]은 처음으로 위소뇌동맥류가 있는 환자에서 단독으로 발생한 도르래신경마비 1예를 발표하였는데 해당 증례에서는 전신 스테로이드치료를 통해 증상이 호전된 것을 보고했다. 또한 Collins et al [10]은 발표한 증례에서 위소뇌동맥류 환자에서 발생한 동측 도르래신경마비 환자가 뇌동맥류 결찰술 이후 증상이 호전되었다고 보고하였다. 그 외에도 여러 연구에서 위소뇌동맥의 선천 장애나 동맥류로 인해 발생한 삼차 신경통과의 연관성이 보고되었으며[11,12], Hirose et al [4]의 연구에서는 25세 여성의 위소뇌동맥의 방추형동맥류(fusiform aneurysm)의 파열로 인한 반대측의 제육뇌신경 마비 1예를 보고한 바 있다.
위소뇌동맥에 발생하는 동맥류로 인한 도르래신경마비의 증례는 국내에서는 Shin et al [13]이 발표한 위소뇌동맥의 선천 기형으로 인한 도르래신경마비의 1예를 제외하고는 비슷한 증례를 찾기가 어렵다. 본 증례에서 저자들은 두통과 복시를 주소로 내원한 우측 도르래신경마비가 의심되는 환자에서 초기에 영상의학적으로 발견된 환자의 두개내 결절에 대해 그 위치가 소뇌천막(tentorium)과 연해 있었고, 동맥류의 호발 부위가 아니었기 때문에, 뇌수막종으로 오인하였으며, 동맥류의 파열을 조기에 예방할 수 없었다. 복시를 동반한 안구운동장애가 있는 환자에서 갑자기 시작된 두통이 동반되었을 때는 혈관질환의 가능성을 두고 반복적인 영상의학적 검사를 통해 감별진단으로 고려해야 할 것이다.
Notes
Conflict of Interest
The authors have no conflicts to disclose.
References
Biography
박정우 / Jeong Woo Park
성균관대학교 의과대학 강북삼성병원 안과학교실
Department of Ophthalmology, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine
