소아에서 Wavefront 수차계를 이용한 굴절검사의 유용성
Usefulness of Refractive Measurement by Wavefront Aberrometer in Children
Article information
Abstract
목적
조절마비 후 wavefront 수차계, 자동굴절검사 및 망막검영법에 의한 굴절검사를 비교하여 소아에서 wavefront 수차계를 이용한 굴절검사의 정확성과 유용성을 평가하고자 하였다.
대상과 방법
조절마비 후 wavefront 수차계, 자동굴절검사 및 망막검영법에 의한 굴절검사를 시행한 3세 이상 16세 이하 소아 65명 130안을 대상으로 하였다. 굴절검사값은 power vector (M, J0, J45) 및 원주렌즈의 절대값으로 변환하여 분석하였다. 각 검사 방법을 통한 굴절검사값 간의 일치도와 상관관계를 분석하였다. 망막검영법의 구면렌즈대응치 절대값 2 D를 기준으로 두 군으로 나누어 추가 비교하였다.
결과
수차계와 자동굴절검사 모두 망막검영법에 비해 근시성 경향을 보였다(p=0.007, p<0.001). 경도의 굴절이상을 가지는 경우, 수차계로 측정한 M, J0, J45 벡터가 망막검영법과 통계적으로 차이를 보이지 않은 반면(p=0.674, p=0.699, p=0.766), 자동굴절검사는 M, J0, J45 벡터, 원주렌즈의 절대값 모두 망막검영법과 통계적으로 유의미한 차이를 보였다(모두 p<0.05). 큰 굴절이상을 가지는 경우 수차계와 자동굴절검사를 통하여 얻은 M 벡터는 망막검영법과 비교시 근시성 경향을 보이며 통계적으로 의미 있는 차이를 보였다(모두 p<0.001).
결론
Wavefront 수차계를 이용한 굴절검사는 경도의 굴절이상을 보이는 경우 기존의 자동굴절검사보다 망막검영법에 근사한 값을 보이나, 큰 굴절이상을 보이는 경우 수차계와 자동굴절검사는 모두 망막검영법과는 차이를 보였다.
Trans Abstract
Purpose
To compare the refractive measurements from a wavefront aberrometer, autorefractor, and retinoscopy after cycloplegia in evaluating the usefulness and validity of refractive measurements by a wavefront aberrometer in children.
Methods
A total of 130 eyes of 65 children, aged from 3 to 16 years, were examined using retinoscopy, a wavefront aberrometer (OPD-Scan III), and an autorefractor (KR-1) after cycloplegia. Refractive measurements were converted to power vectors (M, J0, and J45) and cylindrical absolute values for statistical analysis. The agreement between instruments was assessed and the correlations of measurements were evaluated. Subgroup analysis was performed on two subgroups: one representing less refractive error (|M| < 2 D on cycloplegic retinoscopy) and the other with larger refractive error (|M| ≥ 2 D on cycloplegic retinoscopy).
Results
Compared with retinoscopy readings, the aberrometer and autorefractor yielded more myopic values (p = 0.007, p < 0.001). In the less refractive error group, the autorefractor results showed statistically significant differences from retinoscopy readings for M, J0, and J45 and the cylindrical absolute value (all p < 0.05); there were no statistically significant differences between M, J0, and J45 vectors of the aberrometer and those obtained using retinoscopy (p = 0.674, p = 0.699, p = 0.766). With the larger refractive error group, the M vectors of the aberrometer and autorefractor showed more myopic values than the M vector retinoscopy readings; the differences were statistically significant (all p < 0.001).
Conclusions
The wavefront aberrometer yielded refraction readings closer to those obtained with retinoscopy than the automated refraction in the less refractive error group. With a larger refractive error, statistically significant differences (all p < 0.001) were found among the aberrometer, autorefractor, and retinoscopy readings.
소아에서 정확한 굴절검사를 하기 위한 여러 시도들이 있었다. 조절력이 강한 소아에서는 조절마비 후 시행하는 굴절검사가 보다 정확한 검사로 생각되고 있으며, 조절마비 후 망막검영법이 가장 정확한 검사로, 보편적으로 소아에서의 표준 굴절검사값으로 여겨지고 있다[1-4]. 다만 조절마비 후 망막검영법에 의한 굴절검사는 비교적 많은 시간과 검사자의 숙련도가 필요하여, 조절마비 후 자동굴절검사도 외래에서 유용하게 시행되고 있다. 최근 국내 연구에서 조절마비자동굴절검사는 망막검영법에 의한 조절마비굴절검사와 높은 상관관계를 보였지만 여전히 30%의 소아에서 두 검사 간의 차이를 보여 자동굴절검사 결과를 그대로 적용하기에는 한계가 있을 것으로 보고된 바 있다[5].
파면 측정기술의 발달로 안구 전체의 광학적 지도를 Zernike 다항식을 이용하여 산출하는 wavefront 수차계가 보급되고 있으며, 이를 통하여 굴절검사값을 측정하는 것이 가능하다[6]. Zernike 다항식을 통하여 얻는 2차항은 저위 수차로, 파면에서의 구면렌즈대응치를 의미하는 defocus와 원주렌즈 값을 의미하는 astigmatism으로 구성되는 반면, 고위수차는 수차계로만 측정되는 3차항 이상의 항목으로, 수차계의 2차항을 통하여 얻은 굴절검사값은 이를 포함하지 않는다[7,8]. Wavefront 수차계를 이용하여 얻은 2차항을 구면렌즈, 원주렌즈, 축으로 표현되는 굴절검사값으로 환산할 수 있으며, 이는 망막검영법, 자동굴절검사와는 다른 새로운 방법으로 굴절검사값을 측정할 수 있는 수단이 된다. Wavefront 수차계를 이용한 굴절검사의 유용성을 증명하기 위한 여러 시도들이 있어왔다[7-11].
소아에서는 보다 정확한 굴절검사를 위한 여러 시도가 있어온 반면, wavefront 수차계를 이용하여 소아 환자에서 굴절검사를 시행한 국내 연구는 없는 실정이다. 이에 본 연구에서는 조절마비 후 wavefront 수차계를 이용한 굴절검사와 자동굴절검사, 망막검영법에 의한 굴절검사를 비교하여 소아에서의 wavefront 수차계를 이용한 굴절검사의 정확성과 유용성을 평가하고자 하였다. 본 연구는 헬싱키선언에 입각한 가톨릭대학교 연구윤리심의위원회(Institutinal Review Board, IRB)의 승인을 받아(승인 번호: SC20RASI0061) 진행되었다.
대상과 방법
2019년 5월 1일부터 6월 30일까지 본원 안과에서 조절마비 후 wavefront 수차계, 자동굴절검사 및 망막검영법에 의한 굴절검사를 시행한 16세 이하 소아 65명 130안을 대상으로 하였다. 각막질환과 망막질환이 없는 환자를 포함하였으며, 근시 억제를 위하여 조절마비제를 점안하고 있는 환자는 제외하였다. 세 가지 측정법을 모두 시행한 환아에 대하여 굴절검사값의 검사 방법 간 차이를 비교하였다.
1% cyclopentolate (Ocucyclo®; Samil, Seoul, Korea)와 0.5% phenylephrine과 0.5% tropicamide 혼합제(Mydrin P®; Santen Pharmaceutical Co., Ltd., Osaka, Japan)을 양안에 10분간격으로 3회 점안하였다. 동공확대와 빛 반사가 없는 것을 확인한 후 wavefront 수차계 OPD-Scan III (Nidek, Gamagori, Japan), 자동굴절검사(KR-1, Topcon, Tokyo, Japan)와 망막검영법에 의한 굴절검사 순서로 시행하였다. 망막 검영법에 의한 굴절검사는 1명의 숙련된 안과 의사가 검영기를 이용하여 측정한 굴절검사값을 결과치로 하였다.
조절마비 후 Wavefront 수차계, 자동굴절검사와 망막검영법에 의한 굴절검사법으로 구면렌즈, 원주렌즈, 축으로 이루어진 세 가지의 굴절검사값을 얻었으며, 이는 power vector analysis를 사용하여 분석하였다. Power vector analysis는 굴절검사값을 M 벡터, J0 벡터, J45 벡터 세 가지의 독립적인 벡터로 분리하여 분석하는 방법이다. M은 구면렌즈 대응치를, J0은 일반적인 원주렌즈 값에 대한 0° 축 벡터에서의 Jackson cross cylinder 대응치를, J45는 45° 축 벡터에서의 Jackson cross cylinder 대응치를 의미한다[12].
M=Sph+Cyl/2
J0 =(-Cyl/2) cos(2×Axis)
J45=(-Cyl/2) sin(2×Axis)
(Sph=spherical, Cyl=cylinder)
구면렌즈 대응치가 -0.75 diopters (D) 이하를 근시로, +1.00 D 이상을 원시로, 구면렌즈 대응치가 근시, 원시 기준 미만이지만 난시도수가 ± 1.50 D 이상이면 난시로, 이러한 굴절이상이 없는 경우에 정시로 분류하였다[5].
세 가지 검사 방법에 따라 구해진 M, J0, J45, 원주렌즈 절대값의 일치도를 확인하기 위하여 Bland-Altman plot을 그려보았으며, 그 연관성을 확인하기 위하여 Spearman의 순위 상관분석을 사용하였다. Friedman test를 통하여 세 가지 검사 방법에 따라 구해진 굴절검사값 간에 차이가 있음을 확인하고, 수차계와 망막검영법, 수차계와 자동굴절검사, 자동굴절검사와 망막검영법 세 가지 경우를 짝지어 Wilcoxon signed rank test를 통하여 측정법 간의 굴절검사값 크기를 비교하였다. 65명 130안 중 경도의 굴절이상을 가진 경우와 큰 굴절이상을 가진 경우 측정된 굴절검사값의 차이를 알아보기 위하여, 망막검영법의 구면렌즈대응치 M 벡터를 기준으로 절대값 2 D 미만은 Group A, 절대값 2 D 이상은 Group B로 나누어 검사 방법 간에 따라 측정된 굴절검사값의 차이를 확인하였다. 조절마비 후 망막검영법으로 얻은 굴절값의 난시를 기준으로 한 wavefront 수차계와 자동굴절검사의 double-angle polar plot상의 위치는 Eye Pro 2013: Astig PLOT (for iPhone/iPad; Apple; Cupertino, CA, USA)을 통하여 분석하였다.
결 과
세 가지 굴절검사를 모두 시행한 65명 소아의 평균 나이는 8.55 ± 2.99세로 4세에서 16세까지의 분포를 보였으며, 남아 23명(35.4%), 여자 42명(64.6%)이었다. 망막검영법 기준으로 정시 10안(7.7%), 원시 13안(10%), 근시 99안(76.2%), 난시 8안(6.2%)이었다. Wavefront 수차계와 조절마비 후 자동굴절검사와 망막검영법으로 얻은 세 가지의 굴절검사값을 power vector analysis를 사용하여 환산하였고, 원주렌즈의 절대값을 분석하였다(Table 1).
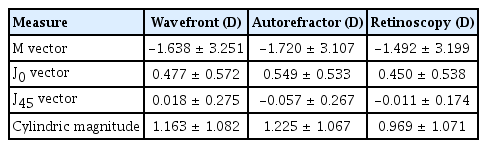
Descriptive statistics of refractive measurements
조절마비 후 Wavefront 수차계와 자동굴절검사, 망막검영법을 통하여 얻은 굴절검사값을 M, J0, J45 벡터, 원주렌즈 절대값으로 환산한 후 Spearman 순위상관분석을 통하여 검사 방법 간의 상관의 정도에 대해 분석하였다(Table 2). 수차계와 망막검영법, 수차계와 자동굴절검사, 자동굴절검사와 망막검영법 세 가지 경우를 짝지어 그 상관의 정도에 대해 분석해보았으며, M, J0, J45 벡터, 원주렌즈 절대값 네 가지 굴절검사값 모두에서 각각의 검사법이 의미있는 상관관계를 보였다(모두 p<0.001). 검사법마다 구해진 굴절검사값의 일치도를 확인하기 위하여 Bland-Altman plot을 이용해 수차계와 망막검영법, 자동굴절검사와 망막검영법 두 가지로 짝을 지어 각각 비교해보았다(Fig. 1).

Correlation analysis of the refractive measurements
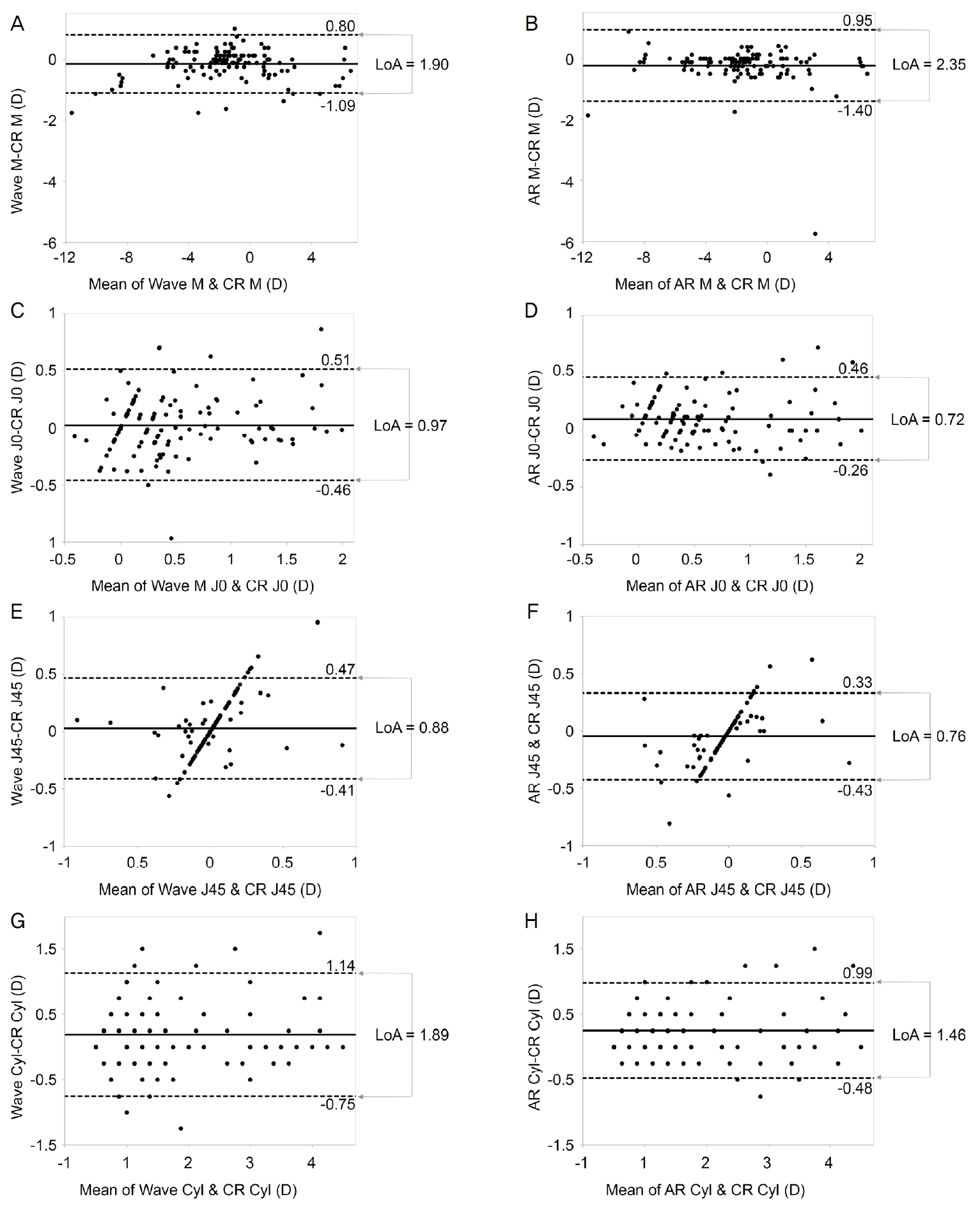
Agreement between instruments assessed using Bland-Altman plots. Bland-Altman plots showing differences of M vector, J0 vector, J45 vector and cylindrical magnitude between wavefront aberrometer and retinoscopy (A, C, E, G), autorefractor and retinoscopy (B, D, F, H). Mean difference is presented by solid lines and 95% limits of agreement (LoA) are represented by dotted lines. Wave = wavefront aberrometer; CR = cycloplegic retinoscopy; D = diopters; AR = autorefractor; Cyl = cylindrical magnitude; LoA = limits of agreement; Lower LoA = mean – 1.96 × standard deviation (SD); Upper LoA = mean + 1.96 × SD; Width of LoA = upper LoA – lower LoA; SD = standard deviation.
세 가지 검사를 통하여 얻은 굴절검사값의 비교를 위하여 M, J0, J45 벡터, 원주렌즈의 절대값 간의 차이를 분석하였으며, 망막검영법의 구면렌즈대응치인 M 벡터를 기준으로 절대값 2 D 미만은 그룹 A (63안), 절대값 2 D 이상은 그룹 B (67안)로 나누어 경도의 굴절이상을 가진 경우와 큰 굴절이상을 가진 경우 검사 방법 간의 굴절검사값 차이를 한 번 더 확인하였다(Table 3). 전체 130안에 대해 망막검영법을 기준으로 하여 비교시, M 벡터의 차이의 평균은 수차계는 -0.146 D (p=0.007), 자동굴절검사는 -0.228 D (p<0.001)로 두 검사 모두 망막검영법 대비 근시성 경향을 보였다. J0, J45 벡터의 경우 수차계와 망막검영법은 통계적으로 차이가 없었으나(p=0.239, p=0.424), 자동굴절검사의 경우 망막검영법과 통계적으로 유의미한 차이를 보였다(p<0.001, p=0.002).
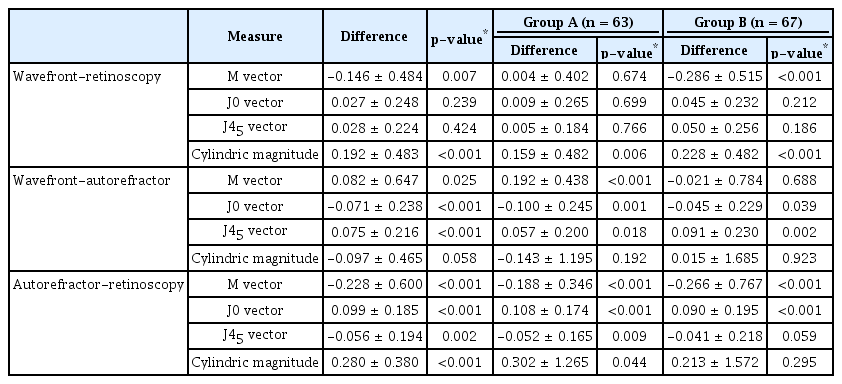
Comparison of the refractive measurements between 3 instruments. Subgroup analysis was performed on two subgroups: Group A (n = 63) represents eyes with less refractive error (|M| < 2 D on cycloplegic retinoscopy) whereas Group B (n = 67) represents eyes with larger refractive error (|M| ≥ 2 D on cycloplegic retinoscopy)
경도의 굴절이상을 가진 Group A의 경우 수차계와 망막검영법의 M 벡터 측정값 차이는 0.004 D (p=0.674)로 수차계가 망막검영법을 비교적 잘 반영한 반면, 자동굴절검사는 망막검영법과의 차이가 -0.188 D (p<0.001)로 망막검영법 대비 근시성 경향을 보였다. Group A에서 수차계를 이용한 굴절검사값은 M, J0, J45 벡터가 망막검영법과 통계적으로 차이를 보이지 않았고(p=0.674, p=0.699, p=0.766), 원즈렌즈 절대값만 수차계와 통계적으로 유의미한 차이를 보인 반면(p=0.006), 자동굴절검사를 이용한 검사는 M, J0, J45 벡터, 원즈렌즈 절대값 네 가지 검사값 모두 망막검영법과 유의미한 차이를 보였다(모두 p<0.05).
큰 굴절이상을 가진 Group B의 경우 측정된 M 벡터가 망막검영법 수차계는 -0.286 D, 자동굴절검사는 -0.266 D 차이가 있어, 두 검사 모두 망막검영법 대비 근시성 경향을 보였다(모두 p<0.001). 이 외에도, Group B에서 수차계는 원즈렌즈 절대값이 망막검영법과 통계적으로 의미 있는 차이를 보였고, 자동굴절검사의 경우 J45 벡터가 망막검영법과 차이를 보였다(모두 p<0.001).
수차계와 망막검영법, 자동굴절검사와 망막검영법 차이를 Group A와 Group B로 나누어 도식화하였다(Fig. 2). 전체 130안에 대해서는 M, J0, J45 벡터와 원주렌즈 절대값 모두에서 수차계와 망막검영법의 차이의 절대값이 더욱 작은 것으로 나타났고(Table 3), 이는 경도의 굴절이상을 보이는 Group A에서도 같은 결과를 보였으나, 큰 굴절이상을 보이는 Group B의 경우 J0 벡터를 제외한 M, J45, 원즈렌즈의 절대값 모두 자동굴절검사가 망막검영법과의 차이가 더 작았다.
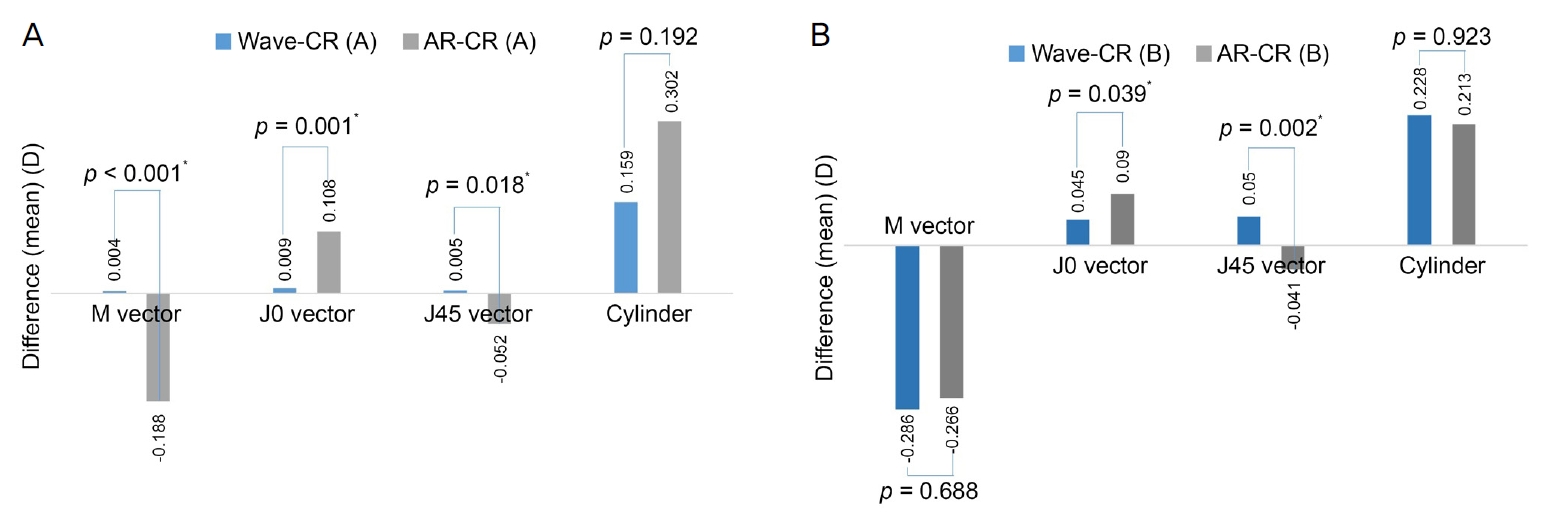
Differences of the refractive measurements between the instruments. (A) Group A (n = 63) represents eyes with less refractive error (|M| < 2 diopters (D) on cycloplegic. retinoscopy). (B) Group B (n = 67) represents eyes with larger refractive error (|M| ≥ 2 D on cycloplegic retinoscopy). Values are presented as mean difference. Wave = wavefront aberrometer; CR = cycloplegic retinoscopy; AR = autorefractor. *Cases statistically significant (p < 0.05), p-value for Wilcoxon signed rank test.
조절마비 후 망막검영법으로 얻은 굴절값의 난시를 기준으로 수차계와 자동굴절검사를 통하여 측정한 난시의 경향성을 파악하기 위하여 double-angle polar plot을 사용하였다(Fig. 3). 수차계 상의 난시는 망막검영법에 비해 0.08 D (직난시; with-the rule astigmatism 112° 방향) 편위된 값을 나타낸 반면, 자동굴절검사는 0.22 D (직난시 77° 방향)만큼 편위되어 나타나, 수차계를 통한 검사 방법상의 난시가 망막검영법을 통한 검사값에 더욱 가까운 경향을 보였다.
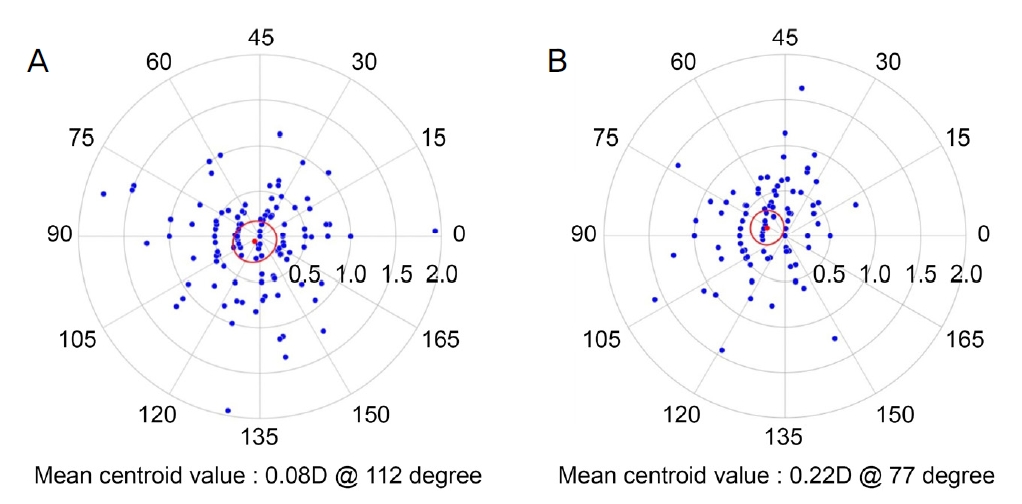
Double-angle polar plot of astigmatism. (A) Astigmatism of wavefront aberrometer analyzed based on cycloplegic retinoscopy. (B) Astigmatism of autorefractor analyzed based on cycloplegic retinoscopy.
고 찰
본 연구에서 조절마비 후 wavefront 수차계로 측정한 굴절검사값은 조절마비 후 자동굴절검사, 망막검영법으로 측정한 두 가지 검사 결과값 모두와 각각 높은 상관관계를 보였다. 조절마비 후 수차계로 얻은 굴절검사값은 망막검영법의 굴절검사값에 비해서 구면렌즈대응치를 기준으로 0.146 D 근시성 경향을 보여, 망막검영법에 비해 0.228 D 근시성 경향을 보인 자동굴절검사에 비하면 망막검영법에 더 가까운 결과를 보이는 것처럼 보였다. 다만 굴절 이상의 정도에 따라 나누어 분석해봤을 시, 경도의 굴절 이상이 있었던 경우 수차계는 망막검영법의 구면렌즈대응치와 평균 0.004 D 차이로 망막검영법을 비교적 잘 반영한 반면, 자동굴절검사는 망막검영법 대비 0.188 D 근시성 경향을 보이며 M, J0, J45 벡터, 원즈렌즈 절대값 네 가지 검사값 모두 망막검영법과 유의미한 차이를 보였다(모두 p<0.05). 구면렌즈대응치 절대값 2 D 이상의 굴절이상이 있었던 경우에는 망막검영법 대비 수차계는 0.286 D, 자동굴절검사는 0.266 D 근시성 경향을 보였다.
경도의 굴절이상을 보이는 Group A의 경우 수차계의 M, J0, J45 벡터값이 망막검영법을 통한 굴절검사값과 통계적으로 유의미한 차이가 없는 것으로 나타나, 작은 굴절이상을 보이는 경우에는 수차계가 망막검영법을 잘 반영한 것을 알 수 있다. 다만 큰 굴절이상을 가진 경우 M 벡터는 수차계, 자동굴절검사 모두 망막검영법과는 통계적으로 유의미한 차이를 보이며 근시성 경향을 보여(모두 p<0.001), 안경 처방이 필요한 큰 굴절이상을 가지는 소아에 있어서 아직은 망막검영법을 대체할 만큼의 정확한 검사 측정 장비는 없다고 할 수 있겠다.
Harvey et al [13]은 생후 6개월에서 8세 이하의 환아를 대상으로 조절마비제를 사용하지 않고 open-field Shack-Hartmann 수차계로 근거리와 원거리 주시시 얻은 굴절검사값과 조절마비 후 자동굴절검사기로 얻은 굴절검사값을 비교하였다. 이 연구에서는 수차계를 통하여 얻은 M 벡터와 원주렌즈 값 모두 자동굴절검사와 높은 상관관계가 관찰되었으며, 자동굴절검사에 비해 M 벡터는 더욱 근시성으로, 난시는 더욱 큰 절대값으로 측정되었다. 하지만 이 연구는 조절마비제의 사용 여부에 있어 본 연구와는 차이를 보인다. 본 연구는 소아를 대상으로 하였을 때, 조절마비제를 사용한 동일한 조건에서 망막검영법과 자동굴절검사, wavefront 수차계에 의한 검사를 시행한 첫 연구로 생각된다.
지난 10년간 기술의 발달로 Wavefront 수차계는 안과와 시과학 연구 분야에서 더욱 많이 사용되고 많은 연구에 적용되고 있다[14]. Wang et al [10]은 Wavescan 수차계와 Tracey 수차계로 얻은 굴절검사값과 망막검영법을 통한 굴절검사값을 비교하였을 때, 망막검영법 대비 Wavescan 수차계의 구면렌즈대응치는 0.26 D 근시성 경향을 보였고, Tracey 수차계의 구면렌즈대응치는 0.21 D 근시성 경향을 보였다. 이는 본 연구에서 wavefront 수차계가 망막검영법에 비해 0.146 D 근시성 경향을 보이는 것과 비슷한 결과이다. Park et al [8]은 같은 Wavescan 수차계로 얻은 굴절검사값과 망막검영법을 통한 굴절검사, 자동굴절검사를 비교하였다. Wavescan 수차계로 얻은 굴절검사값은 다른 두 검사를 통하여 얻은 굴절검사값과 높은 상관관계를 보였으며, 망막검영법의 굴절검사값에 비해서 구면렌즈대응치를 기준으로 0.247 D 근시성 경향을, 자동굴절검사의 굴절검사값에 비해서는 0.068 D의 근시성 경향을 가졌다. 이는 본 연구에서 wavefront 수차계를 통하여 얻은 굴절검사값이 자동굴절검사에 비해 0.082 D 원시성 경향을 보인 것과 차이가 있었으나, 큰 굴절이상을 나타낸 Group B에서는 0.021 D 근시성 경향을 보이기도 하였다.
기존 연구들에 있어서 wavefront 수차계의 근시성 경향은 측정 영역에 의한 것이라는 가설이 제시된 바 있다[15]. 각막은 중심부보다 주변부의 굴절력이 큰 양의 구면수차를 가지며, 각막의 구면수차는 나이가 들수록 증가한다고 알려져 있다. 반면 인간의 수정체의 경우 나이가 어릴수록 음의 구면수차를 가지고 있어 각막수차를 보정해주는 역할을 하나, 나이가 들수록 수정체 역시 양의 구면수차를 띄게 되므로 각막수차를 보정해주는 기능이 떨어진다고 보고된 바 있다[16-18]. 자동굴절검사의 경우 동공 중앙의 3 mm를 중심으로 측정이 되지만, wavefront 수차계의 경우 이보다 넓은 6 mm 광학부(optical zone)를 통한 측정이 이루어지고[15], 과거 연구의 경우 성인이나 백내장 환자를 대상으로 하였기 때문에 측정 영역에 따라 굴절검사값이 영향을 받을 수 있다고 볼 수도 있다. 다만 본 연구의 경우 소아를 대상으로 하였기 때문에 측정 영역에 따라 굴절검사값이 달라질 수 있다는 가설은 적용되지 않을 것으로 생각된다. 도리어 검사기기마다 측정되는 굴절검사값의 특성과 그 차이는 각 기기의 측정 과정에서 사용되는 근적외선의 파장과 근적외선에서 측정된 굴절검사값을 가시광선을 통하여 측정하였을 때 예측되는 굴절검사값으로 보정해주는 과정에서 발생하는 것으로 생각해 볼 수 있다.
본 연구에서와 같이 두 가지 검사가 일치하는지를 알기 위하여서는 각각의 검사의 재현성을 확인하는 것이 중요하지만[19], 본 연구에서는 각각의 검사를 반복하여 시행하지 않았다는 제한점이 있다. 하지만 본 연구에서 사용한 wavefront 수차계와 자동굴절검사, 망막검영법에 의한 굴절검사 세 가지 모두 재현성이 높은 것으로 알려져 있다[10,20-22]. 또한 본 연구는 모집단에 사시, 수술력이 있는 등 질병이 있는 눈과 정상안을 구분하지 않고 분석하였다는 단점이 있다. 추후에는 사시, 수술력 등 질병의 유무에 따른 굴절검사의 정확성과 재현성을 확인하는 노력이 필요할 것으로 생각된다.
결론적으로, 소아에서 조절마비 후 wavefront 수차계로 측정한 굴절검사값은 경도의 굴절이상을 보이는 경우에는 망막검영법에 의한 굴절검사값을 더욱 잘 반영하였다. 즉, 경도의 굴절이상을 보이는 소아의 경우는 망막검영법을 시행하기 어려운 경우, 수차계를 통하여 비교적 안정적인 결과를 얻을 수 있다. 다만 큰 굴절이상을 보이는 경우에는 수차계와 자동굴절검사 모두 망막검영법 수치를 충분히 반영하지 못하여, 보다 정확한 굴절검사가 필요한 큰 굴절이상을 보이는 소아에 있어 아직은 망막검영법 시행이 필수적이라고 할 수 있겠다.
Notes
Conflict of Interest
The authors have no conflicts to disclose.
References
Biography
오시은 / Si Eun Oh
가톨릭대학교 의과대학 안과학교실
Department of Ophthalmology, College of Medicine, The Catholic University of Korea
