골내 해면상혈관종에 의한 코눈물관폐쇄 및 눈물주머니 낭종의 치료
Successful Treatment of Dacryocystocele due to Secondary Nasolacrimal Duct Obstruction by Intraosseous Cavernous Hemangioma
Article information
Abstract
목적
비강내 해면상혈관종에 의한 코눈물관폐쇄 및 눈물주머니 낭종을 치료한 1예를 보고하고자 한다.
증례 요약
78세 남자 환자가 우측 내안각 부위의 종괴 및 눈물흘림 증상을 주소로 내원하였다. 종괴는 무통성의 경계가 분명하고 부드러우며 고정된 양상이었고 주사기 관류검사상 우하측 누소관의 식염수가 역류되었다. 안와 전산화단층촬영에서 우측 눈물주머니의 낭성 종괴 및 우측 비강내의 골성 병변이 전방 내측에서 코눈물관을 압박하는 소견이 보였다. 안와 자기공명영상에서는 다낭성 종괴가 우측 안와의 전내측 눈물주머니 위에 있었고, 비강내 골성 병변이 함께 보였다. 비강내 종양에 의한 코눈물관폐쇄 및 이차성 후천성 눈물주머니 낭종 진단하에 코내시경을 이용하여 눈물주머니 종괴를 완전 제거 후 코경유눈물주머니코안결술을 시행하였다. 병리검사 결과 림프 소포로 구성된 눈물주머니의 만성 염증, 비강내 종괴는 해면상혈관종으로 진단되었다.
결론
비강내 해면상혈관종에 의해 이차성으로 발생한 눈물주머니 낭종에 대해 코내시경을 이용한 종양 제거 및 눈물주머니코안연결술로 성공적으로 치료한 1예를 보고한다.
Trans Abstract
Purpose
Here, we report the clinical features and successful treatment of a very rare case of dacryocystocele due to secondary nasolacrimal duct obstruction by cavernous hemangioma in an adult patient.
Case summary
A 78-year-old man had a painless mass on the right medial canthus and epiphora for 5-6 years. The mass on the lower area of the right medial canthus had a well-defined border, was fixed in position, and smooth. Lacrimal irrigation via the lower punctum showed reflux through the opposite punctum without nasal passage. Orbital computed tomography showed multicystic mass formation on the right lacrimal sac and a bony lesion with ground glass opacity on the anteromedial side of the right nasolacrimal duct causing duct narrowing. Orbital magnetic resonance imaging showed a multicystic, fluid-filled structure in the right lacrimal sac. An intranasal bony lesion 14 mm in diameter was also observed. The patient was diagnosed with dacryocystocele due to secondary nasolacrimal duct obstruction by an intranasal mass. Endoscopic transnasal removal of two lacrimal cystic masses and the intranasal mass, and dacryocystorhinostomy (DCR) were performed. Pathological examination revealed chronic inflammation with lymphoid follicles of the tear bag and cavernous hemangioma of the nasal cavity.
Conclusions
Acquired dacryocystocele in adults is most commonly idiopathic. Here, we report a case of a dacryocystocele due to secondary nasolacrimal duct obstruction by cavernous hemangioma that was treated successfully by endoscopic transnasal tumor removal and DCR.
눈물주머니 낭종은 눈물주머니의 팽창으로 인해 내안각 아래의 낭성 부종을 동반한다. 대부분 영유아에서 선천적 원인에 의해 발생하는 질환으로 후천적 눈물주머니 낭종은 드물며 특발성, 외상, 종양, 원발성 코눈물관폐쇄, 만성 누소관염의 합병증, 부비동 종양의 치료 후 발생하는 의인성 원인 등에 의해 발생한다. 이 중에서도 후천적 눈물주머니 낭종의 가장 흔한 원인은 특발성이다[1].
성인에서 발생하는 이차성 눈물주머니 낭종은 매우 드문 질환이며, 골내 해면상혈관종 또한 전체 골종양 중 1% 미만에 불과하다[2]. 골내 해면상혈관종에 의한 이차성 코눈물관폐쇄가 동반된 1례를 보고하고자 한다.
증례보고
78세 남자 환자가 5-6년 전부터 발생한 우측 내안각 부위 종물을 주소로 내원하였다. 무통성으로 서서히 크기가 증가하였고 우안 눈물흘림 증상이 동반된다고 하였다. 고혈압의 과거력 및 7년 전 양안 백내장수술력이 있었다. 최대교정시력은 우안 0.9, 좌안 0.8이었으며 안압은 우안 9 mmHg, 좌안 7 mmHg였다.
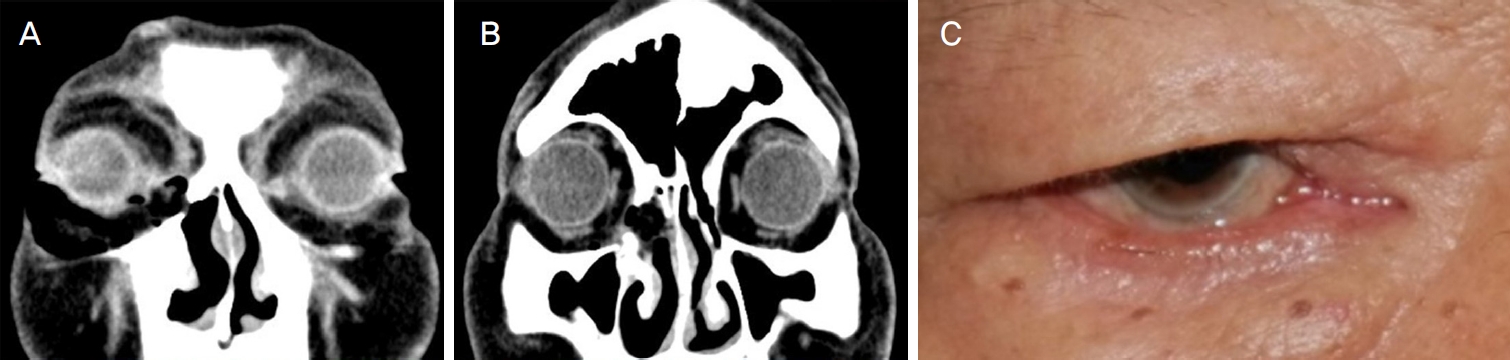
촉진상 우측 내안각 하부의 종괴는 경계가 분명하고 부드러우며 고정되어 있었으며 압통이나 발적, 화농성 분비물 등의 염증 소견은 보이지 않았다(Fig. 1). 주사기 관류검사상 우하측 누소관의 식염수는 통과되지 않고 역류되는 양상이었다. 안구운동범위는 양안 정상이었으며, Hertel 안구돌출계검사상 안구함몰이나 돌출은 없었다. 안와 전산화단층촬영에서 테두리의 조영증가를 동반한 우측 눈물주머니의 낭성 종괴가 관찰되어 눈물주머니 낭종을 시사하였다(Fig. 2A). 또한 우측 비강내의 간유리 음영의 골성 병변이 전방 내측에서 코눈물관을 압박하는 소견이 동반되었다(Fig. 2B). 안와 자기공명영상 T1 강조영상에서 균질하게 낮은 신호강도, T2 강조영상에서 높은 신호강도를 보이는 액체로 가득찬 다낭성 종괴가 분명한 경계를 띠고 우측 안와의 전내측에 자리잡고 있었다(Fig. 2C, D). 안와 전산화단층촬영에서 관찰되었던 직경 14 mm의 비강내 병변은 섬유이형성증 또는 골화성 종양이 의심되는 소견을 보였다. 이에 이비인후과의 협진수술로 코내시경을 이용하여 비강내 종괴를 제거한 후 눈물주머니 낭종 제거를 계획하였다.

Preoperative external photograph. A subcutaneous, immobile and non-tender mass is located below the right medial canthal area. The patient consented to the use of these photographs.

Preoperative orbital computed tomography (CT) and magnetic resonance imaging (MRI). Coronal scan of the orbital CT shows two cystic isodense masses formation with rim enhancement of right lacrimal sac, suggestive of dacryocystoceles (A) and bony lesion with ground glass opacity, anteromedial side of right nasolacrimal duct, causing duct narrowing, possible fibrous dysplasia (arrow, B). Orbital MRI shows two cystic, fluid-filled structure with no adjacent solid components, within the anteromedial aspect of the right orbit, in the lacrimal sac with low signal intensity on T1-weighted image (C) and high signal intensity on T2-weighted image (D).
이비인후과에서 우측 중비갑개 안쪽으로 비강내 종괴를 제거하였고(Fig. 3A), 도중에 눈물주머니 낭종이 파열되면서 비강 내로 일부 배농되었다. 본과에서 코내시경을 이용하여 2개의 크고 작은 눈물주머니 낭성 종괴를 완전히 제거하였으며(Fig. 3B), 코경유눈물주머니코안결술 및 실리콘관삽입술을 시행하였다.
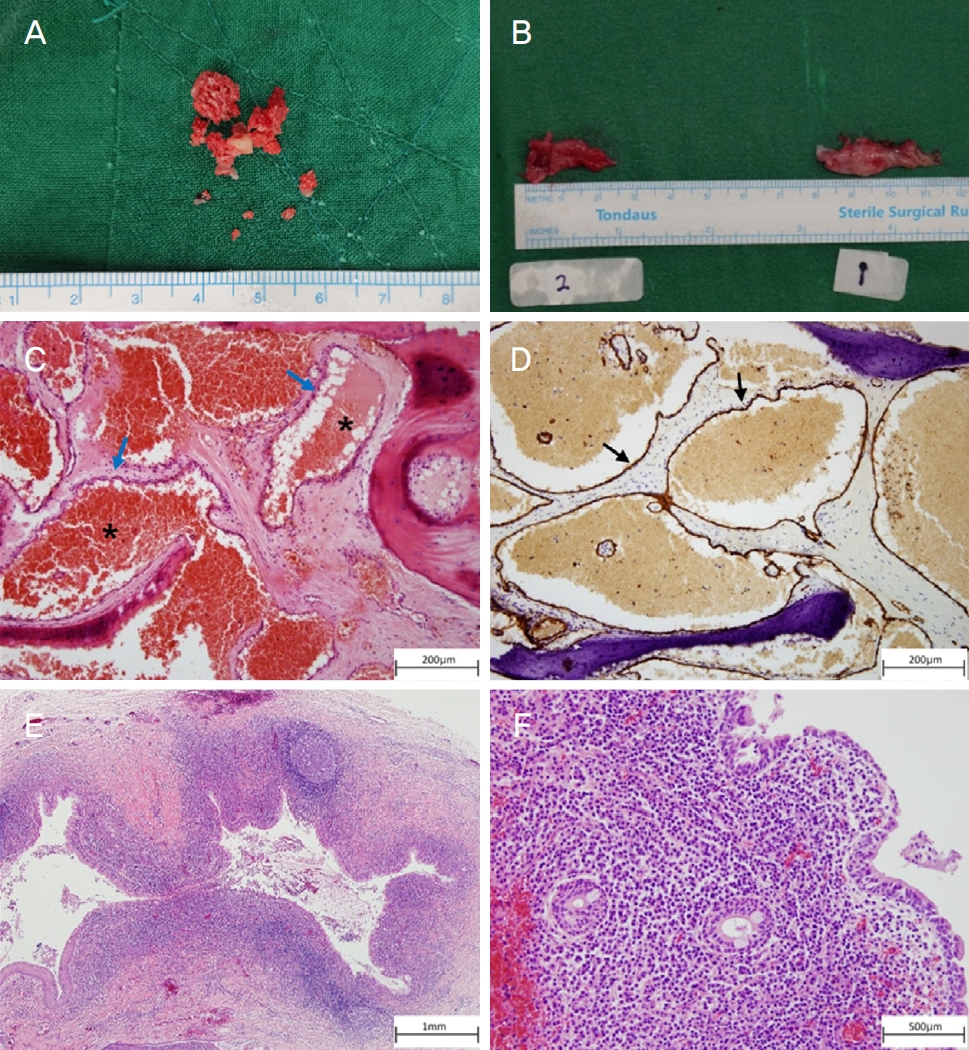
Photograph of surgical specimen and histopathologic examination. Gross examination reveals fragments of a mass in right nasal cavity (A) and two cystic masses of right lacrimal sac (B). Histopathologic findings of the mass in nasal cavity show cystically dilated vessels which are densely filled with RBCs (asterisks), lined with flattened endothelium (blue arrows) and separated by fibrous stroma (hematoxylin and eosin [H&E] staining,×100) (C). On immunohistochemical staining, the endothelial cells shows positivity for CD34 (black arrows) (×100) (D). Histopathologic findings of the masses in lacrimal sac show chronic inflammation with lymphoid follicles (H&E staining [×20, E], [×40, F]).
병리검사 결과 비강내 종괴는 크게 확장된 혈관으로 구성되어 있었는데, 이 혈관들 내부에는 적혈구가 채워져 있었고 납작하고 편평한 내피세포가 혈관내벽을 둘러싸는 형태를 띄어 골내 해면상혈관종으로 진단하였다(Fig. 3C, D). 제거한 눈물주머니낭종은 림프여포들과 림프형질세포의 침윤 소견을 보여 만성 염증으로 진단하였다(Fig. 3E, F). 눈물주머니 내부의 농을 세균배양검사한 결과 Citrobacter freundii, Klebsiella oxytoca가 동정되었다. 항생제 감수성 검사 결과에 따라 Cefepime (Maxipime®; Boryung, Seoul, Korea) 1 g 하루 2회 정맥주사, 0.5% levofloxacin hydrate (Cravit®, Santen, Seoul, Korea) 하루 3회 점안 유지하였다.
수술 후 촬영한 안와 전산화단층촬영에서 우안의 눈물주머니 낭종과 비강내 종양은 잘 제거된 소견을 보였다(Fig. 4). 술 후 3개월째 실리콘관을 제거하였고, 술 후 15개월 경과 관찰상 내안각 부위 종괴의 재발이나 눈물흘림 증상은 없었으며, 주사기 관류법 및 플루오레신 염색소실검사 시행시 눈물 배출로는 잘 유지되고 있었다.
Postoperative orbital computed tomography and external photograph of the patient. Postoperative orbital computed tomography shows complete removal of the previous dacryocystocele (A) and bony lesion in the anteromedial side of right nasolacrimal duct (B). External photograph also shows no residual mass over the area of the right lacrimal sac (C). The patient consented to the use of these photographs.
고 찰
눈물주머니 낭종의 발생 기전으로는 원위부 코눈물관의 만성 폐쇄증이 있는 상태에서 근위부의 염증이 동반되면 공통눈물소관의 개구부는 막히게 되고 양 말단이 닫힌 상태의 눈물주머니 낭종을 형성하게 되는 것이다. 이후 이차적인 눈물주머니염이 흔한 합병증으로 발생한다[3,4].
성인에서의 후천적 눈물주머니 낭종은 매우 드문 질환이며 그 원인은 특발성, 외상, 종양, 원발성 코눈물관폐쇄, 만성 누소관염의 합병증, 부비동 종양의 치료 후 발생하는 의인성 등이 있다[5]. 후천적으로 발생하는 경우 대부분 특발성이며 Lee et al [5]은 성인에서 발생한 특발성 눈물주머니 낭종 5예를 보고하기도 하였다. 최근 비골에 발생한 골내 해면상혈관종을 수술적으로 제거한 사례도 있었으나[6], 이번 증례처럼 이차적으로 눈물주머니 낭종이 발생하여 치료한 예는 국내에 보고된 바가 없다.
성인의 눈물주머니 낭종은 주로 내안각인대 아래쪽에 위치하는 눈물주머니 부근에서 무통성의 분홍 또는 파란색의 종괴로 나타나며, 코눈물관이 막힌 경우 눈물 흘림 증상이 동반되고 이차 감염이 발생한 경우가 흔하여 점액화농성 분비물이 나오고 눈물주머니염이 생기며, 심한 경우에는 안와 주위 또는 얼굴의 봉와직염이 나타나기도 한다[7].
영아에서 생긴 눈물주머니 낭종의 경우 60-80%에서 생후 8개월 이내에 자연 관해가 일어나기 때문에 마사지와 점안항생제 등의 보존적 치료를 우선 시행한다[8,9]. 보존적 치료에도 호전을 보이지 않는 경우에는 하스너판의 폐쇄를 완화하기 위해 눈물소관 탐침법을 시도해보는 것으로 알려져 있다[10]. 성인에서는 이러한 보존적 방법으로는 호전을 기대하기 힘들고 수술적 치료로 눈물주머니코안연결술을 시행하게 되는데, 일반적인 코눈물관폐쇄 환자에서의 눈물주머니코안연결술을 시행하는 경우보다 수술 성공률은 다소 낮은 것으로 알려져 있다[11]. 또한 눈물주머니코안연결술을 시행하는 경우 대부분은 피부 경유로 접근하지만 이번 증례처럼 내시경적 코경유로 접근할 경우 안면에 흉터가 생기지 않고, 눈 둘레근의 펌프 기능을 보존하며, 출혈과 회복 기간이 적다는 장점이 있다[12]. 성인의 눈물주머니 낭종의 술 후 성공률을 높이기 위해서는 전체 눈물주머니를 충분히 개구시켜야 할 뿐만 아니라 늘어난 눈물주머니 낭종을 최대한 절제함으로써 적절한 문합을 만들어주는 것이 필요하다. 그리고 구상돌기(uncinate process)가 비강을 가리는 경우에는 구상돌기의 절제도 함께 시행하여 눈물주머니 코안 연결의 개구부를 크게 함으로서 좋은 결과를 얻을 수 있을 것으로 사료된다[5,13].
결론적으로 성인에서 내안각 종괴를 보이는 경우 드물지만 눈물주머니 낭종을 고려해야 하며, 전산화단층촬영과 자기공명영상 등을 시행하여 고형 종괴 등의 원인 감별이 필요하다. 저자들은 비강내 해면상혈관종 의한 이차성 코눈물관폐쇄 증례를 경험하였고, 수술적 치료로 보통 시행하는 피부 경유가 아닌 내시경적 코경유로 접근하여 눈물주머니 낭종을 제거하고 눈물주머니코안연결술 후 좋은 결과를 얻었기에 이를 보고하는 바이다.
Notes
The contents of this paper were presented at the 122nd annual meeting of the Korean Ophthalmological Society in 2019.
Conflict of Interest
The authors have no conflicts to disclose.
References
Biography
김예원 / Ye Won Kim
가천대학교 의과대학 길병원 안과학교실
Department of Ophthalmology, Gachon University Gil Medical Center, Gachon University College of Medicine
