결막점액성기질종양
A Conjunctival Myxoid Stromal Tumor
Article information
Abstract
목적
결막에서의 발생이 드문 양성종양인 결막점액성기질종양을 치료, 경험하였기에 보고하고자 한다.
증례요약
고혈압, 뇌경색 기저병력이 있는 70세 남자가 1년 전부터 발생한 크기 변화가 없는 좌안 이측 결막의 투명한 종괴를 주소로 내원하였다. 내원 당시 시력은 정상이고, 결막 종괴 외 특이 소견은 관찰되지 않았다. 좌안에서 이측 아래쪽에 주위 조직과의 경계가 뚜렷한 4 × 3 mm 크기의 옅은 황색 젤리와 같은 투명한 종괴가 관찰되었고, 유동성은 있으나 통증 및 압통은 없었다. 종괴에 대해서는 절제생검을 시행하였다. 병리조직학검사상 풍부한 점액 모양 기질 내에 망상섬유가 위치하고 있었으며, 방추형 및 성상세포, 산포한 염증세포들이 기질 내에서 관찰되었다. 또한 면역학검사상 CD34 양성, SMA 음성의 결과가 나와서 결막점액성기질종양으로 진단되었다.
결론
임상적으로 결막에 경계가 명확하고 뚜렷한 혈관 분포나 색소 침착이 없는 옅은 황색에서 옅은 분홍색의 투명한 종괴가 관찰될 경우 결막점액성기질종양의 가능성을 고려하고 조직검사를 통해 병리학, 면역학검사 후 필요에 따라 전신질환 동반 유무를 확인해야 한다.
Trans Abstract
Purpose
We report a conjunctival myxoid stromal tumor (CMST), which is a rare benign conjunctival mass.
Case summary
A 70-year-old man with a history of hypertension and cerebral infarction visited our hospital with a clear mass of the conjunctiva in the left eye. His visual acuity was normal, and no other abnormal findings were noted. A transparent, yellowish, jelly-like, 4 × 3 mm mass with a clear border between it and the surrounding tissue was found at the lower temporal part of the conjunctiva. The mass was mobile and there was no pain or tenderness. Excisional biopsy was performed on the mass. Histopathological examination showed reticular fibers located in an abundant mucus-like matrix with fusiform, astrocytic and scattered inflammatory cells. Immunologic examination revealed CD34 positive and SMA negative findings and we diagnosed the mass as a CMST.
Conclusions
When there is a clear pale yellow to light pink mass with a clear border and a distinct vascular distribution or pigmentation in the conjunctiva, the possibility of a CMST must be considered. Histopathologic and immunologic examination should be performed through biopsy and evaluation for systemic disease should be performed as necessary.
결막에는 상피성, 낭성, 혈관성과 림프구성 등의 다양한 종양들이 존재한다. 점액종은 원시 중간엽에서 기원하는 것으로 생각되는 양성의 연조직종양이다. 점액종은 안와 구조에서는 아주 드물게 발견되며, 결막, 안와, 안검, 각막 등에서 보고된 바 있다[1-9]. 결막에서 이와 같은 중배엽세포의 증식은 결막기질종양(conjunctival stromal tumor, COST)의 일종으로 분류되고, 결막 종양 중에 <0.001%에서 발견되는 흔하지 않은 양성종양이다[7]. 결막점액종(conjunctival myxoma)의 실체를 인지함으로써 심장점액종과 같이 생명을 위협하는 악성종양에 대한 조기 발견 및 처치를 하는 것은 중요하다[5,9]. 결막기질종양(COST)은 2012년에 4개의 증례로 보고된 적 있다[5,7]. 결막기질종양(COST)은 명백한 병리조직학적 소견을 가지는 종양으로써, 방추형의 세포들과 드물게 거짓 핵들, 다핵의 거대세포들을 보이며, 부분적으로 점액종성 기질을 가지고 있으며 면역학적으로 CD34, Bcl-2, 비멘틴(vimentin)과 부분적으로 CD68 양성의 특징을 가지고 있다[5].
최근 2018년에는 결막점액종(conjunctival myxoma)과 결막기질종양(COST)의 특징을 동시에 가지면서 풍부한 점액성의 중간 기질을 가지는 종양을 결막점액성기질종양(conjunctival myxoid stromal tumor, CMST)으로 분류하였다[9]. 저자들은 병리학적으로 방추형의 세포들과 풍부한 점액성의 중배엽성 기질을 가지며 면역학적으로 결막점액종(conjunctival myxoma)과 결막기질종양(COST)의 특징을 가지는 결막점액성기질종양(CMST) 1예를 보고하고자 한다. 국내에서는 결막에서 발생한 점액종은 2례에 불과하며, 두 증례 모두 병리조직학검사를 통해 특징적인 결막점액종(conjunctival myxoma)의 양상이 관찰되어 진단되었다. 결막점액종(conjunctival myxoma)의 진단은 특징적인 병리조직학적 소견을 통해 가능하며, 조직 소견이 명확하지 않은 경우에서는 필요에 따라 병리과에서 면역학적 검사를 통해 지방종, 결막낭, 신경섬유종, 신경초점액종, 멜라닌결핍모반(amelanotic nevus), 멜라닌결핍흑색종(amelanotic melanoma), 편평세포암종과 감별하게 된다. 국내에서 보고된 2례는 결막점액성기질종양(CMST)이라는 개념이 확립되기 전의 증례로 국내에서는 면역학검사를 시행하여 결막에서 발생한 점액종을 감별한 적은 없다. 본 증례는 면역학검사를 통해 적극적으로 결막종양의 감별을 시도하여 결막점액성기질종양(CMST)으로 진단하였기에 이를 보고하고자 한다.
증례보고
고혈압, 뇌경색 기저병력 있는 70세 남자가 1년 전부터 발생한 크기 변화가 없는 좌안 이측 쪽 결막의 투명한 종괴를 주소로 내원하였다. 내원 당시 교정시력 좌안 1.0, 결막 종괴 외 특이 소견은 관찰되지 않았다. 좌안에서 이측 아래쪽에 주위 조직과의 경계가 뚜렷한 4 × 3 mm 크기의 옅은 황색 젤리와 같은 비교적 투명한 종괴가 관찰되었고, 만졌을 때 유동성이 있었고, 통증 및 압통은 없었다(Fig. 1). 다른 전안부검사 및 안저검사는 정상이었다. 좌안 결막 종괴에 대해 절제생검을 시행하였다. 병리조직학검사상 풍부한 점액 모양 기질 내에 망상섬유가 위치하고 있었으며, 방추형 및 성상세포, 산포한 염증세포들이 기질 내에서 관찰되었다. 또한 면역학검사상 CD34 양성, SMA 음성의 결과가 나와서 결막점액성기질종양(CMST)으로 진단되었다(Fig. 2). 환자에게 전신 평가를 권유하였고, 1년까지 추적 관찰하였을 때 재발을 포함하여 특이할 만한 합병증 전신질환은 발견되지 않았다(Fig. 3).
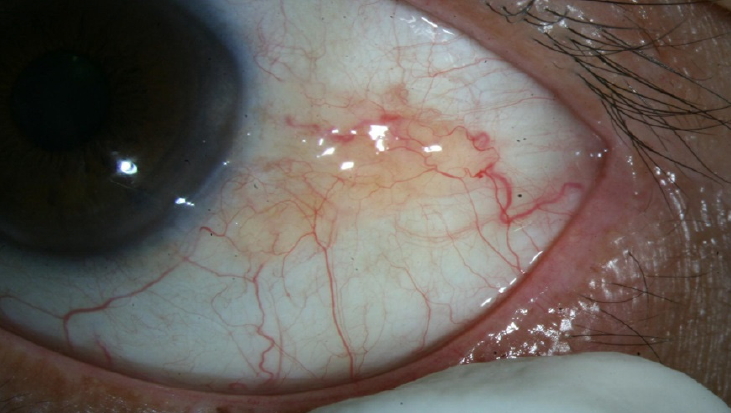
A yellow-pink subconjunctival mass lesion was noted on temporal bulbar conjunctiva on the left eye. The mass was a firm cystic lesion fixed (4 × 3 mm) to the palpebral conjunctiva. Though there were no posterior feeder vessels, fine intrinsic tumor vascularity was present. Extraocular movements were full and painless.

Conjunctival myxoid stromal tumor. (A) Spindle-shaped and stellate-shaped cells, few vascular structures, and basophilc loose mucinous matrix (haematoxylin and eosin, ×200). (B) Mucoid matrix stains positively with mucicarmine (×200). (C) Tumor cells were positive for CD34 (immunostaining marker for vascular endothelial cells, hematopoetic stem cells, and some soft tissue tumors) (×200). (D) Tumor cells were negative for SMA immunostaining (×200).
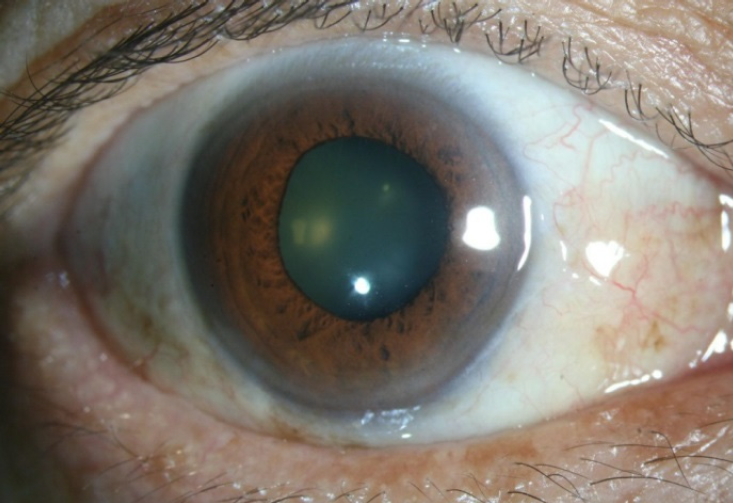
The clinical photographs of the left eye 6 months after the operation. The incision scar disappeared and there was no sign of recurrence.
고 찰
결막은 안구 표면을 싸고 있는 반투명한 점막조직으로 눈물층을 비롯한 안구표면 유지에 매우 중요한 역할을 한다. 다양한 세포를 포함하고 있는 결막은 인체의 다른 점막조직에서 발생하는 종양과 비슷한 양상의 종양이 발생하지만, 다른 점막조직과는 달리 햇빛이나 여러 외부 자극에 노출되어 있어 다른 형태의 종양이 발견되기도 한다. 결막 종양을 구분화시킴으로써 임상과정을 예측해볼 수 있으며 다른 전신질환의 평가의 중요성을 강조할 수도 있다[1-4,6-8].
결막에서 중배엽 세포의 증식은 흔하지 않으며, 결막에서 발견되는 종양인 지방종, 결막낭, 신경섬유종, 신경초점액종, 멜라닌결핍모반(amelanotic nevus), 멜라닌결핍흑색종(amelanotic melanoma), 편평세포암종 등과 감별되어야 한다[5,7,9]. 중배엽에서 기원하는 결막점액종(conjunctival myxoma)은 안와 조직에서 매우 드물게 발생하며, 특히 결막에서는 거의 발생하지 않아 결막에 발생하는 종양의 <0.001%의 빈도로 보고되고 있다[7]. 병리학적으로 명백하게 방추형의 세포들과 드물게 거짓핵들, 다핵의 거대세포들을 보이며, 부분적으로 점액종성 기질을 가지고 있으며 면역학적으로는 CD34, Bcl-2, 비멘틴(vimentin)과 부분적으로 CD68 양성의 특징을 가지는 결막점액종(conjunctival myxoma)을 결막기질종양(COST)으로 정의한 바 있다[5,7]. 결막기질종양(COST)은 항체검사들 중 CD34, Bcl-2, 비멘틴(vimentin)에서는 대부분 양성 소견을 보였으며, CD68에서는 부분 양성, Ki-67에 대해서는 매우 낮은 비율의 양성, S100, SMA, 미오신(myosin), 데스민(desmin)과 액틴(actin)에서는 음성 반응을 보인다고 한다[5,7]. 이를 바탕으로 결막점액종(conjunctival myxoma)과 결막기질종양(COST)의 특징을 동시에 가지면서 풍부한 점액성의 중간 기질을 가지는 결막종양을 결막점액성기질종양(CMST)으로 정의하게 된다[9]. 결막점액성기질종양(CMST)은 결막점액종(conjunxtival myxoma) 또는 결막기질종양(COST)의 독특한 임상 병리학적 특징을 나타내는 용어로, 이러한 용어의 확립은 다른 결막종양들을 감별하여 치료의 방향을 결정하는 데 도움이 될 것이다.
결막점액성기질종양(CMST)은 전형적으로 경계가 뚜렷하며, 분홍색의 투명한 낭성 종괴로 나타나지만, 경계가 불 분명하거나 종괴의 색이 노란색 또는 하얀색으로 나타날 수 있다. 특징적 조직병리학적 소견으로 방추형의 세포들과 레티큘린 섬유들이 풍부한 점액성 기질 내에 관찰된다. 점액 기질은 히알루론산(hyaluronic acid)가 대부분을 차지하며, 황산 콘드로이틴(chondroitin sulfate)이 적은 양으로 포함되어 있다. 현미경으로 관찰 시, 세포질 내 공포와 세포질 미세섬유가 성긴 다발로 엉켜있는 것을 볼 수 있다. 공포는 조면 소포체 및 함입된 핵막주름으로 이루어져 있다. 여러 항체검사들 중 특히나 CD34, 비멘틴(vimentin), Bcl-2가 결막점액성기질종양(CMST)의 강한 표지자일 수 있으며[5,9], 본 증례에서는 여러 면역 검사들 중 CD34 양성과 SMA 음성 반응을 확인하였다. CD34는 주로 미성숙한 중간엽 줄기세포(mesenchymal stem cells)에서 염색되며, CD34 양성을 통해 결막에서 중간엽 세포 증식이 있음을 확인할 수 있었으며, SMA 음성을 통해 근육섬유모세포종양(myofibroblastic tumor)이 아님을 확인하였다.
양상병리학검사를 통해 진단된 결막점액종(conjunctival myxoma)중 CD34, 비멘틴(vimentin), Bcl-2 면역학검사를 의뢰함으로써 결막점액성기질종양(conjunctival myxoid stromal tumor, CMST)의 진단에 도움을 줄 수 있을 것이며, 본 증례에서는 비멘틴(vimentin), Bcl-2 검사를 시행하지 못하였지만 면역학검사를 시도함으로써 결막종양을 감별하여 치료의 방향을 결정하고자 하였기에 이를 보고하는 바이다.
결막점액성기질종양(CMST)의 최적 치료는 절제 생검이다. 결막 및 각막점액종의 절제 생검 후 재발이나 악성화는 보고된 바가 없다[9]. 점액종은 원시 중배엽과 비슷한 양상을 보이는 드문 양성종양으로 신체 어디에나 발생할 수 있으나 주로 근골격계나 심장, 피부, 비뇨생식계에 발생하여 전신질환으로는 Carney 증후군, Mazabraud 증후군, McCuneAlbright 증후군 등의 일부로 발견될 수 있다. 그중 Carney 증후군에서 심장점액종에 의한 증상이 나타나기 전, 안과 소견이 먼저 발현될 수 있기 때문에 특히나 안과 소견을 발견한 경우 Carney 증후군과의 연관성에 대한 인식이 필요하며 추가적인 전신검사가 중요하다[10]. Carney 증후군은 상염색체우성질환으로, 점막피부의 다발성 색소침착, 심장 및 심장 외 점액종, 내분비 과활성, 뇌하수체 선종, 비전형 고환종양, 멜라닌성수초종(psammomatous melanotic schwannoma) 중 2가지를 보일 때 진단한다. 눈꺼풀 늘어짐, 결막 색소침착, 눈꺼풀 또는 결막점액종(conjunctival myxoma)과 같은 임상학적 증상이 초기에 동반될 수 있으며Carney 증후군 환자들은 심장 점액종과 관련하여 색전 현상을 겪는 경우가 많으며 결막점액종(conjunctival myxoma)의 조기 발견은 이러한 위협적인 악성종양을 예방하는 데 도움이 된다. 따라서 점액종이 진단되었을 때에는 Carney 증후군의 진단을 위해 심초음파, computed tomography (CT), magnetic resonance imaging, 고환 초음파, thyroid stimulating hormone (TSH), adrenocortical hormone (ACH), growth hormone (GH) level을 포함한 전신검사를 시행해볼 수 있다[3,5,6,9]. 본 증례의 경우는 환자의 나이, 기저질환을 고려하여 심초음파, 복부CT를 시행하였고 상기 검사에 대한 이상 소견은 관찰되지 않아 감별진단이 가능하였다. 결막점액성기질종양(CMST)은 매우 드물지만, 결막의 경계가 명확한 뚜렷한 혈관 분포나 색소침착이 없는 옅은 황색 또는 옅은 분홍색의 움직이는 종양을 감별진단할 때에는 이를 염두에 두어야 하며, 진단이 되고 나면 제거 후 재발이나 악성화는 드물지만 다른 전신질환 동반 유무를 확인해야 한다.
Acknowledgements
The work was supported by a 2-year research (2019.3.1-2021.2.28) grant of Pusan National University.
Notes
Conflict of Interest
The authors have no conflicts to disclose.
References
Biography
김휘경 / Hui Kyung Kim
부산대학교병원 안과
Department of Ophthalmology, Pusan National University Hospital
