새로운 비접촉안압계 HNT-1P의 신뢰성: 안압, 중심각막두께, 교정안압에 대한 비교
New Non-contact Tonometer HNT-1P Reliability: Comparing Intraocular Pressure, Central Corneal Thickness, and Corrected Intraocular Pressure
Article information
Abstract
목적
새로운 비접촉안압계 HNT-1P의 안압, 중심각막두께, 교정안압을 각각 골드만압평안압계로 측정한 안압, 초음파 각막두께측정계로 측정한 중심각막두께, 이 두 측정치를 이용하여 산출한 교정안압과 비교하여 신뢰도 및 임상적 유용성을 평가하고자 하였다.
대상과 방법
정상안 또는 녹내장 의증 65명 120안을 대상으로 하였다. HNT-1P로 안압과 중심각막두께를 측정하였으며 이어서 골드만압평안압계로 안압과 초음파 각막두께측정계로 중심각막두께를 측정하였다. 골드만압평안압을 초음파 중심각막두께로 보정하여 교정안압을 산출하였다. HNT-1P와 대조기기들 간의 상관관계를 Pearson 상관분석으로 알아보았으며 일치도를 Bland-Altman plot 분석으로 확인하였다.
결과
HNT-1P와 골드만압평안압계로 측정한 평균 안압 간의 상관계수는 0.964 (p<0.001)였다. HNT-1P와 초음파 각막두께측정계의 측청치 평균중심각막두께 측정치 사이의 상관계수는 0.913 (p<0.001)이었다. HNT-1P와 골드만압평안압계로 확인한 평균 교정안압 측정치 사이는 0.956 (p<0.001)의 상관계수를 보였다. Bland-Altman plot 분석에서 HNT-1P와 각 대조기기 간의 높은 일치도를 보였다.
결론
새로운 비접촉안압계 HNT-1P는 골드만압평안압계와 초음파 각막두께측정계와 비교하여 높은 일치도 및 신뢰도를 보여 정확한 안압, 중심각막두께, 교정안압을 제공할 수 있을 것으로 보인다.
Trans Abstract
Purpose
To assess the reliability of a new non-contact tonometer, HNT-1P, by comparing its intraocular pressure (IOP), central corneal thickness (CCT), and corrected IOP (cIOP) measurements with the IOP measured by Goldmann applanation tonometry (GAT), the CCT measured with ultrasound pachymetry (USP), and the cIOP derived from GAT IOP and USP CCT.
Methods
A total of 120 eyes of 65 healthy or glaucoma suspects were included in this study. The IOP was measured with the HNT-1P and GAT. The CCT was determined using the HNT-1P and USP. The IOP measured with GAT was corrected according to the CCT measured by USP. The correlations of the measurements obtained with the various instruments were evaluated using Pearson’s correlation coefficient, and the agreement was assessed using Bland-Altman plots.
Results
The average IOP measured with the HNT-1P and GAT was 14.8 ± 5.1 mmHg and 15.6 ± 5.2 mmHg, respectively, and the correlation coefficient between the two IOP measurements was 0.964 (p < 0.001). The mean CCT was 553.5 ± 27.4 μm using the HNT-1P and 550.6 ± 26.3 μm using USP, and the correlation coefficient between the two measurements was 0.913 (p < 0.001). The average cIOP was 14.6 ± 5.0 and 13.4 ± 6.5 mmHg according to the HNT-1P and GAT, respectively, and the correlation coefficient between the two corrected measurements was 0.956 (p < 0.001). Bland-Altman plots showed a high degree of agreement between the HNT-1P measurements and those of the other devices.
Conclusions
The new non-contact HNT-1P tonometer provided reliable IOP, CCT, and cIOP measurements when compared with GAT and USP. HNT-1P could therefore be used clinically for reliable and accurate measurements of the IOP, CCT, and cIOP.
안압 측정은 안과 환자에서 수행되는 기본 검사 중 하나로 녹내장의 선별, 진단 및 치료에 중요하다[1]. Goldmann과 Schmidt이 개발한 골드만압평안압계는 안압 측정의 가장 표준이 되는 검사로 널리 사용되고 있다[2,3]. 골드만압평안압계의 정확도는 각막두께, 각막곡률 그리고 단단함, 점도, 탄성, 수화와 같은 생체공학적 특성에 영향을 받는다[4-8]. 그러나 이러한 생체공학적 특성은 개개인마다의 변동성이 있으며 각막의 병리학적 특성과 수술 여부에 영향을 받는다[5,7,9-11]. 골드만압평안압계는 눈물층의 염색과 함께 각막의 마취가 필요하고 각막과의 접촉이 필요한 침습적인 검사이다. 또한, 세극등현미경을 이용해야 하기 때문에 안과 검사실에서만 측정 가능하다는 단점이 있다[5,12,13]. 이러한 골드만압평안압계의 단점을 극복하기 위해 비접촉안압계, 리바운드안압계, 토노펜과 같은 다양한 대체 안압계들이 개발되었다.
새로운 안압계 HNT-1P는 비접촉식 안압계이다. 환자의 안압에 따라 공기 분사의 강도를 자동조절하여 개별 맞춤 안압 측정이 가능하고, 안압 신호를 획득한 순간에 정확히 공기압의 발생을 멈추어 환자의 불편감과 불쾌감을 최소화한다. 이와 더불어 샤임플러그(Scheimpflug) 원리의 촬영 방식을 이용한 각막두께 측정이 가능하며, 이 측정값에 따라 교정된 안압값을 제공한다. 그 외에도 전방각 단면촬영이 가능하고, 이러한 기능들을 이용하여 녹내장에 관한 진단에 도움이 될 수 있을 것으로 기대된다.
이에 저자들은 본 연구를 통해 새로운 비접촉안압계 HNT-1P로 측정한 안압, 중심각막두께, 교정된 안압값을 골드만압평안압계로 측정한 안압, 초음파 각막두께측정계로 측정한 중심각막두께, 그리고 이 둘을 이용한 교정된 안압값과 비교하여 HNT-1P 안압계의 신뢰도 및 임상적 유용성을 평가하고자 하였다.
대상과 방법
2017년 9월 서울아산병원을 방문한 정상안 또는 녹내장 의증 환자를 대상으로 한 전향적 연구를 시행하였으며, 3.5디옵터 이상의 각막 난시가 있거나 각막혼탁, 안내염증, 외상의 병력, 이전 굴절교정수술 병력, 최근 2주 이내 콘택트렌즈를 착용한 환자, 국소마취제 및 형광색소 성분에 과민증이 있는 경우, 임부 또는 수유부를 제외한 환자 60명(남자 29명, 여자 31명)을 대상으로 하였다. 본 연구는 헬싱키선언을 준수하였으며 본원의 임상시험심사위원회(Institutional Review Board, IRB)의 심사 및 승인을 받았다(승인 번호: 2017-0865).
대상안 120안에 대해 안압 및 중심각막두께를 숙련된 두 검사자가 측정하였다. 모든 대상군에게 서면 동의를 획득하였으며 인구학적 정보, 병력 조사, 임신반응검사 등 기초 정보를 확인하고, 시진, 시력검사, 굴절검사, 세극등검사를 시행하였다. 이후 두 검사자 중 한 명이 비접촉안압계(HNT-1P, Huvitz Co., Anyang, Korea)로 안압 및 중심각막두께를 측정하였고, 그 다음 점안 마취를 하고 골드만압평안압계(AT 900®, Haag-Streit, Bern, Switzerland)로 안압을 측정하였으며, 마지막으로 초음파 각막두께측정계(SP-3000®, Tomey, Nagoya, Japan)로 중심각막두께를 측정하였다. 각 측정계 사이에 적어도 5분의 시간 간격을 두었으며 측정 평균값을 유효성 평가를 위한 결과값으로 사용했다.
비접촉안압계 HNT-1P로 대상안의 안압 및 중심각막두께를 3회 반복 측정하였다. 안압, 중심각막두께, 및 교정된 안압값이 제공되었으며 평균값을 기록하였다. 환자가 눈을 감아 검사가 되지 않거나 기계상 오류가 표시된 경우는 제외하였다. 골드만압평안압계는 측정 전 0.5% 염산프로파카인과 형광물질이 혼합된 용액을 대상안에 점안한 후 안압을 3회씩 반복 측정하였다. 각 측정마다 최소 1분의 시간 간격을 두었으며 3회 측정 평균치를 분석에 사용했다. 초음파 각막두께측정계를 이용한 중심각막두께 측정은 골드만압평안압계 측정 이후 마지막으로 시행되었으며 측정 전 대상안에 0.5% 염산프로파카인 마취제를 점안하였다. 측정하는 동안 환자는 일정한 거리에 있는 지점을 보도록 하였으며 초음파 탐침이 각막 표면에 직각을 이루도록 하여 각막의 중심에 약하게 압평되었다. HNT-1P에서 자동 제공되는 중심각막두께가 교정된 안압은 (central corneal thickness [CCT] average – Pachy data) × C ratio가 이용되었으며 Pachy data는 HNT-1P로 측정한 중심각막두께이며 CCT average와 C ratio는 사용자가 조정할 수 있다. 본 연구에서는 기본적으로 설정되어 있는 CCT average 550 µm와 C ratio 0.05가 사용되었다[14,15]. 골드만압평안압계의 교정된 안압은 공식([골드만압평안압계로 측정한 안압]-0.012 × [초음파 각막두께측정계로 측정한 중심각막두께]-520)을 이용하여 산출하였다[16].
환자의 개인 특징과 측정치의 통계 결과는 연속형 자료는 평균 ± 표준편차로, 범주형 자료는 빈도로 표기하였다. 실험기기 HNT-1P와 대조기기로 측정한 안압, 중심각막두께 그리고 교정된 안압을 paired t-test로 비교하였고 Pearson 상관분석을 하였다. HNT-1P의 3회 측정치에 대한 재현성을 알아보기 위해 급내상관계수(intraclass correlation coefficient)를 분석하였으며 Bland-Altman plot을 사용하여 시험기기 및 대조기기 측정치 간의 차이의 평균과 일치도를 확인하였다. SPSS version 21.0 (IBM Corp., Armonk, NY, USA)를 이용하여 유의수준은 0.05 미만인 경우 통계학적으로 유의한 것으로 판단했다.
결 과
전 대상자들의 평균 나이는 61.2 ± 11.8세(20-79세)였고, 남자 29명(58안), 여자 31명(62안)이었다. 평균 구면렌즈대응치는 -0.84 ± 2.42D였으며 평균 각막난시는 0.88 ± 0.71D였다. 평균 비접촉안압계 HNT-1P로 측정한 안압(HNT-1P 안압)은 평균 14.9 ± 5.1 mmHg, 골드만압평안압계로 측정한 안압(골드만안압)은 평균 15.6 ± 5.2 mmHg, HNT-1P로 측정한 중심각막두께(HNT-1P 중심각막두께)는 평균 553.5 ± 27.4 µm, 초음파 각막두께측정계로 측정한 중심각막두께(초음파 중심각막두께)는 평균 550.6 ± 26.3 µm, HNT-1P로 측정한 교정안압(HNT-1P 교정안압)은 평균 14.7 ± 4.7 mmHg, 골드만안압과 초음파 중심각막두께로 산출한 교정안압(골드만 교정안압)은 평균 14.9 ± 4.8 mmHg였다. HNT-1P와 각 대조기기의 측정치를 paired t-test로 비교하였을 때 안압(p=0.054), 중심각막두께(p=0.050) 및 교정안압(p=0.068)은 모두 유의한 차이를 보이지 않았다(Table 1).
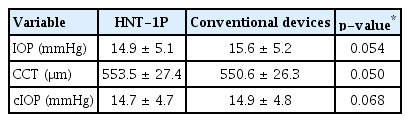
Mean and paired t-test comparison of IOP, CCT, and cIOP measured with HNT-1P and conventional devices
HNT-1P와 각 대조기기 간에는 뚜렷한 상관관계를 보였다(Fig. 1). HNT-1P 안압과 골드만안압(r=0.964, p<0.001), HNT-1P 중심각막두께와 초음파 중심각막두께(r=0.913, p<0.001), 그리고 HNT-1P 교정안압과 골드만안압(r=0.971, p<0.001)은 모두 유의한 상관 관계를 보였다(Table 2).

Correlation between HNT-1P and conventional devices. Correlation between (A) HNT-1P and Goldmann applanation tonometer intraocular pressure (IOP) measurements (r = 0.964, p < 0.001), (B) HNT-1P and ultrasound pachymetry central corneal thickness (CCT) measurements (r = 0.913, p < 0.001), and (C) HNT-1P and Goldmann applanation tonometer corrected intraocular pressure (cIOP) measurements (r = 0.913, p < 0.001). GAT = Goldmann applanation tonometry; USP = ultrasound pachymetry; R = Pearson correlation coefficient.

Bland-Altman analysis of IOP, CCT, and cIOP measurements by HNT-1P
골드만안압과 HNT-1P 안압을 기준으로 두 안압군(<15 mmHg과 ≥15 mmHg)으로 나누어 하위분석을 시행하였다(Table 3). 골드만압평안압계와 HNT-1P를 비교한 paired t-test는 골드만안압 기준(<15 mmHg, p=0.256; ≥15 mmHg, p=0.090)과 HNT-1P 안압 기준(<15 mmHg, p=0.092; ≥15 mmHg, p=0.354) 모두 유의한 차이를 보이지 않았으며 상관분석에서는 골드만안압 기준(<15 mmHg, r=0.801, p<0.001; ≥15 mmHg, r=0.941, p<0.001)과 교정된 안압 기준(<15 mmHg, r=0.808, p<0.001; ≥15 mmHg, r=0.941, p<0.001) 모두 유의한 상관관계를 보였다.
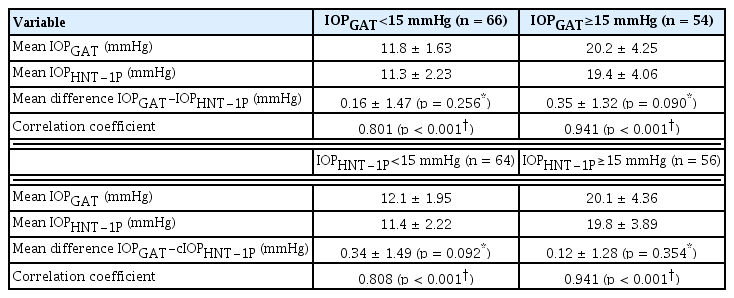
Subgroup analysis according to IOP measured with GAT and HNT-1P
급내상관계수는 HNT-1P로 3회씩 측정하였을 때 안압 0.995 (95% 신뢰구간 0.979-0.989), 중심각막두께 0.985 (95% 신뢰구간 0.979-0.989), 교정안압 0.994 (95% 신뢰구간 0.992-0.996)이었다. HNT-1P의 측정치 모두 우수한 재현성을 보였다(Table 4).
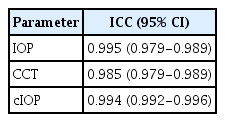
ICC of different parameters obtained by HNT-1P
HNT-1P로 측정한 안압, 중심각막두께, 그리고 교정된 안압을 각각의 대조 측정치와 비교하는 Bland-Altman plot에서는 골드만안압과 HNT-1P 안압 차이의 평균값은 0.25 ± 1.40 mmHg, 초음파 중심각막두께와 HNT-1P 중심각막 두께의 차이의 평균값은 -2.31 ± 11.31 µm, 골드만 교정안압과 HNT-1P 교정안압 차이의 평균값은 0.24 ± 1.16 mmHg였다(Table 2). HNT-1P의 95% limits of agreement 폭은 각 대조기기와 비교하여 안압 5.48 mmHg (-2.49 to 2.99), 중심각막두께 44.34 µm (-24.48 to 19.86), 그리고 교정안압 4.55 mmHg (-2.03 to 2.51)였다(Fig. 2). HNT-1P 측정값과 각 대조기기 간의 차이가 95% limits of agreement 폭에서 벗어난 경우는 안압은 6안(5%), 중심각막두께는 4안(3.33%), 교정안압 3안(2.5%)이었다.
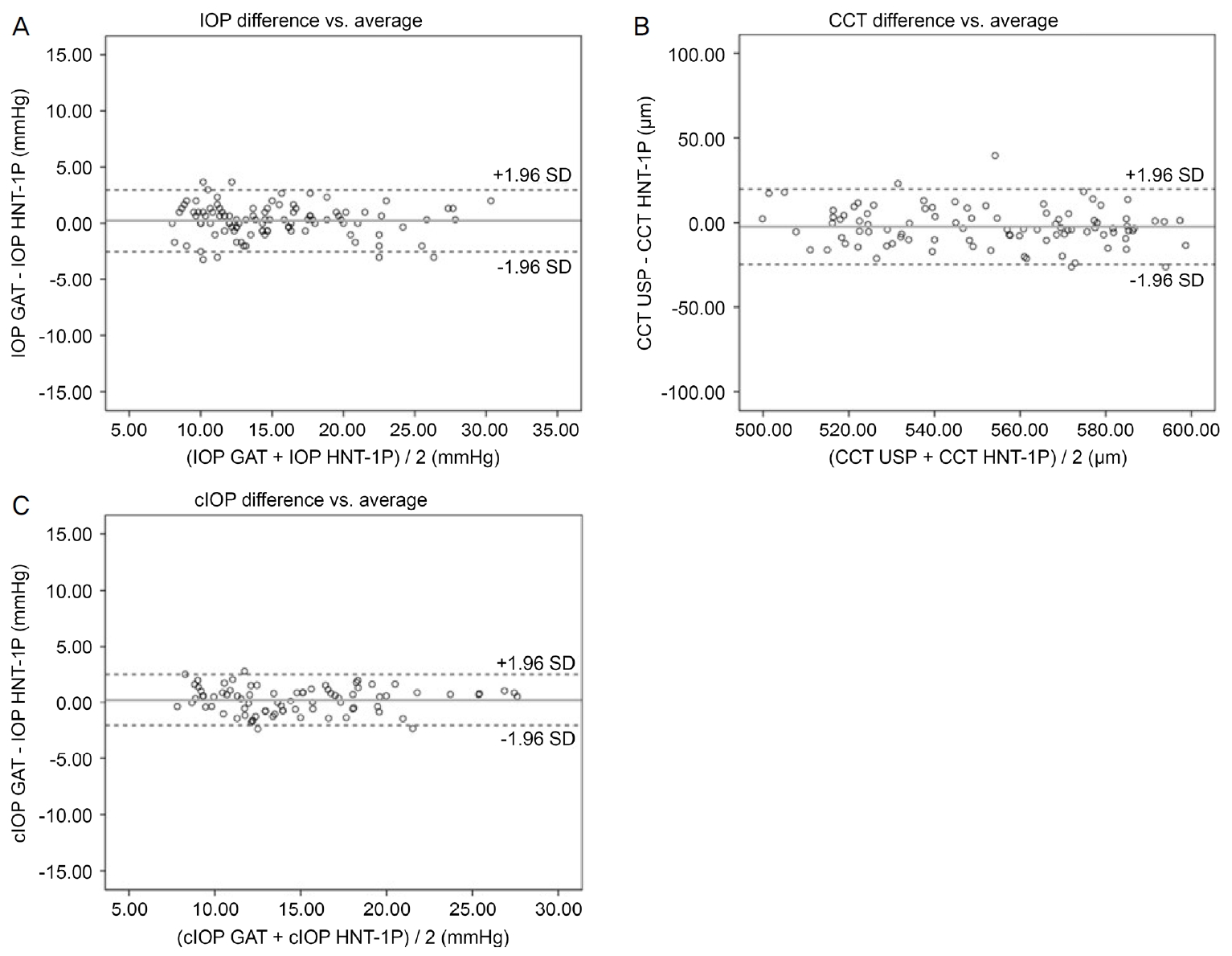
Bland-Altman plots between HNT-1P and conventional devices. Bland-Altman plots of the agreement between (A) intraocular pressure (IOP) measurements of HNT-1P and Goldmann applanation tonometer, (B) central corneal thickness (CCT) measurements of HNT-1P and ultrasound pachymetry, and (C) cIOP measurements of HNT-1P and Goldmann applanation tonometry (GAT). USP = ultrasound pachymetry; cIOP = corrected intraocular pressure; SD = standard deviation.
고 찰
정확한 안압 측정은 안과 환자의 중요한 기본적인 검사 중 하나로 특히 녹내장 환자나 고안압증 환자에서는 진단 및 치료의 효과 판단에 매우 중요하다[1]. 본 연구는 새로운 비접촉안압계 HNT-1P로 측정한 안압, 중심각막두께, 교정된 안압을 각각 대조기기인 골드만압평안압계로 측정한 안압, 초음파 각막두께측정계로 측정한 중심각막두께, 이 둘의 값을 이용하여 산출한 중심각막두께로 교정된 안압과 비교하여 신뢰도 평가 및 기기의 임상적 유용성에 대해 평가하고자 하였으며 HNT-1P는 각 대조기기와 비교하여 높은 상관도 및 일치도를 보였다.
골드만압평안압계는 안압 측정에 있어 가장 정확하며 널리 사용되고 있다[17,18]. 그러나 눈물층의 염색과 함께 각막의 마취가 필요하고 각막과의 접촉이 필요한 침습적인 검사이다. 또한, 세극등현미경을 이용해야 하기 때문에 안과 검사실에서만 측정 가능하다는 단점이 있다. 1972년 Grolman에 의해 소개된 비접촉안압계는 안과 진료에서 흔히 사용되는 안압계이다[19]. 이는 각막에 공기를 분사하고 각막의 압평을 광학적으로 측정하여 안압값을 산출한다. 비접촉안압계는 각막마취 및 눈물막의 염색이 필요하지 않아 감염 위험이 줄어든다는 장점이 있다[20]. HNT-1P는 비접촉안압계로서 각막마취 및 눈물막의 염색과 각막과의 접촉이 필요하지 않아 비침습적인 검사를 시행할 수 있으며, 빠른 검사 시간과 환자와 검사자 모두에게 편리한 검사 환경을 제공할 수 있을 것이다. HNT-1P로 측정한 안압과 골드만압평안압계로 측정한 안압을 비교하였을 때 유의한 상관성을 보였다(r=0.964, p<0.001). 골드만안압과 HNT-1P 안압 15 mmHg 기준으로 나누어 시행한 하위분석에서도 두 기기 간에 유의한 상관성을 보여줘 다양한 안압 범위에서의 HNT-1P에 대한 신뢰성을 확인할 수 있었다. 또한 두 기기 간의 Bland-Altman plot 분석에서 골드만안압과 HNT-1P 안압 차이의 평균은 0.25 mmHg로 적은 차이를 보였으며 95% limits of agreement 범위는 5.48 mmHg (-2.49 to 2.99)로 확인되었다. 이전 연구의 골드만압평안압계와 비접촉안압계의 Bland-Altman plot 비교에서 3에서 10 mmHg의 95% limits of agreement를 보여 본 연구 또한 이에 상응하는 높은 일치도를 보였다[21-24]. 안압 측정치에서 95% limits of agreement를 벗어나는 경우는 6안(5%)으로 대부분의 측정치가 95% limits of agreement 내로 측정되었으며 HNT-1P 안압과 골드만안압 간에 높은 일치도를 보였다. HNT-1P가 비침습적인 방법으로 신뢰성 있는 안압 정보를 제공하여 진단에 도움이 될 수 있을 것으로 사료된다.
중심각막두께는 골드만압평안압계와 비접촉안압계 모두에 중요한 변수로 작용한다[25,26]. 골드만압평안압계는 평균 중심각막두께 520 µm를 기준으로 교정되어 계산된 값으로이 기준으로부터 벗어나게 되면 정확성에 영향을 받게 된다[6,27]. 비접촉안압계는 더 넓은 각막 표면에 작용하여 중심각막두께 변화에 더 취약하다[22]. 따라서 정확한 안압을 평가하기 위해서 중심각막두께를 확인하는 것이 중요하다. 초음파 각막두께측정계는 표준 검사로 널리 사용되며 높은 재현성과 신뢰도를 보인다[28-30]. 그러나 검사자의 숙련도나 각막의 측정 부위에 따라 오차가 발생할 수 있다[31]. 또한 측정 전 점안마취가 필요하며 각막의 표면에 직접 접촉으로 인한 감염도 발생할 수 있는 침습적인 검사이다[32,33]. 검사하는 동안 환자가 일정하게 주시를 해야 하며 불편감을 초래할 수 있다. 이러한 단점들을 극복하고자 근래에는 측정 오차를 줄이기 위한 비접촉 방법으로 각막두께를 측정하는 검사 장비들이 다양하게 개발되고 있다[34]. HNT-1P는 샤임플러그 원리의 촬영 방식을 이용하여 각막두께 측정이 가능하다. 비접촉 각막두께측정계로서 비접촉성, 비침습적 방법으로 각막마취가 필요하지 않으며, 접촉으로 인해 발생할 수 있는 오차와 합병증을 줄일 수 있다. HNT-1P와 초음파 각막두께측정계의 중심각막두께 측정치는 높은 상관성을 보였다(r=0.913, p<0.001). 또한, Bland-Altman plot 분석에서 중심각막두께는 초음파 각막두께측정계와 HNT-1P 측정치 차이의 평균이 2.31 µm로 확인되었으며 44.34 (-24.48 to 19.86)의 95% limits of agreement 범위를 보였다. 이러한 차이는 측정치 범위 전체에 걸쳐 일정하게 나타났다. 이전 연구에서 초음파 각막두께측정계와 샤임플러그 방식을 이용한 각막두께측정계인 Pentacam®과 비교하였을 때 56.5에서 62.6 µm까지의 95% limits of agreement 범위의 결과를 보였으며 본 연구도 이에 상응하는 것을 확인하였다[35,36]. 본 연구에서는 4안(3.33%)에서 95% limits of agreement를 벗어나는 중심각막두께 측정치를 보였으나 대부분은 95% limits of agreement 내로 측정되어 HNT-1P 중심각막두께와 초음파 중심각막두께 간에 높은 일치도를 보였다. 중심각막두께 측정에서도 HNT-1P가 비접촉의 안전적인 방법으로 신뢰성 있는 정보를 제공할 수 있을 것이다.
골드만압평안압계와 비접촉안압계로 측정한 안압 모두 중심각막두께에 영향을 받기 때문에 정확한 안압 평가를 위해서 중심각막두께 정보가 중요하며 이를 교정한 안압이 녹내장의 진료와 진단에 도움이 될 수 있다. Suzuki et al [16]은 중심각막두께를 이용한 교정된 안압을 계산할 수 있는 공식을 제시하였다. 이와 달리 HNT-1P는 중심각막두께 측정과 함께 이를 이용한 교정된 안압 정보를 자동 제공하여 편리성과 더불어 보다 정확한 안압 정보를 제공할 수 있다. HNT-1P에서 제공한 교정안압과 골드만 교정안압은 유의한 상관관계를 보였다(r=0.971, p<0.001). 이전 연구에서 중심각막두께가 교정된 안압을 자동 제공하는 비접촉안압계인 CT-1P와 골드만 교정안압을 비교하였을 때 유의한 상관관계를 보였으며(r=0.712, p<0.001), 본 연구의 결과가 이와 상응하는 것을 확인할 수 있었다[37]. Bland-Altman plot 분석에서 중심각막두께를 교정한 골드만 교정안압과 HNT-1P 교정안압 측정치 차이의 평균은 0.24 mmHg였으며 95% limits of agreement 범위는 4.55 mmHg (-2.03 to 2.51)였다. 이를 벗어나는 경우는 3안(2.5%)에서 확인되었으며 대부분의 측정치가 95% limits of agreement 내로 측정되어 높은 일치도를 보여 신뢰성 있는 교정안압을 제공할 수 있을 것으로 보인다.
본 연구의 제한점은 3차 병원 내원객 중의 지원자를 대상으로 하여 전체 대상자의 평균 나이가 61.2세의 높은 연령대로 지정된 표본 집단이 전체 인구를 대변하지 못한다는 점이 있다. 추후 더 다양한 연령대의 환자를 대상으로한 연령별 분석이 필요할 것이다. 대상자들은 골드만 안압 측정 후 초음파 중심각막두께를 측정하였는데, 두 검사 다각막을 압평하는 검사로서 이로 인한 이력현상으로 초음파 중심각막두께 결과에 영향을 줬을 가능성이 있으며, 검사 순서를 바꿔 측정치 못한 제한점이 있다. 본 연구에서 골드만압평안압계로 측정한 안압과 교정된 안압을 기준으로 저안압군과 고안압군에서의 하위분석을 시행하였으나 연구 대상자가 정상안 또는 녹내장 의증 환자들로서 저안압(안압≤10mmHg) 및 고안압(안압≥21 mmHg)의 환자 수가 많지 않아 다양한 안압 범위에서의 신뢰성을 확인하기에는 제한이 있다. 추후 넓은 안압 범위의 환자를 대상으로 다양한 안압 범위에서의 추가 분석이 필요할 것이다. 또한 3.5디옵터 이상의 각막 난시가 있는 환자들은 본 연구에서 제외가 되어 원추각막, 각막부종, 각막궤양, 각막혼탁 등의 각막 표면이 일정하지 않거나 각막 난시가 높은 환자들을 대상으로 검사의 정확성을 알 수 없다. 향후 각막 난시가 높은 환자들을 대상으로 하여 난시에 따른 결과를 확인해야 할 것이다. 또한 본 연구에서는 중심각막두께에 따른 비교분석을 시행하지 않았다. 중심각막두께에 의한 HNT-1P 안압값의 영향을 확인하기 위해 향후 중심각막별두께별로 대조기기와의 비교 하위분석이 필요하다.
결론적으로 새로운 비접촉안압계 HNT-1P는 비침습적, 비접촉식으로 안압과 각막두께가 측정 가능한 기기로 환자와 검사자에게 편의와 안정성을 제공할 수 있다. 각 대조기기와 비교하여 HNT-1P 안압, 중심각막두께, 교정안압은 우수한 일치도를 보여 신뢰도 높은 안압 정보를 제공할 수 있을 것이다. 따라서 일반검진 또는 집단검진 시에 정확한 안압 측정으로 녹내장의 진단과 치료 및 경과 관찰에 도움이 될 것으로 보인다.
Notes
Conflict of Interest
The authors have no conflicts to disclose.
References
Biography
어규상 / Kyu Sang Eah
울산대학교 의과대학 서울아산병원 안과학교실
Department of Ophthalmology, Asan Medical Center, University of Ulsan College of Medicine
