한국인에서 홍채각막내피증후군의 임상 양상
Clinical Features of Iridocorneal Endothelial Syndrome in Korean Patients
Article information
Abstract
목적
국내 단일기관에 내원한 홍채각막내피증후군 환자의 질환별 분포와 임상 양상을 보고하고자 한다.
대상과 방법
1993년부터 2023년까지 영남대학교병원 안과에 내원하여 홍채각막내피증후군으로 진단받은 환자들의 의무기록을 후향적으로 분석하였다. 각막과 홍채 이상 정도에 따라 Chandler 증후군, 진행성 홍채위축, 홍채모반증후군으로 구분하였으며 진단 당시 녹내장, 각막부종 및 홍채 이상 유무 등을 조사하였다.
결과
총 21명 환자의 홍채각막내피증후군 22안이 분석에 포함되었다. 진단 시 환자들의 평균 연령은 56.6 ± 16.1세였고 대부분 여성(20명, 95.5%)이었으며, 단안(20명, 95.5%)에 발생하였다. 질환의 아형(subtype)은 Chandler 증후군이 9안(40.9%), 진행성 홍채위축이 7안(31.8%), 홍채모반증후군이 6안(27.3%)으로 분포하였다. 15안(68.2%)에서 녹내장이 관찰되었고, 8안(36.4%)에서 녹내장수술을 시행받았다. 첫 녹내장수술로 섬유주절제술을 시행받은 7안 중 6안에서 안압 조절이 불량하였으며 이 중 4안에서 Ahmed valve 삽입술을 시행받았다. 10안(45.5%)에서 초진 시 각막부종을 보였으며 6안(27.3%)에서 각막 기능부전으로 진행하였다.
결론
국내 홍채각막내피증후군 대부분이 중년 여성에게 단안으로 발생하였고, Chandler 증후군이 가장 많았다. 높은 녹내장의 빈도, 불량한 섬유주절제술의 경과 및 높은 각막 기능부전의 진행 위험성으로 인해 지속적인 녹내장 관리와 각막 기능 보존을 위한 노력이 필요할 것으로 생각된다.
Trans Abstract
Purpose
To document the distribution and clinical features of iridocorneal endothelial (ICE) syndrome in its various subtypes observed in patients who visited a single institution in Korea.
Methods
A retrospective analysis was conducted on the medical records of patients diagnosed with ICE syndrome at the Department of Ophthalmology, Yeungnam University Hospital, from 1993 to 2023. The cases were classified into Chandler syndrome, progressive iris atrophy, and iris nevus syndrome based on the severity of corneal and iris abnormalities. We also examined the presence of glaucoma, corneal edema, and iris abnormalities at diagnosis.
Results
In all, 22 eyes from 21 patients with ICE syndrome were included. The mean age at diagnosis was 56.6 ± 16.1 years with a female predominance (20 patients, 95.5%). The syndrome was primarily unilateral (20 patients, 95.5%). Subtypes included 9 eyes with Chandler syndrome (40.9%), 7 eyes with progressive iris atrophy (31.8%), and 6 eyes with iris nevus syndrome (27.3%). Glaucoma was present in 15 eyes (68.2%), with 8 eyes (36.4%) undergoing glaucoma surgery. Of the 7 eyes that had trabeculectomy as initial glaucoma surgery, six experienced poor intraocular pressure control leading to Ahmed valve implantation in 4 cases. Corneal edema was noted in 10 eyes (45.5%) at diagnosis progressing to corneal decompensation in 6 eyes (27.3%).
Conclusions
ICE syndrome in Korea predominantly affects middle-aged women and occurs unilaterally with Chandler syndrome being the most common subtype. Given the high risk for glaucoma development, suboptimal outcomes of trabeculectomy, and significant risk for corneal decompensation, ongoing management efforts are essential for glaucoma and corneal function preservation.
홍채각막내피증후군(iridocorneal endothelial syndrome, ICE syndrome)은 각막부종, 홍채의 변화, 이차 폐쇄각녹내장 등의 특징을 보이는 질환이다. 1979년 Yanoff에 의해 유사한 특징을 가지는 세 질환인 Chandler 증후군(Chandler syndrome), 진행성 홍채위축(progressive iris atrophy) 그리고 홍채모반증후군(iris nevus syndrome, Cogan Reese syndrome)을 총칭하여 홍채각막내피증후군으로 처음 명명되었다.1
비정상적인 각막내피세포가 전방각 및 홍채로 증식하게 되고, 이렇게 발생한 막이 수축을 하며 이차 폐쇄각녹내장 및 홍채의 변형을 유발하는 것이 홍채각막내피증후군의 발병 기전으로 알려져 있다.2,3 주로 중년의 여성에게 단안으로 발생하며 발병 원인으로 herpes simplex virus가 연관이 있다고 제시되고 있다.4 세극등현미경검사상 hammered-silver 모양의 각막내피세포층 변화를 보이며5 경면현미경검사상 정상 각막내피세포와 명암 반전을 보이는 특징적 ICE 세포를 관찰할 수 있다.6,7
Chandler 증후군에서는 각막부종이 특징적이며 홍채는 정상 또는 경도의 이상을 보인다. 진행성 홍채위축의 경우 홍채 이상이 특징적으로 심한 홍채위축 및 홍채 구멍(iris hole) 등을 관찰할 수 있다.8,9 각막 및 홍채 이상의 정도와 상관없이 홍채의 결절(iris nodule)을 동반하는 경우 홍채모반증후군으로 진단할 수 있다.10
홍채각막내피증후군을 대상으로 미국에서 백인 82안,11 태국에서 태국인 60안,12 인도에서 인도인 203안13을 각각 분석하여 질환별 분포 및 임상 양상이 보고된 바 있다. 하지만 아직까지 국내에서는 홍채각막내피증후군의 양상이 증례 위주로 보고되었고,14,15 다수의 환자들을 대상으로 아형의 분포와 임상 특징을 분석한 연구는 없었다.
이에 본 연구에서는 영남대학교병원 안과에 내원하여 홍채각막내피증후군으로 진단받은 환자들을 대상으로 질환의 아형 분포와 임상 양상을 분석하고 기존 보고된 해외 연구와 비교하여 한국 홍채각막내피증후군 환자들의 임상 특징을 알아보고자 하였다.
대상과 방법
1993년 4월부터 2023년 2월까지 영남대학교병원 안과에 내원하여 홍채각막내피증후군으로 진단받은 모든 환자의 의무기록을 후향적으로 분석하였다. 포도막염, 안외상 등 홍채 병변에 영향을 줄 수 있는 질환의 병력이 있는 환자는 연구에서 제외되었다. 본 연구는 헬싱키선언(Declaration of Helsinki)을 준수하였으며 영남대학교병원 임상연구윤리위원회(Institutional Review Board, IRB)의 승인을 얻었다(승인번호: 2023-07-025).
홍채각막내피증후군은 전형적 형태의 각막내피세포층 변화 또는 각막부종을 보이며 특징적인 홍채 이상 및 주변 홍채앞유착이 동반된 경우에 진단되었다. 정상 또는 경도의 홍채 이상을 가진 대상자는 Chandler 증후군으로 분류하였고, 심한 홍채위축과 홍채 구멍, 동공 편위를 동시에 보이는 대상자는 진행성 홍채위축으로, 홍채의 색소 결절을 가진 대상자는 홍채모반증후군으로 세부 분류하였다.
대상자들의 병력, 시력, 골드만압평안압, 세극등현미경검사 결과 및 전안부 사진, 앞방각경검사, Humphrey 자동시야검사(Carl Zeiss Meditec, Dublin, CA, USA), 망막신경섬유층 및 시신경유두 사진, 경면현미경검사를 분석하였다.
각막부종은 임상적으로 세극등현미경검사상 각막실질 혹은 상피의 부종이 관찰되고 시력저하가 동반된 경우로 정의하였다. 주변홍채앞유착(peripheral anterior synechiae, PAS)은 앞방각경검사에 따라 absent (30° 미만), mild (30° 이상, 90° 미만), moderate (90° 이상, 180° 이하), severe (180° 초과, 270° 이하), extensive (270° 초과) PAS로 분류하였다. 녹내장은 안저검사상 전형적인 녹내장성 시신경유두 손상을 보이고, 녹내장 외에 시신경 손상을 일으킬 만한 원인 질환이 없으며 이에 상응하는 시야결손이 Humphrey 자동시야검사에서 반복적으로 관찰되는 경우로 정의하였다.
자료의 통계 분석은 IBM SPSS ver. 27.0 (IBM Corp., Armonk, NY, USA)을 사용하였다. 세 가지 아형 간 비교를 위해 범주형 변수는 Fisher’s exact test를 사용하였고 연속형 변수는 Kruskal Wallis test를 사용하였으며 p<0.05일 때 통계적인 유의성이 있다고 판단하였다. 통계적인 유의성이 있는 경우 각각의 아형 간의 다중 비교를 위해 Mann-Whitney U test 및 Bonferroni correction을 통한 사후검정을 시행하였고, p<0.017=0.05/3로 유의수준을 설정하였다. 연속형 변수의 수술 전후 비교를 위해서는 Wilcoxon signed rank test를 시행하였다.
결 과
홍채각막내피증후군으로 진단된 전체 21명 대상자의 22안이 포함되었으며 이 중 Chandler 증후군(Fig. 1)이 9안(40.9%), 진행성 홍채위축(Fig. 2)이 7안(31.8%), 홍채모반증후군(Fig. 3)이 6안(27.3%)으로 Chandler 증후군이 가장 많았다. 전체 환자의 평균 연령은 56.6 ± 16.1세(range, 31-87세)였다. 전체 환자 중 Chandler 증후군 남자 환자 1명(4.5%)을 제외하고 모두 여성(20명, 95.5%)이었다. 대부분 단안(20명, 95.5%)에 발생하였고, 진행성 홍채위축 환자 1명(4.5%)에서만 양안에서 관찰되었다. 환자들의 평균 경과 관찰 기간은 90.6 ± 90.1개월이었다. 초진 시 시력(logarithm of minimal angle of resolution)은 Chandler 증후군에서 0.05 ± 0.03, 진행성 홍채위축에서 0.40 ± 0.31, 홍채모반증후군에서 0.29 ± 0.25로, Chandler 증후군 환자에서 진행성 홍채위축 환자에 비해 유의미하게 좋았다(p=0.004, Bonferroni post-hoc test) (Table 1).

Corneal findings of the patient (female/45) with Chandler syndrome. (A) Slit-lamp photography shows a “Hammered-silver” appearance. (B) Specular microscopy shows the typical “ICE cell”, characterized by a light-dark reversal pattern. ICE = iridocorneal endothelial.

Representative cases of progressive iris atrophy show. (A) Female, 63 years old - corectopia, stretch hole, and peripheral anterior synechiae, (B) female, 43 years old - corectopia, polycoria, and ectropion uvea.

Representative cases of Cogan Reese syndrome showing iris nodules and ectropion uvea. (A) Female, 31 years old, (B) female, 53 years old.

Demographic and clinical characteristics of the patients
전체 22안 중 10안(45.5%)에서 초진 시 각막부종이 관찰되었다. 그룹별로는 Chandler 증후군의 55.6%, 진행성 홍채 위축의 28.6%, 홍채모반증후군의 50%에서 초진 시 각막부종을 보였다. 경면현미경검사상 각막내피세포밀도의 중위수는 Chandler 증후군에서 2,120/mm2, 진행성 홍채위축에서 1,508/mm2, 홍채모반증후군에서 1,773/mm2로 측정되었고 그룹 간의 유의한 차이는 없었다(Table 2).

Characteristics associated with glaucoma, corneal abnormalities and iris abnormalities
주변홍채앞유착은 Chandler 증후군의 55.6%, 진행성 홍채위축 및 홍채모반증후군의 모든 환자에서 관찰되었다. 180° 초과의 심한 주변홍채앞유착의 경우 Chandler 증후군의 11.1%, 진행성 홍채위축의 28.6%, 홍채모반증후군의 83.3%에서 관찰되어 각 그룹 간 의미 있는 차이가 있었다(p=0.013) (Table 2).
홍채각막내피증후군으로 진단된 총 22안 중 11안(50%)에서 초진 시 녹내장이 동반되어 있었으며, 10안(45.6%)에서 안압하강제(2.1 ± 0.7개)를 점안하고 있었다. 전체 환자의 초진 시 안압은 평균 22.1 ± 11.4 mmHg, 안압하강제를 점안하지 않던 환자들의 안압은 평균 17.8 ± 7.1 mmHg, 안압하강제를 점안하던 환자들의 안압은 평균 27.2 ± 12.7 mmHg였다. 초진 시 녹내장 동반 여부 및 안압은 홍채각막내피증후군의 세 그룹 간 서로 유의한 차이를 보이지 않았다. 초진 시 녹내장이 없었던 4안(18.2%)에서 경과 관찰 도중 녹내장이 발생하였으며 녹내장 발생 시까지 기간은 평균 74.5개월이었다(Table 2).
8안(36.4%)에서 초진으로부터 평균 12.5개월 후 첫 녹내장수술을 시행받았다. 녹내장수술 시행 여부 또한 각 그룹 간 의미 있는 차이를 보이지 않았다. Chandler 증후군 9안 중 3안(33.3%)에서 섬유주절제술을 시행받았으며 이 중 2안에서 섬유주절제술 이후 추가로 Ahmed valve 삽입술을 시행받았다. 진행성 홍채위축 7안 중 2안(28.6%)에서 첫 녹내장수술로 섬유주절제술 및 Ahmed valve 삽입술을 각각 시행받았다. 홍채모반증후군 6안 중 3안(50%)에서 섬유주절제술을 시행받았으며 이 중 2안(33.3%)에서 Ahmed valve 삽입술을 추가로 시행받았다. Ahmed valve 삽입술을 시행받은 5안 모두 술 후 안압이 21 mmHg 이하로 조절되었으나 이 중 4안(80%)에서 각막 기능부전으로 진행하였다. 경면현미경검사상 평균 각막내피세포밀도는 Ahmed valve 삽입술 시행 전(1,686개/mm2)에 비해 시행 후(778개/mm2) 통계적으로 유의하게 감소하였다(p=0.043).
동공 편위는 Chandler 증후군의 22.2%, 진행성 홍채위축 및 홍채모반증후군의 모든 환자에서 관찰되었다. Chandler 증후군 환자에서는 홍채 구멍 및 포도막외반이 보이지 않았으나 진행성 홍채위축 환자의 42.9%, 홍채모반증후군 환자의 16.7%에서 홍채 구멍을 보였으며, 진행성 홍채위축 환자의 14.3%, 홍채모반증후군 환자의 66.7%에서 포도막 외반을 볼 수 있었다(Fig. 2, 3, Table 3).
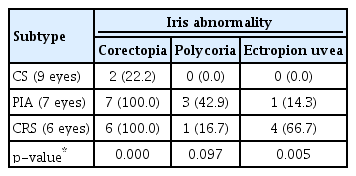
Iris abnormalities according to the subtype of ICE syndrome
고 찰
홍채각막내피증후군은 주로 중년의 여성에서 단안을 침범하는 후천성 각막 질환으로 비정상적인 각막내피세포의 증식으로 인해 각막부종 및 이차 폐쇄각녹내장을 동반하는 질환이다.9 본 연구에서는 국내 홍채각막내피증후군 환자들의 임상 양상과 경과를 분석하였고, 다른 인종들을 대상으로 한 기존 보고들과 비교하였다(Table 4).
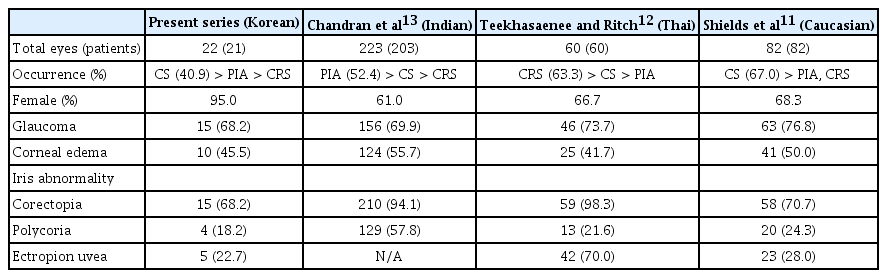
Comparison of clinical features of ICE syndrome between the present study and previous studies
이전 인도인,13 태국인,12 백인11들을 대상으로 한 이전 연구들에서 홍채각막내피증후군 환자 중 여성이 차지하는 비율은 각각 61.0%, 66.7%, 68.3%였고, 한국인을 대상으로 한 본 연구에서는 95.0%로 기존 연구보다 높은 여성 비율을 보였다. 본 연구에서 환자들의 평균 연령은 56.6세로 기존 연구들(41.5-43.7세)11-13에 비해 다소 높게 나타났다. 이는 홍채각막내피증후군의 발병에 관여하는 소인에 인종별 차이가 있을 수 있음을 시사하였다.
홍채각막내피증후군 각 아형의 빈도에 대해서도 인종 간 차이를 보였다. 본 연구와 미국 백인을 대상으로 한 연구11에서는 Chandler 증후군의 빈도가 각각 40.9%, 67.0%로 가장 높았다. 반면에, 태국인을 대상으로 한 연구12에서는 홍채모반증후군이 63.3%로 가장 많았으며, 인도인을 대상으로 한 연구13에서는 진행성 홍채위축이 52.4%로 가장 많았다. 이는 홍채각막내피증후군의 병인과 관련하여 이상 증식하는 각막내피세포의 각막 및 홍채 침범 정도와 연관된 특징들이 인종별 차이가 있을 수 있음을 시사한다. 특히, 홍채각막내피증후군 환자의 방수 및 각막내피에서 herpes simplex virus가 검출되어 병인과 연관될 것으로 생각되고 있는데16 유전적, 환경적 요인 및 면역체계의 차이 등에 의해 인종별로 virus의 영향이 다르게 나타날 수 있어, 추후 이에 대한 연구가 필요할 것으로 생각된다. 또한 Chandler 증후군의 경우, 임상 양상이 비교적 경한 경우 진단에서 빠질 가능성이 있어, 아형의 빈도에 영향을 줄 수 있을 것으로 생각된다.
본 연구에서 초진 시부터 녹내장이 있었던 환자의 빈도는 50.0%로, 기존 연구들(69.9-76.8%)11-13에 비해 낮은 경향을 보였다. 하지만 본 연구에서도 마지막 경과 관찰 시에는 녹내장의 빈도가 68.2%로 확인되어 기존 연구들과 유사한 높은 녹내장의 이환율을 보였다. 즉, 홍채각막내피증후군 환자의 안압과 녹내장 발생 여부를 지속적으로 확인하는 것이 반드시 필요하다.
국내의 홍채각막내피증후군 환자를 대상으로 섬유주절제술과 Ahmed valve 삽입술 후의 치료 성적을 비교한 연구17에서 술 전과 비교한 술 후 12개월째의 안압은 섬유주절제술보다 Ahmed valve 삽입술에서 더 낮게 유지되었지만, 각막내피세포밀도의 감소는 섬유주절제술보다 Ahmed valve 삽입술에서 더 뚜렷하였다. 본 연구에서 녹내장수술을 받은 8안(36.4%) 중 7안은 첫 녹내장수술로 섬유주절제술을 시행받았으며 1안은 Ahmed valve 삽입술을 시행받았다. 섬유주절제술을 시행받은 7안 중 6안에서 추후 안압이 조절되지 않았으며 이 중 4안에서 Ahmed valve 삽입술을 추가로 시행받았다. Ahmed valve 삽입술을 시행받은 5안 모두 술 후 안압이 조절되었으나 이 중 4안이 각막 기능부전으로 진행하였다. 즉, 안압이 조절되지 않는 홍채각막내피증후군의 경우 섬유주절제술의 예후가 불량하고, Ahmed valve 삽입술 역시 안압하강에도 불구하고 각막 기능부전의 위험성을 높일 수 있다는 제한점이 있음을 본 연구에서도 확인할 수 있었다.
홍채각막내피증후군에서 각막부종은 비정상적인 각막내피세포의 각막 침범 정도 및 안압상승에 의한 이차적인 변화와 연관될 수 있다.18 각막부종을 보이는 경우 우선 점안 안압하강제를 통한 안압 조절이 필요하며, 고삼투압제 안약을 점안하는 것 또한 도움이 된다고 알려져 있다.19 본 연구에서 초진 시 각막부종을 보인 환자의 비율은 45.5%로, 기존 연구들의 결과(41.7-55.7%)11-13와 비슷하였고, 기존 연구들과 마찬가지로 Chandler 증후군 환자에서 각막부종의 비율이 가장 높았다.
태국인을 대상으로 한 연구12에서 각막내피세포밀도가 감소하며 각막 기능부전으로 진행된 빈도가 13.3%로 보고되었다. 본 연구에서는 6명(27.3%)에서 초진 시 심하지 않은 각막부종을 보였으나 경과 관찰 도중 각막 기능부전으로 진행하였다(Fig. 4). 이 중 대부분(5명)은 녹내장수술 후 안압이 조절되었음에도 불구하고 각막 기능부전으로 진행되어 안압과 무관하게 각막 기능이 악화되는 경우가 더 많았고, 이러한 경우 각막이식이 필요하였다.

Slit-lamp photography of iridocorneal endothelial syndrome after Ahmed valve implantation. (A) Female, 45 years old - eye with Chandler syndrome shows mild corneal edema. (B) Female, 58 years old - eye with Cogan-Reese syndrome shows corneal decompensation.
홍채 이상은 동공 편위, 홍채 구멍, 포도막외반 등 다양하게 나타나고, 본 연구에서 이들의 빈도는 각각 68.2%, 18.2%, 22.7%로 미국 백인들을 대상으로 한 연구 결과11와 비슷하였다. 진행성 홍채위축과 홍채모반증후군의 빈도가 높은 인도인13과 태국인을 대상으로 한 연구12들에서 더 심한 홍채의 변형 소견인 홍채 구멍 및 포도막외반의 빈도가 상대적으로 더 높았다. 이는 홍채 이상을 분류하는 기준에 따라, 혹은 홍채각막내피증후군의 3가지 분류 중 어떤 질환이 더 많이 분포하였는지에 따라 보고마다 차이가 날 수 있을 것으로 생각된다.
본 연구는 여러 제한점이 있다. 첫째, 전안부 사진이 누락되어 있는 경우가 있었다는 점이다. 하지만 전안부 사진이 없는 경우, 의무기록에 특징적인 홍채의 형태가 그려져 있고 세극등현미경 소견이 구체적으로 기술되어 있어 홍채각막내피증후군의 아형을 분류하는 데 있어 오류를 최소화할 수 있었다. 또한, 진단에 필수적인 경면현미경검사 결과, 안압의 기록 등은 모두 존재하였다. 둘째, 3차 의료기관을 방문한 환자를 대상으로 연구가 이루어졌기 때문에 안압이 조절되지 않는 등 다소 중한 환자가 많이 포함되는 선택 편향(selection bias)을 배제하기 어렵다. 또한 녹내장이 동반되어 있지 않은 홍채각막내피증후군 환자의 경우 경면현미경검사를 시행하지 않았다면 진단을 받지 못하였을 수도 있다. 셋째, 비교적 드문 질환이기 때문에 연구에 포함된 환자들의 숫자가 많지 않아 통계 분석 결과에 영향을 줄 수 있고, 포함된 환자들의 경과 관찰 기간이 다양하여(90.6 ± 90.1개월) 경과에 영향을 주는 질환별, 임상적 특징을 분석하기 어려웠다. 추후 더 많은 환자들을 대상으로 오랜 기간 추적 관찰한 연구 결과가 필요할 것으로 보인다. 마지막으로, 본 연구는 단일기관에 내원한 환자들의 분석 결과로, 인종 간 비교를 위한 자료로는 제한이 있어, 추후 population-based study가 필요할 것으로 생각된다.
본 연구는 국내 단일기관에 내원한 홍채각막내피증후군 환자들을 대상으로 각 아형별 분포, 임상 양상, 경과 및 예후에 대한 최초 보고로서 의미가 있다. 요약하면, 국내에서 홍채각막내피증후군은 중년 여성에게 단안으로 주로 발생하였으며, Chandler 증후군이 가장 높은 빈도를 보였다. 녹내장의 빈도가 높고 섬유주절제술의 예후가 좋지 않으며 안압이 조절되더라도 각막 기능부전으로 진행되는 경우가 많아 녹내장 관리와 각막 기능 보존을 위한 지속적인 치료가 필요할 것으로 생각된다.
Notes
Conflicts of Interest
The authors have no conflicts to disclose.
References
Biography
박형준 / Hyeong Jun Park
Department of Ophthalmology, Yeungnam University College of Medicine