

Ļ░æņāüņāśļłłļ│æņ”Ø(thyroid eye disease)ņØĆ ņĢłņÖĆņŚÉ ņśüĒ¢źņØä ļ»Ėņ╣śļŖö Ļ░Ćņן ĒØöĒĢ£ ņ×ÉĻ░Ćļ®┤ņŚŁ ņ¦łĒÖś ņżæņŚÉ ĒĢśļéśļĪ£, Ļ░æņāüņäĀĻĖ░ļŖźĒĢŁņ¦äņ”ØĻ│╝ ņŻ╝ļĪ£ ņŚ░Ļ┤ĆļÉśņ¢┤ ļ░£ņāØĒĢśņ¦Ćļ¦ī ĒĢśņŗ£ļ¬©ĒåĀ Ļ░æņāüņäĀņŚ╝Ļ│╝ ņĀĢņāü Ļ░æņāüņäĀ ĻĖ░ļŖź ņāüĒā£ņØ╝ ļĢīļÅä ļ░£ņāØĒĢśļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[1]. Ļ░æņāüņāśļłłļ│æņ”ØņØĆ ņĢłĻĄ¼ Ēæ£ļ®┤ņØś ļ│ĆĒÖöļź╝ ņØ╝ņ£╝ņ╝£ Ļ┤æņŗ£ņ”Ø, ņ£ĀļŻ©ņ”Ø, ņØ┤ļ¼╝Ļ░ÉņØ┤ ļ░£ņāØĒĢĀ ņłś ņ׳Ļ│Ā, ņÖĖņĢłĻĘ╝ņØś ņä¼ņ£ĀĒÖöņŚÉ ņØśĒĢ£ ņé¼ņŗ£ ļ░Å ļ│Ąņŗ£Ļ░Ć ļ░£ņāØĒĢĀ ņłś ņ׳ņ£╝ļ®░ ļśÉĒĢ£ ņŚ╝ņ”Øņ£╝ļĪ£ ņØĖĒĢ£ ņĢłņÖĆĒøäļČĆņØś ĒåĄņ”ØļÅä ļ░£ņāØĒĢĀ ņłś ņ׳ļŗż.
ņĢłņÖĆ ĒøäļČĆ ņĪ░ņ¦üņØś ļ│ĆĒÖöļŖö Ļ░æņāüņāśņ×ÉĻĘ╣ĒśĖļź┤ļ¬¼ņłśņÜ®ņ▓┤ ņ×ÉĻ░ĆĒĢŁņ▓┤(thyroid stimulating hormone receptor autoantibody, TSHR Ab)ļĪ£ ņØĖĒĢśņŚ¼ ļ░£ņāØĒĢ£ļŗż. TSHR AbĻ░Ć Ļ░æņāüņāśņ×ÉĻĘ╣ĒśĖļź┤ļ¬¼ņłśņÜ®ņ▓┤(thyroid stimulating hormone receptor, TSHR)ņØś leucine-rich domain A subunitņŚÉ ļČÖĻ▓ī ļÉśļ®┤ adenylate cyclaseļź╝ ĒÖ£ņä▒ĒÖöņŗ£ņ╝£ cyclic adenosine monophosphate (cAMP)ļź╝ ņāØņä▒ĒĢśĻ▓ī ļÉśļ®░ ņØ┤ļŖö Ļ░æņāüņäĀņØä ņä▒ņןņŗ£ĒéżĻ▒░ļéś T3, T4ļź╝ ņāØņé░ĒĢśĻ▓ī ļÉ£ļŗż[2,3]. ņĀĢņāü Ļ░æņāüņäĀņŚÉņä£ļŖö Ļ░æņāüņäĀĒśĖļź┤ļ¬¼(T3, T4)ņØ┤ negative feedbackņ£╝ļĪ£ ļćīĒĢśņłśņ▓┤ņŚÉņä£ TSHņØś ņāØņé░ņØä ņ¢ĄņĀ£ĒĢśņ¦Ćļ¦ī, ļ│æņĀüņØĖ ņāüĒā£ņŚÉņä£ļŖö TSHR AbņØś ņ¦ĆņåŹņĀüņØĖ ņ×ÉĻĘ╣ņ£╝ļĪ£ ņØĖĒĢ┤ ņĢłņÖĆ ņä¼ņ£ĀņĢäņäĖĒżĻ░Ć ņ×ÉĻĘ╣ļÉśļ®░ cAMP ņāØņä▒Ļ│╝ PI3K/Akt ņŗĀĒśĖ Ļ│╝ņĀĢņØä ĒåĄĒĢ┤ Ē׳ņĢīļŻ©ļĪĀņé░ ĒĢ®ņä▒Ļ│╝ ņ¦Ćļ░® ņāØņä▒ņØ┤ ņ”ØĻ░ĆĒĢśĻ▓ī ļÉ£ļŗż. ņØ┤ļĪ£ ņØĖĒĢ┤ Ļ▓░ĻĄŁ ņÖĖņĢłĻĘ╝ņØś ņŚ╝ņ”ØĻ│╝ ļ”╝ĒöäĻĄ¼Ļ░Ć ņ╣©Ēł¼ĒĢśņŚ¼ Ļ░äņ¦ł ņé¼ņØ┤ ļČĆņóģņØ┤ ļ░£ņāØĒĢśļ®░ Ļ░æņāüņāśļłłļ│æņ”ØņØś ņŚ¼ļ¤¼ ņ”ØņāüņØ┤ ļéśĒāĆļéśĻ▓ī ļÉ£ļŗż[4]. ņØ┤Ēøä ņĢłņÖĆ ņä¼ņ£ĀņĢäņäĖĒżĻ░Ć Ļ│╝ļÅäĒĢśĻ▓ī ņāØņé░ĒĢśļŖö glycosamicoglycansļĪ£ ņØĖĒĢ┤ ļČĆņóģņØ┤ ļŹö ņŗ¼ĒĢ┤ņ¦ĆĻ▓ī ļÉ£ļŗż.
ņØ┤ļ¤¼ĒĢ£ ņØ╝ļĀ©ņØś Ļ░æņāüņāśļłłļ│æņ”ØņØś ņ×äņāüņ¢æņāüņØś Ļ│╝ņĀĢņŚÉ ļö░ļØ╝ ņĢłĻĄ¼ļé┤ ĒśłĻ┤ĆņŚÉ ņśüĒ¢źņØä ņżä ņłś ņ׳ļŖöļŹ░, ņØ┤ņĀä ļģ╝ļ¼ĖļōżņŚÉņä£ļÅä ņżæņ”ØļÅäņŚÉ ļö░ļźĖ Ļ░æņāüņāśļłłļ│æņ”ØĻ│╝ ņĢłĻĄ¼ļé┤ ĒśłĻ┤ĆņØś Ļ┤ĆĻ│äļź╝ ĻĘ£ļ¬ģĒĢśĻĖ░ ņ£äĒĢ£ ļģĖļĀźļōżņØ┤ ņ׳ņŚłļŗż. Kurioka et al [5]ņÖĆ Li et al [6]ņØĆ ņ╗¼ļ¤¼ ļÅäĒöīļ¤¼ņ┤łņØīĒīīļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ Ļ░æņāüņāśļłłļ│æņ”ØņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ ņżæņŗ¼ļ¦Øļ¦ēļÅÖļ¦źņØś ĒśłĻ┤Ć ņĀĆĒĢŁņØ┤ ņ”ØĻ░ĆĒĢ£ļŗżļŖö Ļ▓āņØä ļ░ØĒśöĻ│Ā ļ¦Øļ¦ēļÅÖļ¦źņØś Ēśłļźś Ļ│ĄĻĖēņØĆ ņØśļ»Ė ņ׳Ļ▓ī ņżäņ¢┤ļōĀļŗżĻ│Ā ĒĢśņśĆļŗż. ļśÉĒĢ£ Alimgil et al [7]ņØĆ ņĢłņÖĆ ļé┤ņØś ņĢĢļĀź ņ”ØĻ░ĆļĪ£ ļ¦źļØĮļ¦ēĒśłĻ┤Ć ņĀĆĒĢŁņØ┤ ņ╗żņ¦ĆĻ│Ā ņØ┤ņ¢┤ņä£ ņĢłĻĄ¼ņŚÉ Ēśłļźś Ļ│ĄĻĖēņØ┤ ņżäņ¢┤ļōĀļŗżĻ│Ā ļ░ØĒśöļŗż. Ļ░æņāüņāśļłłļ│æņ”ØļÅä TSHR AbņØś ņ”ØĻ░ĆņŚÉ ļö░ļØ╝ ņŚ╝ņ”ØņŚÉ ņØśĒĢ£ ņĢłĻĄ¼ļé┤ ĒśłĻ┤Ć ņ×Éņ▓┤ņØś ļ│ĆĒÖöņÖĆ ĻĘĖņŚÉ ļö░ļźĖ ĒśłļźśņŚÉ ļ│ĆĒÖöĻ░Ć ņ׳ņØä ņłś ņ׳Ļ│Ā, ļśÉļŖö ņŚ╝ņ”ØņŚÉ ņØśĒĢ£ ņÖĖņĢłĻĘ╝ ļ░Å ņĢłņÖĆņĪ░ņ¦üņØś ļČĆņóģņ£╝ļĪ£ ĻĖ░ņØĖĒĢ£ ņĢłĻĄ¼ļé┤ Ēśłļźś ļ│ĆĒÖöņÖĆ ĻĘĖņŚÉ ļö░ļźĖ ĒśłĻ┤ĆļōżņØś ļ│ĆĒÖöĻ░Ć ņ׳ņØä Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż.
ņĄ£ĻĘ╝ ļ╣øĻ░äņäŁļŗ©ņĖĄņ┤¼ņśüĒśłĻ┤ĆņĪ░ņśüņłĀ(optical coherence tomography angiography, OCTA)ņØ┤ Ļ░£ļ░£ļÉśņ¢┤ ņ╗¼ļ¤¼ ļÅäĒöīļ¤¼ņ┤łņØīĒīīļ│┤ļŗż ļŹö ņĀĢĒÖĢĒĢśĻ▓ī ļ¬©ņäĖĒśłĻ┤Ć ņłśņżĆĻ╣īņ¦Ć Ļ┤Ćņ░░ĒĢĀ ņłś ņ׳Ļ▓ī ļÉśņŚłļŗż. OCTAļź╝ ņØ┤ņÜ®ĒĢ£ ņŚ░ĻĄ¼ļĪ£ ļ¦Øļ¦ē ļ¼┤ĒśłĻ┤Ć ļČĆņ£ä(foveal avascular zone, FAZ) ļ│ĆĒÖöļŖö ņŗ£ļĀźņŚÉ ņśüĒ¢źņØä ņżĆļŗżĻ│Ā ņĢīļĀżņĀĖ ņ׳Ļ│Ā, ĒŖ╣Ē׳ ļ¦źļØĮļ¦ēņØĆ ļŗ©ņ£ä ļ¼┤Ļ▓īļŗ╣ Ļ░Ćņן ļ¦ÄņØĆ ĒśłĻ┤Ć ĒØÉļ”äņØä ļ│┤ņØ┤ļŖö ĒśłĻ┤Ć ņĪ░ņ¦üņ£╝ļĪ£ ļ¦Øļ¦ēņÖĖņĖĄĻ│╝ ļ¦Øļ¦ēņāēņåīņāüĒö╝ņŚÉ Ēśłļźśļź╝ Ļ│ĄĻĖēĒĢśļŖöļŹ░ ņŚ¼ļ¤¼ ļ¦Øļ¦ē, ļ¦źļØĮļ¦ē ņ¦łĒÖśĻ│╝ņØś ņŚ░Ļ┤Ćņä▒ņŚÉ ļīĆĒĢ┤ ļ¦ÄņØ┤ ļ│┤Ļ│ĀļÉśņŚłļŗż[8-13]. ĻĘĖņżæ ļ¦źļØĮļ¦ēļæÉĻ╗ś(choroidal thickness, CT)ļŖö ļģĖĒÖöļéś ļ│æņĀüņØĖ ņāüĒā£ņŚÉņä£ ļ¦źļØĮļ¦ē ĒśłņĢĪ ņł£ĒÖśĻ│╝ Ļ┤ĆĻ│äĻ░Ć ņ׳Ļ│Ā, ņ¢ćņĢäņ¦ä ļ¦źļØĮļ¦ēņØĆ ļ¦źļØĮļ¦ēņŚÉ ņČ®ļČäĒĢ£ ĒśłļźśĻ░Ć Ļ│ĄĻĖēļÉśņ¦Ć ļ¬╗ĒĢśĻ│Ā ņ׳ņØīņØä ņØśļ»ĖĒĢ£ļŗżļŖö Ļ▓āņØ┤ ļ░ØĒśĆņĪīļŗż[14,15]. ņØ┤ņŚÉ ņĀĆņ×ÉļōżņØĆ Ļ░æņāüņāśļłłļ│æņ”ØņØä ņ¦äļŗ©ļ░øņØĆ ĒÖśņ×ÉņŚÉņä£ ņ▓½ ļé┤ņøÉņŗ£ņÖĆ ĒĢ£ ļŗ¼ ĒøäņØś TSHR AbņØś ļ│ĆĒÖöņÖĆ OCTAļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ ļ¦Øļ¦ēĒśłĻ┤ĆĻ│╝ ļ¦źļØĮļ¦ēņØś ļ│ĆĒÖöļź╝ ĒÖĢņØĖĒĢśĻ│Ā ĻĘĖ ņŚ░Ļ┤Ćņä▒ņØä ļČäņäØĒĢśņŚ¼ Ēśłņ▓ŁņØś ļ│ĆĒÖöņÖĆ ņØ┤ņŚÉ ļö░ļźĖ ņĢłĻĄ¼ļé┤ ĒśłĻ┤ĆņŚÉ ļ»Ėņ╣śļŖö ņśüĒ¢źņØä ņĢīņĢäļ│┤Ļ│Āņ×É ĒĢśņśĆļŗż.
ļīĆņāüĻ│╝ ļ░®ļ▓Ģ
2018ļģä 9ņøöļČĆĒä░ 2019ļģä 2ņøöĻ╣īņ¦Ć ļ│ĖņøÉņŚÉ ļé┤ņøÉĒĢ£ ĒÖśņ×Éļōż ņżæ Ļ░æņāüņāśļłłļ│æņ”Øņ£╝ļĪ£ ņ¦äļŗ©ļ░øņØĆ 23ļ¬ģ(ņÜ░ņĢł) ĒÖśņ×ÉļōżņØä ļīĆņāüņ£╝ļĪ£ ĒĢśņŚ¼ ņØśļ¼┤ĻĖ░ļĪØņØä ĒøäĒ¢źņĀüņ£╝ļĪ£ ļČäņäØĒĢśņśĆļŗż. ļ│Ė ņŚ░ĻĄ¼ļŖö ļ¬©ļōĀ Ļ│╝ņĀĢņŚÉņä£ ĒŚ¼ņŗ▒ĒéżņäĀņ¢Ė(Declaration of Helsinki)ņØä ņżĆņłśĒĢśņśĆņ£╝ļ®░, ļ│ĖņøÉ ņ×äņāüņŗ£ĒŚśņŗ¼ņé¼ņ£äņøÉĒÜī(Institutional Review Board, IRB)ņØś ņŖ╣ņØĖņØä ļ░øņĢśļŗż(ņŖ╣ņØĖ ļ▓łĒśĖ: 2020-02-029).
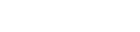
Ļ░æņāüņāśļłłļ│æņ”ØņØś ņ¦äļŗ© ĻĖ░ņżĆņØĆ ļé┤ļČäļ╣ä ļé┤Ļ│╝ņŚÉņä£ Ļ░æņāüņäĀ ĻĖ░ļŖź ņØ┤ņāüņ£╝ļĪ£ ņ╣śļŻī ņżæņØĖ ĒÖśņ×ÉĻ░Ć ļłłĻ║╝ĒÆĆļÆżļŗ╣Ļ╣Ć, ļłłĻ║╝ĒÆĆļČĆņóģ, ņĢłĻĄ¼ļÅīņČ£ ļō▒ Ļ░ØĻ┤ĆņĀüņØĖ ņ”ØņāüņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ļĪ£ ĒĢśņśĆļŗż[16]. ĒśłņĢĪĻ▓Ćņé¼ļź╝ ĒåĄĒĢ┤ TSHR Ab titerĻ░Ć 1.5 IU/L ņØ┤ņāüņØ┤ļ®┤ ļ│Ė ņŚ░ĻĄ¼ņŚÉ ĒżĒĢ©ļÉśņŚłļŗż. ĒÖśņ×ÉņØś ļéśņØ┤, ņä▒ļ│ä, ņŗ£ļĀźņØä ņĪ░ņé¼ĒĢśņśĆĻ│Ā, ļ¦Øļ¦ē ņ¦łĒÖś ļ░Å ļ¦Øļ¦ē ņłśņłĀļĀźņØ┤ ņ׳Ļ▒░ļéś Ļ░æņāüņäĀ ņ¦łĒÖśņØä ņĀ£ņÖĖĒĢ£ Ļ│ĀĒśłņĢĢ ļō▒ ņĀäņŗĀ ņ¦łĒÖśņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ļŖö ņĀ£ņÖĖĒĢśņśĆļŗż. Swept-source OCT (SS-OCT, DRI-OCT; Topcon, Tokyo, Japan)ļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ OCTAļź╝ Ļ▓Ćņé¼ĒĢśņśĆĻ│Ā, Ēæ£ņĖĄļ¬©ņäĖĒśłĻ┤Ćņ┤Ø(superficial capillary plexus layer, SCP)ņÖĆ ņŗ¼ļČĆļ¬©ņäĖĒśłĻ┤Ćņ┤Ø(deep capillary plexus layer, DCP)ļŖö ņĀĢļ®┤ OCTAņØś ņé¼ņ¦äņŚÉņä£ ņåīĒöäĒŖĖņø©ņ¢┤ņŚÉ ļé┤ņןļÉ£ ļÅäĻĄ¼ļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ FAZ Ēü¼ĻĖ░ļź╝ ņĖĪņĀĢĒĢśņśĆļŗż(Fig. 1A, B). CTļŖö ĒĢ£ ļ¬ģņØś Ļ▓Ćņé¼ņ×ÉĻ░Ć OCT ņåīĒöäĒŖĖņø©ņ¢┤ņŚÉ ļé┤ņןļÉ£ ņłśļÅÖ ĻĖĖņØ┤ ņĖĪņĀĢ ļÅäĻĄ¼ļź╝ ņé¼ņÜ®ĒĢśņŚ¼ ĒÖ®ļ░śņżæņŗ¼ļČĆ ļ¦Øļ¦ēņāēņåīņāüĒö╝ņŚÉņä£ ļ¦źļØĮļ¦ē Ēü░ ĒśłĻ┤ĆņØś ļ░öĻ╣źļ®┤Ļ╣īņ¦Ć ņĖĪņĀĢĒĢ£ ņżæņŗ¼ņÖĆņÖĆ ĻĘĖ ņØ┤ņĖĪ, ļ╣äņĖĪ 100 ╬╝mņŚÉ ļé┤ļ”░ ņäĖ ņłśņ¦üņäĀ ĻĖĖņØ┤ņØś ĒÅēĻĘĀņ╣śļź╝ ņé¼ņÜ®ĒĢśņśĆļŗż(Fig. 1C). ņØ┤ ļ░®ļ▓ĢņØĆ ņżæņŗ¼ņÖĆņÖĆ ņØĖņĀæĒĢ£ ļ¦źļØĮļ¦ēļæÉĻ╗śņØś ĒÅēĻĘĀņ╣śļź╝ ņé¼ņÜ®ĒĢ£ ļģ╝ļ¼Ė[17,18]ņØä ņ░ĖņĪ░ĒĢśņśĆĻ│Ā, ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ļŖö ļ¦Øļ¦ēņżæņŗ¼ļČĆņØś ņĀĢĒÖĢĒĢ£ CTļź╝ ņĖĪņĀĢĒĢśĻĖ░ ņ£äĒĢ┤ ņżæņŗ¼ņÖĆņÖĆ ĻĘĖ ņØ┤ņĖĪ, ļ╣äņĖĪ 100 ╬╝m ļ▓öņ£äļĪ£ ņĀĢĒĢśņśĆļŗż. 1 mm ņżæņŗ¼ņÖĆņÖĆ 3 mm ņżæņŗ¼ņÖĆ ļČĆĻĘ╝ sCPDļŖö ĒÖ®ļ░śņØä ĻĖ░ņżĆņ£╝ļĪ£ ņ¦Ćļ”ä 1 mm ņøÉ ļé┤ļČĆņŚÉņä£ņØś sCPDņÖĆ ņ¦Ćļ”ä 3 mm ņøÉ ļé┤ļČĆņŚÉņä£ņØś sCPDļź╝ ņĖĪņĀĢĒĢśņŚ¼ ļ╣äĻĄÉĒĢśņśĆļŗż. ņ¦Ćļ”ä 3 mm ņøÉ ļé┤ļČĆņØś sCPDļŖö ņ¦Ćļ”ä 1 mmļČĆĒä░ 3 mmĻ╣īņ¦ĆņØś ļ▓öņ£äļź╝ ņ£äņ¬Į, ņĢäļלņ¬Į, ĻĘĆņ¬Į, ņĮöņ¬Į 4ļČĆļČäņ£╝ļĪ£ ļéśļłäņ¢┤ Ļ░üĻ░üņØś sCPDļź╝ ņĖĪņĀĢĒĢ£ ļÆż ļ¬©ļæÉ ĒĢ®ĒĢ£ Ļ░ÆņØä 4ļĪ£ ļéśļłł Ļ▓āņ£╝ļĪ£ ņĀĢņØśĒĢśņśĆļŗż(Fig. 1D) [19]. ļé┤ņøÉ 1Ļ░£ņøö Ēøä Ļ░ÖņØĆ ļ░®ļ▓Ģņ£╝ļĪ£ SCP, DCPņØś FAZ Ēü¼ĻĖ░ņÖĆ CT, ņżæņŗ¼ņÖĆņÖĆ ņżæņŗ¼ņÖĆļČĆĻĘ╝ sCPDļź╝ ņĖĪņĀĢĒĢśņśĆļŗż(Fig. 1E-H). ĒåĄĻ│äļŖö IBM SPSS Statistics 25.0.0 (IBM Co., Armonk, NY, USA)ņØä ņØ┤ņÜ®ĒĢśņŚ¼ Ēö╝ņ¢┤ņŖ© ņāüĻ┤ĆĻ┤ĆĻ│ä ļČäņäØ(PearsonŌĆÖs correlation analysis)ņØä ņŗ£Ē¢ēĒĢśņśĆņ£╝ļ®░ p-valueĻ░Ć 0.05 ļ»Ėļ¦īņØ┤ļ®┤ ĒåĄĻ│äĒĢÖņĀüņ£╝ļĪ£ ņ£ĀņØśĒĢ£ Ļ▓āņ£╝ļĪ£ Ļ░äņŻ╝ĒĢśņśĆļŗż.
Ļ▓░ Ļ│╝
ĒÖśņ×ÉļōżņØś ĒÅēĻĘĀ ļéśņØ┤ļŖö 43.30 ┬▒ 16.16ņäĖņśĆĻ│Ā, ņŚ¼ņ×ÉĻ░Ć ņĀäņ▓┤ 23ļ¬ģ ĒÖśņ×É ņżæ 18ļ¬ģ(78%)ņ£╝ļĪ£ ļŹö ļ¦ÄņĢśļŗż. ĒÅēĻĘĀ ņĄ£ļīĆĻĄÉņĀĢņŗ£ļĀź(logMAR)ņØĆ 0.08 ┬▒ 0.14ņśĆņ£╝ļ®░, ĒÅēĻĘĀ ņĢłņĢĢņØĆ 14.91 ┬▒ 2.91 mmHgņśĆļŗż. ņ▓śņØī ļé┤ņøÉ ļŗ╣ņŗ£ņØś ĒÖśņ×ÉļōżņØś ĒÅēĻĘĀ TSHR AbļŖö 11.47 ┬▒ 11.22 IU/L (ņĀĢņāüņØĆ 1.5 IU/L ļ»Ėļ¦ī)ņśĆĻ│Ā, ĒÅēĻĘĀ sFAZļŖö 289,319.95 ┬▒ 166,409.06 mm2, ĒÅēĻĘĀ dFAZļŖö 312,646.04 ┬▒ 167,368.65 mm2ļĪ£ ņĖĪņĀĢļÉśņŚłļŗż. ļé┤ņøÉ ļŗ╣ņŗ£ņØś ĒÅēĻĘĀ 1 mm ņżæņŗ¼ņÖĆ, 3 mm ņżæņŗ¼ņÖĆļČĆĻĘ╝ sCPDļŖö Ļ░üĻ░ü 19.50 ┬▒ 4.99%, 54.62 ┬▒ 2.84%ņśĆĻ│Ā, ĒÅēĻĘĀ CTļŖö 189.22 ┬▒ 73.34 ╬╝mņśĆļŗż(Table 1). ņØ┤ņÖĖņŚÉ Ļ░üļ¦ēĻ│╝ ļ¦Øļ¦ēņØś ĒŖ╣ņØ┤ ņåīĻ▓¼ņØĆ ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśļŗż.
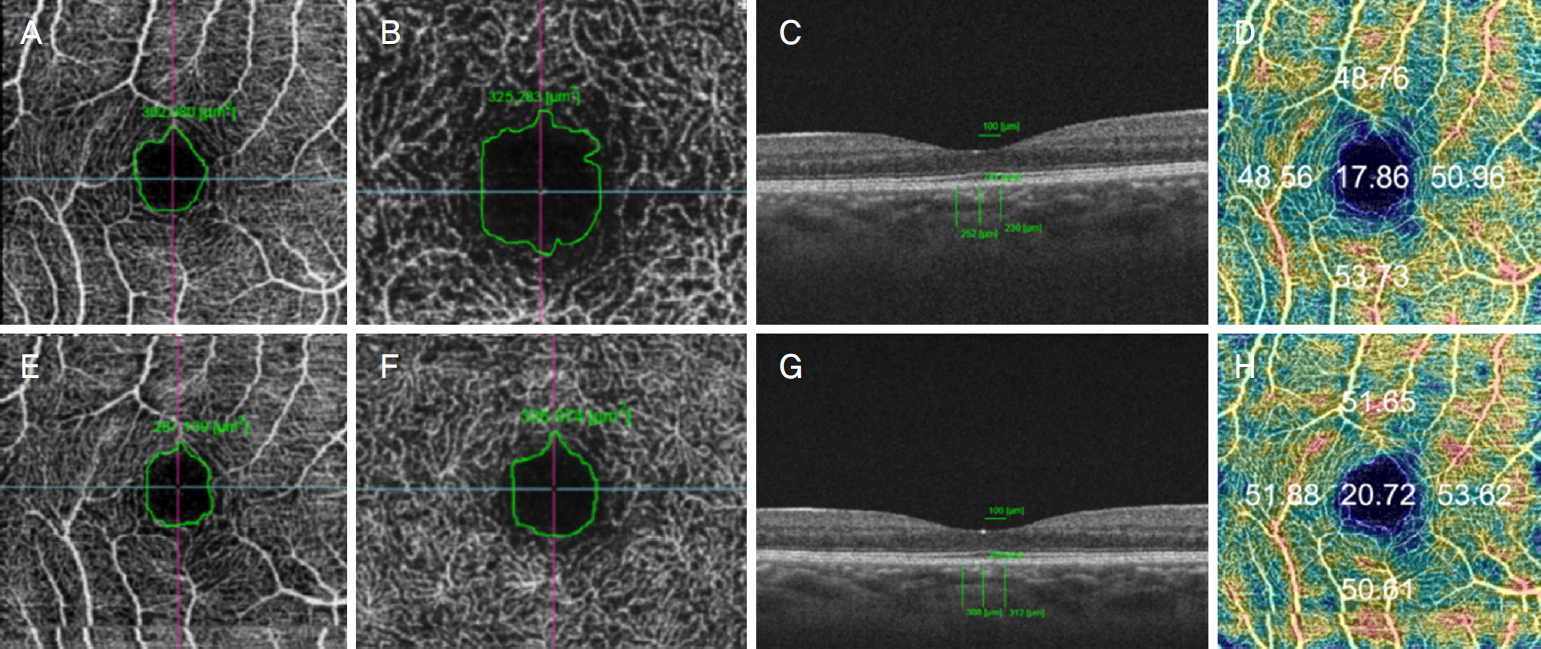
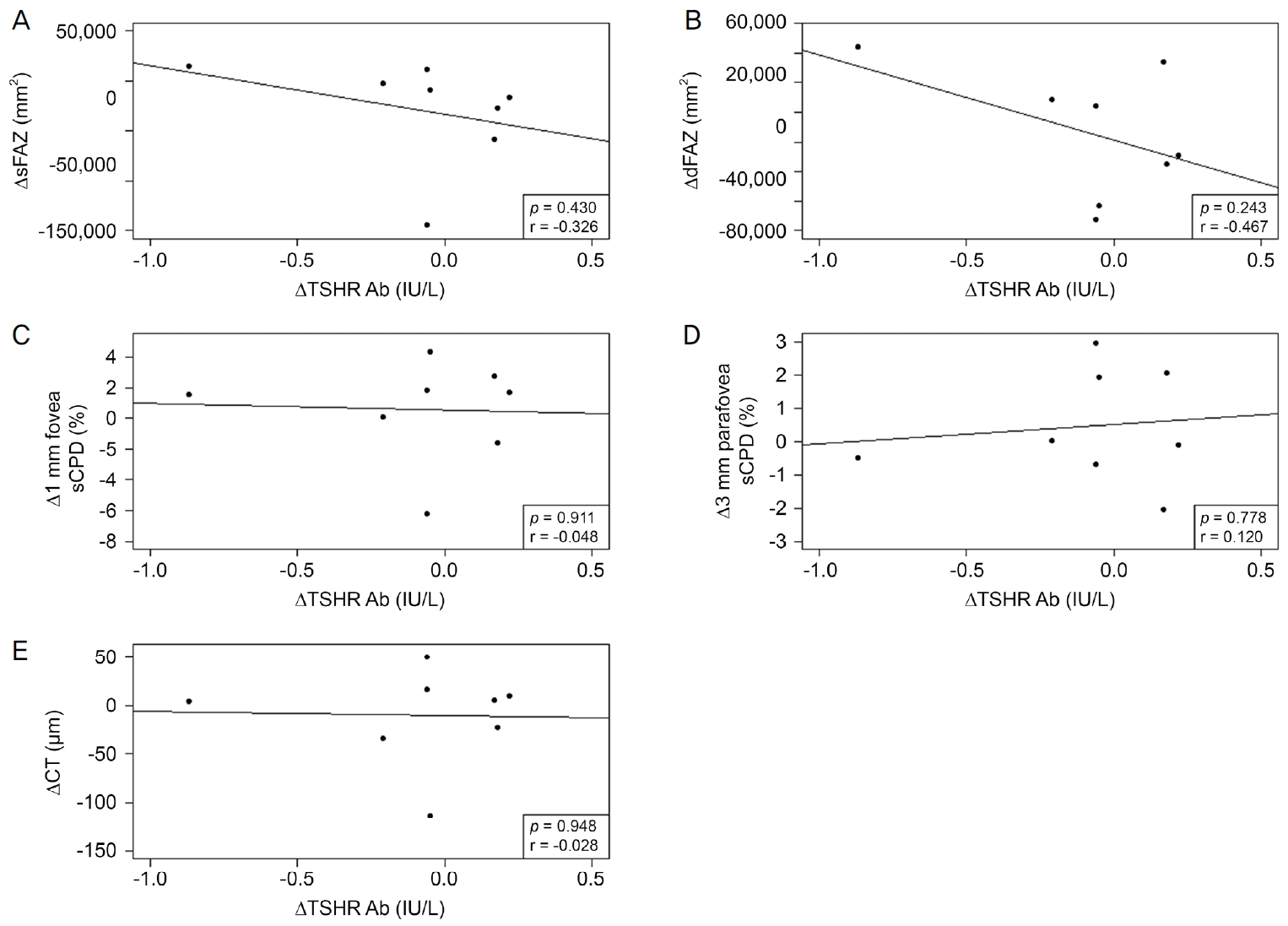
1Ļ░£ņøö ļÆżņØś TSHR AbņØś Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢ£ ĒÖśņ×ÉņØś ĒÅēĻĘĀņØĆ 9.75 ┬▒ 12.37 IU/LņśĆņ£╝ļ®░, sFAZļŖö 255,471.75 ┬▒ 152,796.77 mm2ņśĆĻ│Ā dFAZļŖö 297,799.70 ┬▒ 130,201.18 mm2ņśĆļŗż. 1Ļ░£ņøö ļÆżņØś ĒÅēĻĘĀ 1 mm ņżæņŗ¼ņÖĆ, 3 mm ņżæņŗ¼ņÖĆļČĆĻĘ╝ sCPDļŖö 20.47 ┬▒ 5.82%, 54.11 ┬▒ 2.41%ņśĆņ£╝ļ®░, CTļŖö 193.67 ┬▒ 64.77 ╬╝mņśĆļŗż. 1Ļ░£ņøöĻ░ä TSHR AbņØś ļ│ĆĒÖöļ¤ēņØä ļ│╝ ņłś ņ׳ņŚłļŹś 21ļ¬ģ ĒÖśņ×ÉņØś ĒÅēĻĘĀ ļ│ĆĒÖöļ¤ēņØĆ 0.57 ┬▒ 3.72 IU/LņśĆĻ│Ā, sFAZ, dFAZņØś ļ│ĆĒÖöļ¤ēņØä ļ│╝ ņłś ņ׳ņŚłļŹś 20ļ¬ģ ĒÖśņ×ÉņØś ĒÅēĻĘĀ ļ│ĆĒÖöļ¤ēņØĆ Ļ░üĻ░ü 26,288.00 ┬▒ 84,975.21 mm2, 11,685.15 ┬▒ 63,747.71 mm2ļĪ£ ņĖĪņĀĢļÉśņŚłļŗż. 1 mm ņżæņŗ¼ņÖĆ, 3 mm ņżæņŗ¼ņÖĆ ļČĆĻĘ╝ sCPDņØś ļ│ĆĒÖöļ¤ēņØä ļ│╝ ņłś ņ׳ņŚłļŹś 21ļ¬ģ ĒÖśņ×ÉņØś ĒÅēĻĘĀ ļ│ĆĒÖöļ¤ēņØĆ -1.07 ┬▒ 3.82%, 0.31 ┬▒ 2.39%ņśĆņ£╝ļ®░, CTņØś ļ│ĆĒÖöļ¤ēņØä ļ│╝ ņłś ņ׳ņŚłļŹś 21ļ¬ģņØś ĒÖśņ×ÉņØś ĒÅēĻĘĀ ļ│ĆĒÖöļ¤ēņØĆ -2.76 ┬▒ 45.36 ╬╝mļĪ£ ņĖĪņĀĢļÉśņŚłļŗż. 1Ļ░£ņøöĻ░äņØś TSHR AbņØś ļ│ĆĒÖöņŚÉ ļö░ļźĖ ļ¦Øļ¦ē, ļ¦źļØĮļ¦ē ņāüĒā£ ļ│ĆĒÖöļŖö sFAZ, dFAZ, 1 mm ņżæņŗ¼ņÖĆ sCPDņŚÉņä£ ņāüĻ┤ĆĻ│äņłśĻ░Ć Ļ░üĻ░ü 0.173, 0.073, 0.266ņØ┤ņŚłņ£╝ļ®░, ņØ┤ ņżæ 1 mm ņżæņŗ¼ņÖĆ sCPDņŚÉņä£ļŖö ņĢĮĒĢ£ ņ¢æņØś Ļ▓ĮĒ¢źņä▒ņØä ļ│┤ņØ┤ļéś, ĒåĄĻ│äņĀüņ£╝ļĪ£ ņ£ĀņØśļ»ĖĒĢśņ¦Ć ņĢŖņĢśļŗż(p=0.465, p=0.759, p=0.224; Fig. 2A-C). ļīĆņĪ░ņĀüņ£╝ļĪ£ 3 mm ņżæņŗ¼ņÖĆļČĆĻĘ╝ sCPDņÖĆ CTņŚÉņä£ļŖö ņāüĻ┤ĆĻ│äņłśĻ░Ć -0.185, -0.16ņØ┤ņŚłņ£╝ļéś ļŗżļźĖ ļ│ĆņłśļōżĻ│╝ ļ¦łņ░¼ Ļ░Ćņ¦ĆļĪ£ Ļ▓ĮĒ¢źņä▒ņØ┤ļéś ĒåĄĻ│äņĀüņØĖ ņ£ĀņØśņä▒ņØĆ ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśļŗż(p=0.421, p=0.487; Fig. 2D, E). ņČöĻ░ĆņĀüņ£╝ļĪ£ TSHR AbņØś ņłśņ╣śĻ░Ć 1.5 IU/L ļ»Ėļ¦īņØĖ ĒÖśņ×É 8ļ¬ģņØä ļīĆņāüņ£╝ļĪ£ ļČäņäØĒĢ£ Ļ▓░Ļ│╝ sFAZ, dFAZ, 1 mm ņżæņŗ¼ņÖĆ sCPD, CTņŚÉņä£ ņāüĻ┤ĆĻ│äņłśĻ░Ć Ļ░üĻ░ü -0.326, -0.467, -0.048, -0.028ļĪ£ ņØīņØś Ļ▓ĮĒ¢źņä▒ņØä ļ│┤ņśĆņ£╝ļ®░(p=0.430, p=0.243, p=0.911, p=0.948), 3 mm ņżæņŗ¼ņÖĆļČĆĻĘ╝ sCPDņŚÉņä£ ņāüĻ┤ĆĻ│äņłśĻ░Ć 0.120ņ£╝ļĪ£ ņ¢æņØś Ļ▓ĮĒ¢źņä▒ņØä ļ│┤ņśĆĻ│Ā(p=0.778) ļ¬©ļōĀ Ļ░ÆņŚÉņä£ ĒåĄĻ│äņĀüņ£╝ļĪ£ ņ£ĀņØśļ»ĖĒĢśņ¦Ć ņĢŖņĢśļŗż(Fig. 3).
Ļ│Ā ņ░░
Ļ░æņāüņāśļłłļ│æņ”Øņ£╝ļĪ£ ņ¦äļŗ© ļ░øĻ│Ā ļ│Ė ņŚ░ĻĄ¼ņŚÉ ņ░ĖĻ░ĆĒĢ£ ĒÖśņ×ÉņØś ņ▓½ ļé┤ņøÉņŗ£ TSHR AbļŖö 11.47 ┬▒ 11.22 IU/LņśĆĻ│Ā, 1Ļ░£ņøö ļÆżņØś ļ│ĆĒÖöļ¤ēņØś ĒÅēĻĘĀņØĆ 0.57 ┬▒ 3.72 IU/LņśĆļŗż. ĒŖ╣ņĀĢ ĒÖśņ×ÉņØś ņÜ░ņĢłņØä ĻĖ░ņżĆņ£╝ļĪ£ ņāüĻ┤ĆĻ┤ĆĻ│äļź╝ Ēæ£ņŗ£ĒĢśņŚ¼ Ļ░ü ļ│ĆņłśņØś ņ¢æĻ│╝ ņØīņØś ņāüĻ┤ĆĻ┤ĆĻ│äļź╝ ĒÖĢņØĖĒĢĀ ņłś ņ׳ņŚłļŗż. TSHR AbĻ░Ć ņ”ØĻ░ĆĒĢĀņłśļĪØ ļ¦Øļ¦ē ņżæņŗ¼ņÖĆ 1 mm ņ¦Ćļ”ä ņĢłņØś sCPDļŖö ļŹö ņ╗żņ¦ĆļŖö Ļ▓ĮĒ¢źņØ┤ ņ׳ņŚłņ£╝ļéś, ļ¬©ļōĀ ļ│ĆņłśņØś ĒåĄĻ│äņĀü ņ£ĀņØśņä▒ņØĆ ņŚåņŚłļŗż.
TSHR AbļŖö ļ»ĖņäĖĒśłĻ┤ĆĻ│äņŚÉ ņ╣©ņ░®ļÉśņ¢┤ ņ׳ļŖö ĒĢŁņ▓┤ņØś ņ¢æņØä ļ░śņśüĒĢśļ®░, ņØ┤ļŖö ļłłņØś ņ×ÉĻ░Ćļ®┤ņŚŁ Ļ│╝ņĀĢņØä ņ┤ēļ░£ņŗ£Ēé¼ ļ┐É ņĢäļŗłļØ╝ ņ¦ĆņåŹņĀüņ£╝ļĪ£ ņ£Āņ¦ĆĒĢśļŖö ņŚŁĒĢĀņØä ĒĢśļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[20]. Kumar et al [4]ņØĆ TSHR AbņØś ņ¦ĆņåŹņĀüņØĖ ņ×ÉĻĘ╣ņ£╝ļĪ£ ņØĖĒĢ┤ ņĢłņÖĆ ņä¼ņ£ĀņĢäņäĖĒżĻ░Ć ņ×ÉĻĘ╣ļÉśļ®░ ņØ┤Ēøä Ē׳ņĢīļŻ©ļĪĀņé░ ĒĢ®ņä▒Ļ│╝ ņ¦Ćļ░® ņāØņä▒ņØ┤ ņ”ØĻ░ĆĒĢśĻ▓ī ļÉ£ Ēøä Ļ▓░ĻĄŁ ņÖĖņĢłĻĘ╝ņØś ņŚ╝ņ”ØĻ│╝ ļ”╝ĒöäĻĄ¼Ļ░Ć ņ╣©Ēł¼ĒĢśņŚ¼ Ļ░äņ¦ł ņé¼ņØ┤ ļČĆņóģņØ┤ ļ░£ņāØĒĢśļ®░ Ļ░æņāüņāśļłłļ│æņ”ØņØś ņŚ¼ļ¤¼ ņ”ØņāüņØ┤ ļéśĒāĆļéśĻ▓ī ļÉ£ļŗżĻ│Ā ņ¢ĖĻĖēĒĢśņśĆļŗż. ņØ┤Ēøä ņĢłņÖĆ ņä¼ņ£ĀņĢäņäĖĒżĻ░Ć Ļ│╝ļÅäĒĢśĻ▓ī ņāØņé░ĒĢśļŖö ĻĖĆļ”¼ņĮöņé¼ļ»ĖļģĖĻĖĆļ”¼ņ╣Ėņ£╝ļĪ£ ņØĖĒĢ┤ ļČĆņóģņØ┤ ļŹö ņŗ¼ĒĢ┤ņ¦ĆĻ▓ī ļÉśļŖöļŹ░, ĒŖ╣Ē׳ ĒØĪņŚ░Ļ│╝ ņģĆļĀłļŗłņøĆ ļČĆņĪ▒, Ļ│Āņ¦ĆĒśłņ”ØņØĆ Ļ░üĻ░ü ņ¦Ćļ░®ņāØņä▒ ņ┤ēņ¦ä, ņé░ĒÖö ņ×æņÜ®, ņŚ╝ņ”Ø ņ×æņÜ®ņØä ņ┤ēņ¦äņŗ£ņ╝£ Ļ░æņāüņāśļłłļ│æņ”ØņØś ņ×äņāüņ¢æņāüņØś ņ¦äĒ¢ēĻ│╝ ņŚ░Ļ┤ĆņØ┤ ņ׳ļŖö Ļ▓āņ£╝ļĪ£ ļ░ØĒśĆņĪīļŗż[21-23].
ņŚ¼ļ¤¼ ņ¦łĒÖśļōżņŚÉ ņØśĒĢ£ ņĀäņŗĀ ņŚ╝ņ”Ø ņāüĒā£ļŖö ĻĘĖ ņ¦łĒÖśņØś ĒÖ£ņä▒ļÅäņŚÉ ļö░ļØ╝ ĒśłĻ┤ĆņØ┤ ĒÆŹļČĆĒĢ£ ļ¦źļØĮļ¦ēĒśłĻ┤Ć ņĪ░ņ¦üņŚÉ ņ¦üĻ░äņĀæņĀüņØĖ ņśüĒ¢źņØä ļ»Ėņ╣£ļŗżĻ│Ā ņĢīļĀżņĀĖ ņ׳ļŖöļŹ░, ņŻ╝ļĪ£ ĒśłĻ┤Ćļé┤Ēö╝ņäĖĒżņØś ļ│ĆĒÖöĻ░Ć ņØ╝ņ¢┤ļéśĻ▒░ļéś ņ╣©ņ£żņä▒ ņäĖĒżņÖĆ ļ®┤ņŚŁļ│ĄĒĢ®ņ▓┤ņØś ņ╣©ņ░®ņ£╝ļĪ£ ĒśłĻ┤ĆņØś ĻĄ¼ņĪ░Ļ░Ć ļ│ĆĒśĢļÉśĻ│Ā ĒśłņĢĪļ¦Øļ¦ēņןļ▓ĮņØś ĒīīĻ┤┤ļĪ£ ļłäņČ£ņØ┤ ņØ╝ņ¢┤ļéśļ®░ ņŗĀņāØĒśłĻ┤ĆņØ┤ ņāØĻĖ░ļŖö ļō▒ ĒśłĻ┤Ć ņĪ░ņ¦üņØś ļ│ĆĒÖöĻ░Ć ņØ╝ņ¢┤ļé£ļŗżĻ│Ā ņĢīļĀżņĀĖ ņ׳ļŗż[24]. Ļ░æņāüņāśļłłļ│æņ”ØļÅä TSHR AbņØś ņ”ØĻ░ĆņŚÉ ļö░ļØ╝ ņĢłĻĄ¼ļé┤ Ēśłļźś ļ│ĆĒÖöņÖĆ ĻĘĖņŚÉ ļö░ļźĖ ĒśłĻ┤ĆļōżņØś ļ│ĆĒÖöĻ░Ć ņ׳ņØä Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż.
Ļ░æņāüņāśļłłļ│æņ”ØņŚÉ ņØśĒĢ£ ĒśłĻ┤Ć ņ×Éņ▓┤ņØś ļ│ĆĒÖöņŚÉ ļīĆĒĢ£ ņØ┤ņĀä ļģ╝ļ¼ĖļōżņØä ļ│┤ļ®┤, ĒÖ£ļÅÖĻĖ░ņØś Ļ░æņāüņāśļłłļ│æņ”ØņŚÉņäĀ Ļ░ĢļĀźĒĢ£ ĒśłĻ┤ĆņłśņČĢņĀ£ņØĖ endothelin-1ņØś ņśüĒ¢źņ£╝ļĪ£ ĒśłļźśĻ░Ć Ļ░ÉņåīļÉśĻ│Ā, ļ¦Øļ¦ēĒśłĻ┤ĆņŚÉ ņ×ÉĻ░ĆĒĢŁņ▓┤Ļ░Ć ņ╣©ņ░®ļÉśņ¢┤ ņ£Āļ░£ļÉśļŖö ņŚ╝ņ”Ø ņ×æņÜ®ņ£╝ļĪ£ ļ¦Øļ¦ēļ¬©ņäĖĒśłĻ┤ĆņØ┤ ĒīīĻ┤┤ļÉśņ¢┤ ļ░ĆļÅäļŖö Ļ░ÉņåīĒĢ£ļŗżĻ│Ā ņĢīļĀżņĀĖ ņ׳ļŗż[25-27]. ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ļŖö 1 mm ņżæņŗ¼ņÖĆ sCPDņØś ņ”ØĻ░ĆņØś Ļ▓ĮĒ¢źņä▒ņØä ļ│╝ ņłś ņ׳ņŚłļŖöļŹ░, ĻĖ░ņĪ┤ņØś ņŚ░ĻĄ¼[27]ļŖö ĒĢ£ ņŗ£ņĀÉņŚÉ ņĀĢņāüņØĖĻ│╝ Ļ░æņāüņāśļłłļ│æņ”Ø ĒÖśņ×Éļź╝ ļ╣äĻĄÉĒĢśņŚ¼ ņŚ░ĻĄ¼ļÉ£ ļ░śļ®┤, ļ│Ė ņŚ░ĻĄ¼ļŖö Ļ░æņāüņāśļłłļ│æņ”Øņ£╝ļĪ£ ņ¦äļŗ© ļ░øņØĆ ņé¼ļ×īļ¦īņØä ļīĆņāüņ£╝ļĪ£ ņ▓śņØī ļé┤ņøÉ ņŗ£ņĀÉĻ│╝ 1Ļ░£ņøö Ēøä ļé┤ņøÉ ņŗ£ņĀÉņØś ļ│ĆĒÖöļ¤ēņØä ļ│┤ņĢśļŗżļŖö ņĀÉņŚÉņä£ ļŗżļź┤ļŗż. ļīĆņĪ░ņĀüņ£╝ļĪ£ ĒÖ£ļÅÖĻĖ░ Ļ░æņāüņāśļłłļ│æņ”ØņŚÉņä£ ļ¦Øļ¦ēļ¬©ņäĖĒśłĻ┤Ćļ░ĆļÅäĻ░Ć ņ”ØĻ░ĆĒĢ£ļŗżļŖö Ye et al [28]ņØś ļ│┤Ļ│ĀļÅä ņ׳ņŚłļŗż. ņØ┤ ņŚ░ĻĄ¼ ņŚŁņŗ£ ņĀĢņāüņØĖĻ│╝ Ļ░æņāüņāśļłłļ│æņ”Ø ĒÖśņ×Éļź╝ ļ╣äĻĄÉĒĢ£ ļģ╝ļ¼Ėņ£╝ļĪ£ ļ¦Øļ¦ēļ¬©ņäĖĒśłĻ┤Ćļ░ĆļÅäņØś ņ”ØĻ░ĆļŖö ņĀĢļ¦źņÜĖĒśłņŚÉ ņØśĒĢ£ Ēśłļźś ņ¦ĆņŚ░ņŚÉ ļīĆĒĢ£ Ļ▓░Ļ│╝ļĪ£ Ļ░ĆņĀĢĒ¢łļŗż. ņØ┤ļŖö ļ│Ė ņŚ░ĻĄ¼ņØś 1 mm sCPDņØś ņ”ØĻ░Ć Ļ▓ĮĒ¢źņä▒Ļ│╝ ņØ╝ļ¦źņāüĒåĄĒĢśļŖöļŹ░, ņ£ä ļæÉ ļģ╝ļ¼Ė [27,28]ņØś ņ░©ņØ┤ņĀÉņØĆ Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢ£ ņŗ£ĻĖ░ņŚÉ ļö░ļźĖ Ļ░æņāüņāśļłłļ│æņ”Ø ĒÖśņ×ÉņØś ņżæņ”ØļÅäņØś ņ░©ņØ┤ļĪ£ ņāØĻ░üļÉ£ļŗżĻ│Ā ļ│┤Ļ│ĀĒĢśņśĆļŗż. ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ ņ▓½ ļé┤ņøÉņŗ£ ņ×äņāüņ¢æņāüņŚÉ ļö░ļźĖ clinical activity score (CAS), NOSPECS classification, VISA inflammatory scoreļź╝ ņØ┤ņÜ®ĒĢśņ¦Ć ļ¬╗ĒĢ£ Ļ▓āņØĆ ņ£ĀņØśļ»ĖĒĢśņ¦Ć ļ¬╗ĒĢ£ Ļ▓░Ļ│╝ņŚÉ ļīĆĒĢ£ biasĻ░Ć ļÉĀ ņłś ņ׳ļŗż. ņĀĆņ×ÉļōżņØĆ ņČöĻ░ĆļĪ£ ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ Ļ░æņāüņāśļłłļ│æņ”ØļĪ£ ņ¦äļŗ©ļÉ£ ĒÖśņ×É ņżæ TSHR AbņØś ņłśņ╣śĻ░Ć 1.5 IU/L ļ»Ėļ¦īņØĖ 8ļ¬ģņØś ĒÖśņ×ÉņŚÉ ļīĆĒĢśņŚ¼ Ļ░ÖņØĆ Ļ▓Ćņé¼ļź╝ ĒĢśņŚ¼ ĒåĄĻ│äĒĢÖņĀü ļČäņäØņØä ĒĢ£ Ļ▓░Ļ│╝, ņ▓½ ļé┤ņøÉņŗ£ņÖĆ 1Ļ░£ņøö ļÆżņØś Ēśłņ▓Ł ņłśņ╣śņØś ļ│ĆĒÖöņŚÉ ļö░ļźĖ OCTA ņĖĪņĀĢņ╣ś ļ│ĆĒÖöņŚÉ ļö░ļź┤ļ®┤ ļ¬©ļōĀ ļ│ĆņłśņŚÉ ĒåĄĻ│äņĀü ņ£ĀņØśņä▒ņØĆ ņŚåņŚłņ£╝ļéś, sFAZņÖĆ dFAZĻ░Ć ņØīņØś Ļ▓ĮĒ¢źņä▒ņØä ļ│┤ņśĆļŗż(Fig. 3A, B). 1 mm ņżæņŗ¼ņÖĆ sCPD, 3 mm ņżæņŗ¼ņÖĆļČĆĻĘ╝ sCPDņÖĆ CTņŚÉņä£ļŖö Ļ▓ĮĒ¢źņä▒ņØä ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśļŗż(Fig. 3C-E). ņØ┤ļŖö TSHR AbĻ░Ć ņ”ØĻ░ĆĒĢĀņłśļĪØ sFAZ, dFAZ Ēü¼ĻĖ░Ļ░Ć ņ×æņĢäņ¦ĆļŖö Ļ▓ĮĒ¢źņä▒ņØä ļ│┤ņØĖļŗżļŖö Ļ▓āņØĖļŹ░, 1.5 IU/L ņØ┤ņāüļ¦ī ĒżĒĢ©Ē¢łļŹś ļ│Ė ņŚ░ĻĄ¼ņÖĆ ĒåĄĻ│äņĀüņ£╝ļĪ£ ņ£ĀņØśņä▒ņØ┤ ņŚåļŖö Ļ▓āņØĆ Ļ░Öņ£╝ļéś Ļ▓ĮĒ¢źņä▒ņØ┤ ļŗżļźĖ Ļ▓░Ļ│╝Ļ░Ć ļÅäņČ£ļÉśņŚłļŗż. ņØ┤ Ļ▓░Ļ│╝ļŖö TSHR AbņØś ņżæņ”ØļÅäņŚÉ ļö░ļØ╝ ĒśłĻ┤ĆņŚÉ ņśüĒ¢źņØä ļ»Ėņ╣śļŖö ņĀĢļÅäĻ░Ć ļŗżļź┤ļŗżĻ│Ā ņāØĻ░üĒĢĀ ņłś ņ׳Ļ▓Āļŗż. ļö░ļØ╝ņä£ Ē¢źĒøä ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņ░ĖņŚ¼ ņØĖņøÉņØä ļŖśļĀż Ļ░æņāüņāś ļłłļ│æņ”Ø ĒÖśņ×ÉņØś Ēśłņ▓Ł ĒĢŁņ▓┤ļź╝ TSHR Ab ņØ┤ņÖĖņŚÉ thyroid-stimulating autoantibodiesļÅä ĒĢ©Ļ╗ś Ļ▓Ćņé¼ĒĢśĻ│Ā, ņØ┤ņŚÉ ļŹöĒĢśņŚ¼ ĒĢŁņ▓┤ņØś ņżæņ”ØļÅäņŚÉ ļö░ļØ╝ ĻĄ░ņØä ļéśļłäĻ│Ā, ņČöĻ░ĆņĀüņ£╝ļĪ£ ņŻ╝Ļ┤ĆņĀü ņ”Øņāü(CAS score)ņŚÉ ļö░ļźĖ ņżæņ”ØļÅäļÅä ĒĢ©Ļ╗ś Ļ│ĀļĀżĒĢśņŚ¼ ņĀüņĀłĒĢ£ ļīĆņĪ░ĻĄ░Ļ│╝ ļ╣äĻĄÉĒĢ£ļŗżļ®┤ biasļź╝ ņĄ£ņåīĒĢ£ņ£╝ļĪ£ ņżäņØ┤Ļ│Ā Ēśłņ▓Ł ĒĢŁņ▓┤ņÖĆ ļ¦Øļ¦ē, ļ¦źļØĮļ¦ēĒśłĻ┤Ć Ļ┤ĆĻ│äļź╝ ņĀĢĒÖĢĒ׳ ĒīīņĢģĒĢĀ ņłś ņ׳ņØä Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż.
ļśÉĒĢ£ ļ¦źļØĮļ¦ēļæÉĻ╗ś ļ│ĆĒÖöņŚÉ ļö░ļźĖ Ēśłļźś ļ│ĆĒÖöņŚÉ ļīĆĒĢ£ ņØ┤ņĀäņØś ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņŻ╝ļĪ£ ņŚ╝ņ”ØņŚÉ ņØśĒĢ£ ņÖĖņĢłĻĘ╝ ļ░Å ņĢłņÖĆņĪ░ņ¦üņØś ļČĆņóģņ£╝ļĪ£ ĻĖ░ņØĖĒĢ£ ņĢłĻĄ¼ļé┤ Ēśłļźś ļ│ĆĒÖöļź╝ ņä£ņłĀĒĢśĻ│Ā ņ׳ļŗż. Konuk et al [29]ņØĆ Ļ░æņāüņāśļłłļ│æņ”ØņŚÉņä£ ņÖĖņĢłĻĘ╝ ļ╣äļīĆ, ņĢłņÖĆņ¦Ćļ░® ļ╣äļīĆļĪ£ ļ░£ņāØĒĢśļŖö ņĢłĒøäļČĆ ņĢĢļĀźņØś ļ│ĆĒÖöļŖö ņ£äļłłņĀĢļ¦ź ĒØÉļ”äņØś Ļ░ÉņåīņÖĆ ņĢłņÖĆ ņĀäņ▓┤ņØś ņĀĢļ¦ź ņ£ĀņČ£ņØä Ļ░Éņåīņŗ£Ēé©ļŗżĻ│Ā ļ░ØĒśöļŗż. Jorge et al [30]ņØĆ ņĢłņÖĆ ĒÖśĻ▓ĮņØś ļ¼╝ļ”¼ņĀüņØĖ ļ│ĆĒÖöĻ░Ć ļ¦źļØĮļ¦ē ļ¬©ņäĖĒśłĻ┤ĆņŚÉ ņ¦üņĀæņĀüņØĖ ņśüĒ¢źņØä ļ»Ėņ╣Ā ņłś ņ׳ļŗżĻ│Ā ņĀ£ņŗ£Ē¢łļŗż. Gul et al [31]ņØĆ ņĢłņÖĆ ņĪ░ņ¦ü, ņĢłņÖĆņĀĢļ¦źņØś ņÜĖĒśłņØ┤ Ļ▓░ĻĄŁ ļ¦źļØĮļ¦ēļæÉĻ╗śņØś ņ”ØĻ░ĆļĪ£ ņØ┤ņ¢┤ņ¦äļŗżĻ│Ā ĒĢśņśĆļŗż. Gul et al [31]ņØś Ļ▓░Ļ│╝ļŖö ├¢zkan et al [32]ņØ┤ ĒÖ£ļÅÖĻĖ░ņØś Ļ░æņāüņāśļłłļ│æņ”ØņŚÉņä£ ļ¦źļØĮļ¦ēņØ┤ ņØśļ»Ė ņ׳Ļ▓ī ļæÉĻ║╝ņøīņ¦äļŗżĻ│Ā ļ│┤Ļ│ĀĒĢ£ Ļ▓░Ļ│╝ņÖĆ Ļ░ÖņĢśļŗż. ļśÉ ļŗżļźĖ ņ░ĖĻ│Ā ļģ╝ļ¼ĖņŚÉņä£ļŖö ņĢäņŗ£ņĢäņØĖņØś ņĢłņÖĆļŖö ĒāĆ ņØĖņóģļ│┤ļŗż ņĢłņÖĆļ▓ĮņØ┤ ļæÉĻ╗ŹĻ│Ā ņóüņĢä ņĢłņÖĆĒøäļČĆņØś ļČĆņóģņØś ņ¦üņĀæņĀüņØĖ ņśüĒ¢źņ£╝ļĪ£ CTĻ░Ć Ļ░ÉņåīĒĢĀ ņłś ņ׳ļŗżļŖö ļ│┤Ļ│ĀļÅä ņ׳ņŚłļŗż[33,34]. ĻĘĖļ¤¼ļéś ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ļŖö TSHR AbņØś ļ│ĆĒÖöņŚÉ ļö░ļźĖ CT ļ│ĆĒÖöņŚÉļŖö Ļ▓ĮĒ¢źņä▒ņØ┤ļéś ĒåĄĻ│äņĀü ņ£ĀņØśņä▒ņØĆ ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśļŗż. ņØ┤ļŖö ļ©╝ņĀĆ ĒÖśņ×É ņłśĻ░Ć ņĀüņŚłĻ│Ā ļśÉĒĢ£ Ļ▓ĮĻ│╝ ĻĖ░Ļ░äņØ┤ 1Ļ░£ņøöļĪ£ ņ¦¦ņĢä TSHR AbņØś ļ│ĆĒÖöļ¤ē ņ×Éņ▓┤ļÅä ņĀüņ¢┤ Ļ░ü ļ│ĆņłśņØś ļ│ĆĒÖöļź╝ ļ│┤ļŖöļŹ░ biasĻ░Ć ņāØĻ▓╝ņØä ņłś ņ׳ļŗż. ņČöĒøä ņØĖņøÉņłśļź╝ ļŖśļĀż ņżæņ”ØļÅäņŚÉ ļö░ļźĖ ĻĄ░ņØä ļČäļźśĒĢśĻ│Ā Ļ▓ĮĻ│╝ Ļ┤Ćņ░░ ĻĖ░Ļ░ä RundleŌĆÖs curveņŚÉ ļö░ļØ╝ 6-24Ļ░£ņøöļĪ£ ļŖśļĀż ĻĘĖ ļ│ĆĒÖöļź╝ ĒĢ©Ļ╗ś ļ│Ėļŗżļ®┤ biasļź╝ ņĄ£ņåīļĪ£ ĒĢśņŚ¼ ņŚ░ĻĄ¼ĒĢĀ ņłś ņ׳ņØä Ļ▓āņØ┤ļŗż.
ņĀĆņ×ÉļōżņØ┤ ņĢīĻĖ░ļĪ£ ļ│Ė ņŚ░ĻĄ¼ļŖö ņĄ£ņ┤łļĪ£ Ļ░æņāüņāśļłłļ│æņ”Ø ĒÖśņ×ÉņŚÉņä£ ņŗ£Ļ░äņŚÉ ļö░ļźĖ TSHR AbņÖĆ ļ¦Øļ¦ē, ļ¦źļØĮļ¦ē ļ│ĆĒÖöņØś ņāüĻ┤ĆĻ┤ĆĻ│äņŚÉ ļīĆĒĢ┤ ļŗżļŻ©ņŚłļŗż. ņØ┤ņĀäņØś ļ¦ÄņØĆ ņŚ░ĻĄ¼ļōżņØĆ ņ¦äļŗ©ļÉ£ ņŗ£ņĀÉņŚÉņä£ Ļ░æņāüņāśļłłļ│æņ”ØĻ│╝ ļ¦Øļ¦ēĻ│╝ ļ¦źļØĮļ¦ēņØś ļ»ĖņäĖĒśłĻ┤Ć ļ│ĆĒÖöļź╝ ņĀĢņāüņØĖĻ│╝ ļ╣äĻĄÉĒĢśņśĆĻ│Ā, Ļ░æņāüņāśļłłļ│æņ”ØņØś ļ│æĒā£ņāØļ”¼ĒĢÖņĀü ĒĢ┤ņäØņŚÉ ļö░ļØ╝ ņĢłņÖĆĒśłļźś, ņĢłĻĄ¼ Ļ┤ĆļźśņĢĢņØś ļ│ĆĒÖöņÖĆ ļ¦Øļ¦ē, ļ¦źļØĮļ¦ēņØś ļ│ĆĒÖö Ļ▓░Ļ│╝ļŖö ļŗżņ¢æĒ¢łļŗż[29-32]. ļ│Ė ņŚ░ĻĄ¼ļŖö ņŗ£ļĀź ļ│ĆĒÖöņÖĆ ļ░ĆņĀæĒĢ£ Ļ┤ĆļĀ©ņØ┤ ņ׳ļŖö ļŗ╣ļć©ļ¦Øļ¦ēļ│æņ”Ø, ļéśņØ┤Ļ┤ĆļĀ©ĒÖ®ļ░śļ│Ćņä▒ ļō▒ņØś ļ¦ÄņØĆ ņ¦łĒÖśņŚÉņä£ ņŗ£Ē¢ēĒĢśņśĆļŹś ņ¦ĆĒæ£ļōżņØä ņØ┤ņÜ®ĒĢśņŚ¼ Ļ░æņāüņāśļłłļ│æņ”ØņŚÉņä£ļÅä TSHR AbņØś ļ│ĆĒÖöļ¤ēĻ│╝ ņĀĢĒÖĢĒĢ£ OCTA ņśüņāüņ£╝ļĪ£ ņ¢╗ņØĆ ļ¦Øļ¦ēĻ│╝ ļ¦źļØĮļ¦ē ļ│ĆĒÖöļź╝ ņ¦üņĀæņĀüņ£╝ļĪ£ ļ╣äĻĄÉĒ¢łļŗżļŖö ņĀÉņŚÉņä£ ņØśņØśĻ░Ć ņ׳ļŗż.
ļ│Ė ļģ╝ļ¼ĖņØś ĒĢ£Ļ│äņĀÉņØĆ ĒøäĒ¢źņĀü ņŚ░ĻĄ¼ ļ░®ļ▓Ģņ£╝ļĪ£ ņØśļ¼┤ĻĖ░ļĪØņØä ņé┤ĒÄ┤ļ│┤ņĢśņ£╝ļ®░, ĒÖśņ×É ļ¬©ņ¦æ ĻĖ░Ļ░äņØ┤ ņ¦¦ņĢä ņĪ░ņé¼ ļīĆņāü Ēü¼ĻĖ░Ļ░Ć ņČ®ļČäĒĢśņ¦Ć ļ¬╗Ē¢łĻ│Ā, TSHR AbņØś ļ│ĆĒÖöļ¤ē ņĖĪņĀĢ ĻĖ░Ļ░äņØ┤ 1Ļ░£ņøöļĪ£ ņ¦¦ņĢśņ£╝ļ®░, ņ”ØļÅäņŚÉ ļö░ļźĖ ļČäļźśļź╝ ĒĢśņ¦Ć ļ¬╗ĒĢ£ ņĀÉņØ┤ļŗż. ļśÉĒĢ£ ņĢłņÖĆņĢĢļĀźņØä ļåÆņØ┤Ļ│Ā ņĢłņÖĆņÜĖĒśłņØä ņØ╝ņ£╝Ēé¼ ņłś ņ׳ļŖö ļŗżļźĖ ņØĖņ×Éļōż(ņĢłĻĄ¼ļÅīņČ£, ņÖĖņĢłĻĘ╝ ļČĆĒö╝)ņØä ļ│╝ ņłś ņ׳ļŖö ņĢłņÖĆ ņĀäņé░ĒÖöļŗ©ņĖĄņ┤¼ņśü ļō▒ņØś Ļ│ĀļĀż ņŚåņØ┤ TSHR Ab ņłśņ╣ś ļŗ©ļÅģņ£╝ļĪ£ OCTAņÖĆ ļ╣äĻĄÉĒĢ£ Ļ▓āņØĆ biasĻ░Ć ļÉĀ ņłś ņ׳ļŗż. ĒøäņåŹ ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņ£äņØś ĒĢ£Ļ│äņĀÉņØä ļ│┤ņÖäĒĢśņŚ¼ ĒåĄĻ│äņĀüņ£╝ļĪ£ ņ£ĀņØśĒĢśĻ▓ī ļ░ØĒśĆņ¦ł Ļ┤ĆĻ│äņä▒ņ£╝ļĪ£, Ļ░æņāüņāś ļłłļ│æņ”ØņØś ņżæņ”ØļÅä ļ░Å ņśłĒøä ņśłņĖĪ ļō▒ņØä Ēśłņ▓ŁņØ┤ ņĢäļŗī ļ╣äņ╣©ņŖĄņĀüņØ┤Ļ│Ā ļ╣äĻĄÉņĀü ļäōņØĆ ņŚ░ļĀ╣ļīĆņŚÉļÅä ņēĮĻ▓ī ņ┤¼ņśüņØ┤ Ļ░ĆļŖźĒĢ£ OCTAļź╝ ņØ┤ņÜ®ĒĢ┤ ĒĢĀ ņłś ņ׳ļŗżļŖö ņĀÉņØĆ Ē¢źĒøä ņŚ░ĻĄ¼ņØś Ļ░Ćņן Ēü░ Ļ░ĢņĀÉņØ┤ ļÉĀ Ļ▓āņ£╝ļĪ£ ĻĖ░ļīĆļÉ£ļŗż. Ļ▓░ļĪĀņĀüņ£╝ļĪ£, Ļ░æņāüņāśļłłļ│æņ”Ø ĒÖśņ×ÉņŚÉņä£ OCTA ņØ┤ļ»Ėņ¦Ćļź╝ ņØ┤ņÜ®ĒĢ┤ ļ¦Øļ¦ē, ļ¦źļØĮļ¦ē ļ│ĆĒÖöņÖĆ TSHR Ab ļ│ĆĒÖöņØś ņāüĻ┤ĆĻ┤ĆĻ│äļź╝ ĒīīņĢģĒĢśņśĆņØä ļĢī, 1Ļ░£ņøöĻ░ä TSHR Ab ļ│ĆĒÖöļ¤ēņŚÉ ļö░ļØ╝ ļ¦Øļ¦ēĒśłļźśņÖĆ ļ¦źļØĮļ¦ēļæÉĻ╗ś ļ│ĆĒÖöļ¤ēņŚÉļŖö ņśüĒ¢źņØ┤ ņŚåņŚłņ£╝ļéś 1 mm sCPD ļ│ĆĒÖöņÖĆļŖö ņ¢æņØś Ļ▓ĮĒ¢źņä▒ņØä ļ│┤ņśĆļŗż.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






