

결ě 맼ë˝ë§íę´ëłěŚ(polypoidal choroidal vasculopathy, PCV)ě ěľěą ëě´ę´ë ¨íŠë°ëłěą(age-related macular degeneration, AMD)ě ěíěźëĄ, Yannuzzi et al [1]ě´ 1990ë
ě ěľě´ëĄ ě¸ę¸íěë¤. PCVë ě¸ëěŹě´ěë꡸댰íę´ěĄ°ěě (indocyanine green angiography, ICGA)ěě 결ě -ě ěŹ ëë§ĽëĽ íěĽęłź í¨ęť 맼ë˝ë§ íę´ě ëśě§ëĽź íšě§ěźëĄ íë¤[2-4].
Uyama et al [5]ě PCVě ěě° ę˛˝ęłźě ę´ë ¨íěŹ, 50%ě íěë ěí¸í 경곟뼟 ëł´ě´ë ë°ëŠ´ ëë¨¸ě§ ě ë°ě ěśíęłź ëěś ëąě´ ë°ëłľëě´ íŠë°ëśě ëłěą ë° ěë Ľ ěě¤ëĄ ě´ě´ěĄë¤ęł ëł´ęł íěë¤. PCVěě ěę° ěĽě 뼟 ěźěźí¤ë ě ëë ë¤ěíë, ěźë°ě ěźëĄ wet AMDëł´ë¤ ěë Ľěíę° ë ě˘ě ę˛ěźëĄ ěë ¤ě ¸ ěë¤[5,6].
PCV뼟 ěšëŁí기 ěí í¨ęłźě ě¸ ë°Šë˛ěźëĄ verteporfině ě´ěŠí ę´ěíěë˛(photodynamic therapy, PDT), ííę´ë´íźěąěĽě¸ě(anti-vascular endothelial growth factor, anti-VEGF)ě ě 댏체ę°ë´ 죟ě
, íšě ë ěšëŁě ëłľíŠ ěë˛ ëąě´ ěë¤[7-10]. ę´ěíěë˛ě 결ě ěą ëłëłęłź ěźěśěą ëłíě í´í뼟 ě ëíë ë°ě í¨ęłźě ě¸ ę˛ěźëĄ ëíëŹë¤[11,12]. EVEREST II ě°ęľŹěěë PDTě ranibizumabě ěŹěŠí ëłľíŠ ěë˛ě´ ranibizumabě ë¨ë
ěë˛ëł´ë¤ PCV뼟 ěëĄę˛ ě§ë¨ ë°ě íěë¤ěě ěë Ľě , í´ëśíě ěźëĄ ë ě°ěí í¨ęłźëĽź ěšëŁ ěě 12ę°ě ěě ě ëł´ěë¤ęł ëł´ęł íë¤[9]. ěľęˇźěë AMD ěšëŁëĽź ěí´ ę°ë°ë anti-VEGF ěë˛ě´ PCVě ěźě°¨ ěšëŁëĄ ë§ě´ ěŹěŠëęł ěë¤. ëíě ě¸ anti-VEGF ěšëŁ ë°Šë˛ěźëĄ as-needed regimenęłź treat and extend regimen, fixed dosing regimen ëąě´ ěë¤[13-15]. ěľęˇź PLANET ě°ęľŹěě aflibercept뼟 ě´ěŠí ë¨ë
ěë˛ěźëĄ ě ěí ěë Ľ íĽěě ëł´ěŹěŁźěęł , ěěě íěë§ě´ ěśę°ě PDT ěšëŁę° íěíë¤ęł ëł´ęł íěë¤[10].
ě¤ě ěěěě PCV íěë¤ě ěšëŁ ě´í ë¤ěí 경곟뼟 ëł´ě¸ë¤. ěźëś íěë¤ě ěľěíě ěšëŁë§ěźëĄ ěí¸í 경곟뼟 ëł´ě´ë ë°ëŠ´, ě§ěě ě¸ ěšëŁěë ëśęľŹíęł ěíę° ě ě°¨ ě
íëë íěë¤ë ěë¤. ëłëłě ë°ëłľëë ěŹë°ě ëě ěë Ľěíě ę´ë ¨ ěě ě ěë¤. ë§ě˝ PCV íěě ěšëŁëĽź ěěí기 ě ě 기ě íšěąěźëĄëśí° ěšëŁ 결곟ě ěí뼟 ě츥í ě ěë¤ëŠ´, íěě ěśě ę´ëŚŹ ë° ěšëŁ ë°ŠíĽ ě¤ě ě ëěě´ ë ę˛ě´ë¤. 본 ě°ęľŹě 몊íë ěľěíě ě´ę¸° ěšëŁ í 1ë
ě´ě ěŹë°íě§ ěęł ě°ěí ěë Ľě ě ě§í PCV íěě ěěě íšě§ě 쥰ěŹíë ë° ěë¤.
ëěęłź ë°Šë˛
본 ě°ęľŹë ě˛ěěźëĄ PCV ě§ë¨ě ë°ęł 본ěěě ěšëŁëĽź ěěí ě´í ěľě 1ë
ě´ě ěśě ę´ě°°í íěě ě돴 기ëĄě ë°íěźëĄ ě§íí ííĽě ë§¤ę° ě°ęľŹě´ë¤. 모ë íěë PCVě ëí´ ě˛ě ěšëŁëĽź ë°ę¸° ěěí ě´ë¤ëĄ, ę°í¨ëŚëíęľ ěě¸ěąëިëłěěě ę˛ě§, ěšëŁ ë°ě íěë¤ě ëěěźëĄ ě§íëěë¤. 본 ě°ęľŹë ëłěě ě¤ëŚŹ ěěíě ěšě¸ě ë°ěęł Helsinki ě ě¸ě ěęą°íěŹ ě§íëěěźëŠ° 본ě ěěě°ęľŹěŹěŹěěí(Institutional Review Board, IRB)ě ěšě¸íě ě§íëěë¤(ěšě¸ ë˛í¸: KC19RASI0898).
PCVě ě§ë¨ě ICGAę˛ěŹëĽź ě´ěŠíěŹ ëśě§íę´ë§ ě 돴ě íšě§ě ě¸ ę˛°ě ěą íę´ ëłëłě 쥴ěŹě ěí´ ě´ëŁ¨ě´ěĄë¤. ë¤ěě ě ě¸ ę¸°ě¤ě´ ě ěŠëěë¤: 1) ěľě´ ę˛ěŹěě ě¤ěŹě 욨ë˛íë ě§ëí ěěś ëë ěíě íí°ę° ěë 경ě°, 2) ěë Ľě ěíĽě ě¤ ě ěë ë¤ëĽ¸ ěęłźě ě§í(ěŚěëšë¨ë§ë§ëł ëë ë§ë§ě¤ěŹě 맼íě ëą), 3) ěśě ę´ě°° ę¸°ę° ě¤ í늴ëśě 댏체ě ě ě ě ë°ě íě, 4) 기í 맼ë˝ë§ë§ě§íěźëĄ ě 댏체ë§ë§ěě ë° ěęľŹë´ ěŁźěŹěšëŁ, ę´ěęł ëë ę´ěíěë˛ě ë°ěë íě. ë§ë§í ěśíě ę°ě§ íěě 경ě°ěë íŠë°í ěśíě íŹę¸°ę° 2 ě ëě§ę˛˝ 늴ě ě´ěěźëĄ ě 댏체ę°ë´ ę°ě¤ěŁźě
ě ęłź ę°ě ě˛ěšëĽź ěí ë°ě ě´ë¤ ěě ě ě¸ëěë¤.
모ë íěë íŹę´ě ěęłź ę˛ěŹëĽź ë°ěěźëŠ°, ě´ěë ě¤ëŹë ěë Ľí뼟 ě´ěŠí ěľëęľě ěë Ľ(best-corrected visual acuity, BCVA)ę˛ěŹ, ě¸ęˇšëąí미경ę˛ěŹ, ě°ë í ěě ę˛ěŹ, ěě ě´Źě, ęłľě´ě 죟ěŹë ě´ě ę˛ě경ę˛ěŹëĽź ě´ěŠí íę´ěě íę´ěĄ°ěě ęłź ICGA (Heidelberg Retina Angiograph [HRA]; Heidelberg Engineering Co., Heidelberg, Germany) ëąě´ 기본 ę˛ěŹëĄ íŹí¨ëěë¤. ëšę°ěë¨ě¸ľě´Źě(optical coherence tomography, OCT) ěěě ě¤íí¸ëź ěě OCTëĄ ě´Źěëěë¤(Spectralis OCT+HRA; Heidelberg Engineering, Heidelberg, Germany).
ěľëëłëłě§ę˛˝(greatest linear dimension, GLD)ě Heidelberg Eye Explorer ěíí¸ě¨ě´(v.6.0.9.0; Heidelberg Engineering)뼟 ěŹěŠíěŹ ICGA ěěěě ěę¸°ëĄ ě¸Ąě íěęł , 결ě ě ě ëí ICGA ěěěě íě
íěë¤. ICGAě ě§ě°ę¸°ěě ë¤ě´ě ęłźíę´ ěěě íě
í¨ěźëĄě¨ 맼ë˝ë§íę´ ęłźíŹęłź(choroidal vascular hyperpermeability)뼟 íě¸íěë¤. íŠë°ëśëĽź 욨ë˛íë ë§ë§ë´ěĄ(intraretinal fluid), ë§ë§íěĄ(subretinal fluid), ë§ë§ěěěíźë°ëŚŹ(pigmented epithelial detachment, PED)ë OCT ěěě íľí´ íě¸íěë¤. ě¤ěŹěí 맼ë˝ë§ëęť(subfoveal choroidal thickness)ë ë§ë§ěěěíź ě¸ě¸Ąěěëśí° ë´ě¸Ą ęłľë§ ę˛˝ęłě ęšě§ě ěě§ ęą°ëŚŹëĽź ě¤ěŹěěě 츥ě íěë¤.
íěë¤ě ë´ëš ěěŹě íë¨ě ë°ëź, anti-VEGF ë¨ë
ěë˛ ëë PDTě anti-VEGFě ëłľíŠ ěë˛ ě¤ í ę°ě§ ěšëŁ ë°Šë˛ě ě´ę¸° ěšëŁëĄ ěí ë°ěë¤. ëëśëśě íěë¤ě anti-VEGF ë¨ë
ěë˛ě ěźě°¨ ěšëŁëĄ ěí ë°ěęł , 결ě ęłź ëśě§ íę´ë§ěě ëěśě´ ěë 경ě°ě´ęą°ë PEDě ę´ë ¨ë ę´ë˛ěí ë§ë§íěĄ ëë ěźěśě ëł´ě´ë ę˛˝ě° ëąěë ëłľíŠ ěë˛ě ěźě°¨ ěšëŁëĄ ęł ë ¤íěë¤. Anti-VEGF ěë˛ě ě´ę¸° ěšëŁëĄ ë°ě íěë¤ěę˛ë ranibizumab (Lucentis; Genentech Inc., South San Francisco, CA, USA) ëë aflibercept (Eylea; Bayer HealthCare, Berlin, Germany) ě 댏체ę°ë´ 죟ě
ě ě í ëŹ ę°ę˛ŠěźëĄ 3í 죟ěŹíěë¤. PDTě anti-VEGF ëłľíŠ ěë˛ě 경ě°ë 첍 ë˛ě§¸ ě 댏체ę°ë´ anti-VEGF 죟ěŹëĽź ěííęł 3-4ěź ě´íě PDT ěšëŁëĽź ěííěěźëŠ° ěŁźěŹ ě˝ëŹźě bevacizumab (Avastin; Genentech Inc.)ě ěŹěŠíěë¤. PDTë Treatment of Age-Related Macular Degeneration with Photodynamic Therapy Studyě ëŞ
ěë ë°Šë˛ěźëĄ ěííěë¤[16].
ě´ę¸° ěšëŁ í íěë¤ě 매 1-2ę°ěë§ë¤ 경곟 ę´ě°°í늴ě íě ě anti-VEGF뼟 ěśę°ëĄ 죟ěŹíěëë°, OCTěě ě¤ěŹě뼟 욨ë˛íęą°ë ěííë ë§ë§íěĄ/ë§ë§ë´ěĄě´ ë°ěí ę˛˝ě° íšě ěě ę˛ěŹěě ěëĄě´ ë§ë§/ë§ë§í ěśíě´ ë°ěí 경ě°ëĽź ě§íě íëěąě´ ěŹë°í ę˛ěźëĄ íë¨íęł ěśę° 죟ěŹëĽź ěííěë¤. ěŹë°íě§ ěě íěě 경ě°ěë ěśę° ěšëŁ ěě´ ë´ëš ěěŹě íë¨ě ë°ëź 경곟 ę´ě°° ę°ę˛Šě ě°ěĽíěë¤.
경곟 ę´ě°° ę¸°ę° ě¤ 1) ě´ę¸° ěšëŁ ě´íě ë§ë§íěĄ/ë§ë§ë´ěĄě´ ěě í ěě¤ë ěíëĄ 1ë
ě´ ëë ę¸°ę° ëě ě§í íëěąě ěŹë° ě겏ě ëł´ě´ě§ ěęł , 2) ěśę°ě ě¸ ěŁźěŹ ěšëŁëĽź ë°ě§ ěěěźëŠ°, 3) ë§ě§ë§ 경곟 ę´ě°° ěě ě¤ëŹë ěë Ľ 20/30 ě´ěě ě°ěí ěë Ľě ëł´ě¸ íěë¤ě âëšěŹë°ęľ°âěźëĄ ëśëĽíěęł , ěě ě¸ ę°ě§ ěŹí ě¤ í ę°ě§ëźë í´ëšëě§ ěë íěë¤ě âëšěŹë°ęľ°âě íŹí¨ěí¤ě§ ěěë¤. ë°ëŠ´, ě´ę¸° ěšëŁ ě´í ěě ę´í´ ěŹëśě ěę´ěě´ ę˛˝ęłź ę´ě°° ě¤ ě§í íëěąě ěŹë°ëĄ ěśę°ě ě¸ ěšëŁëĽź ë°ě íěë¤ě âěŹë°ęľ°âěźëĄ ëśëĽíěë¤.
ëšěŹë°ęľ°ęłź ěŹë°ęľ°, ë ꡸룚 ę°ě 기ě íšěą ë° OCT, ICGAě ꡟ깰í í´ëśí ě겏ě ě°¨ě´ëĽź ëšęľíěë¤. ëí ěšëŁ ë°Šë˛ě ë°ëź anti-VEGF ë¨ë
ěŁźěŹ ěšëŁë§ ěí ë°ě íěë¤ ë´ěěě ëšěŹë°ęľ°ęłź ěŹë°ęľ°, ęˇ¸ëŚŹęł ëłľíŠ ěë˛ě ěí ë°ě íěë¤ ë´ěěě ëšěŹë°ęľ°ęłź ěŹë°ęľ° ę°ě ě°¨ě´ ěě ę°ę° ëśěě ěííěë¤. íľęł ëśěě ěí´ BCVA ę°ě logarithm of the minimal angle of resolution (logMAR)ěźëĄ ëłííěë¤. ěëě°ěŠ SPSS ë˛ě 19.0뼟 ěŹěŠíěŹ íľęł ëśěě ěííë¤(SPSS Inc., Chicago, IL, USA). ě°ě ëłě ëšęľëĽź ěí´ studentâs t-test뼟 ěŹěŠíěęł , chi-square ę˛ě ě ěŹěŠíěŹ ë˛ěŁźí ëłě뼟 ëšęľíěěźëŠ°, ë¨ëłë ëśěěě ě ěí ě¸ěë¤ě ëěěźëĄ ëĄě§ě¤íą íęˇëśěě ěśę°ëĄ ěííěë¤. p-valueę° 0.05 미ë§ě¸ ę˛˝ě° íľęłě ěźëĄ ě ěíë¤ęł í´ěíěë¤.
결 곟
본 ě°ęľŹë 101ëŞ
íěě ë 101ěě ëśěíěë¤. Table 1ě anti-VEGF ë¨ë
ěë˛ ëë PDTě anti-VEGF ëłľíŠ ěë˛ ěšëŁëĽź ë°ě 모ë PCV íěë¤ě 기ě íšě§ě ëł´ěŹěŁźęł ěë¤. íęˇ ě°ë šě 63.83 Âą 8.79ě¸ěęł ě¤ěŹěí 맼ë˝ë§ëęťë 286.11 Âą 104.45 Âľm, íŠë°ëśëĽź 욨ë˛íë ë§ë§íěĄ, ë§ë§ë´ěĄ, ěěěíźë°ëŚŹě ěĄ´ěŹ ëšě¨ě ę°ę° 94.1%, 12.9%, 32.7%ěë¤. ěľëëłëłě§ę˛˝ě íŹę¸°ë 3,041.22 Âą 1,178.73 Âľm ěęł ę˛°ě ě ěë 1.47 Âą 0.85ę°ěë¤. 59ěě anti-VEGF ë¨ë
ěë˛ě ěí ë°ěęł 42ěě ëłľíŠ ěë˛ě ěí ë°ěë¤. 모ë ëěěě íęˇ ěśě ę´ě°° 기ę°ě 59.32 Âą 32.75ę°ěě´ěë¤.
47ěě´ ě´ę¸° ěšëŁ í 경곟 ę´ě°° ě¤ě 1ë
ě´ě ěŹë° ěě´ ě˘ě ěë Ľě ě ě§íë ěí¸í 경곟뼟 ëł´ěęł (ëšěŹë°ęľ°), 54ěě ě§ěě ě¸ ëłëłě ěŹíěąíëĄ anti-VEGF ěŁźěŹ ëë PDT뼟 ěśę° ěšëŁëĄ ěí ë°ěë¤(ěŹë°ęľ°). ěŹë°ęľ°ě ę˛˝ě° 65.57 Âą 35.29ę°ěě ěśě ę´ě°° ę¸°ę° ëě ěśę° ěšëŁëĄ 모ë ěěě ěľě 5í ě´ěě anti-VEGF ěŁźěŹ ěšëŁę° ěíëěěźëŠ° íęˇ ěŁźěŹ íěë 21.22 Âą 12.73íěë¤. 5ěěěë PDT 1í, 2ěěěë PDT 2íę° ěśę°ëĄ ěíëěë¤.
ëšěŹë°ęľ°ęłź ěŹë°ęľ°, ë ꡸룚 ę°ě ě°¨ě´ě ě Table 2ě ě ěëě´ ěë¤. ëšěŹë°ęľ°ě íŹí¨ë íěë¤ ě¤ 29ěě anti-VEGF ë¨ë
ěë˛ě, 18ěě ëłľíŠ ěë˛ě ě´ę¸° ěšëŁëĄ ěíë°ěęł , ěŹë°ęľ°ě íŹí¨ë íěë¤ ě¤ 30ěě anti-VEGF ë¨ë
ěë˛ě, 24ěě ëłľíŠ ěë˛ě ěí ë°ěěźëŠ°, ë ꡸룚 ę° ě´ę¸° ěšëŁ ë°Šë˛ě íľęłě ěźëĄ ě ěí ě°¨ě´ëĽź ëł´ě´ě§ ěěë¤(p=0.551). ë ꡸룚 ę° ëě´, ěąëł, ę¸°ě¤ ěë Ľ ěě ě ěí ě°¨ě´ë ěěęł , ěľě˘
ěë Ľ(logMAR)ě ëšěŹë°ęľ°ěě ë ě˘ěë¤(0.07 Âą 0.06 vs 0.44 Âą 0.31, p<0.001). OCT 결곟ěě ěŹë°ęľ°ě´ ëšěŹë°ęľ°ëł´ë¤ ěěěíźë°ëŚŹě ěĄ´ěŹ ëšě¨ě´ ëę˛ ëíëŹęł (p=0.003), ICGA 결곟ěě ëšěŹë°ęľ°ě ěľëëłëłě§ę˛˝ íŹę¸°ę° ë ěěěźëŠ°(p<0.001) 결ě ě ěë ěŹë°ęľ°ëł´ë¤ ě ę˛ ëíëŹë¤(p<0.001). ë§ë§íěĄ, ë§ë§ë´ěĄ, ě¤ěŹěí 맼ë˝ë§ëęť, 맼ë˝ë§íę´ ęłźíŹęłźë ë ꡸룚 ę° ě ěí ě°¨ě´ëĽź ëł´ě´ě§ ěěë¤. íęˇëśě 결곟ěě ěě ěľëëłëłě§ę˛˝(p=0.002), ě ě ěě 결ě (p=0.013), ęˇ¸ëŚŹęł ěěěíźë°ëŚŹě ëśěŹ(p=0.025)ę° ě˘ě ěíě ę´ë ¨ ěěě´ íě¸ëěë¤.
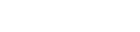
Anti-VEGF ë¨ë
ěë˛ë§ ë°ě íěěěě ëšěŹë°ęľ° ë° ěŹë°ęľ°ě 기ě íšěąě ëśěíěŹ Table 3ě ě ěíěë¤. ëšěŹë°ęľ°ě ěŹë°ęľ°ě ëší´ ěěěíźë°ëŚŹě ěĄ´ěŹ ëšě¨ě´ íľęłě ěźëĄ ě ěíę˛ ëŽěęł (p=0.049) ěľëëłëłě§ę˛˝ íŹę¸°ę° ěěęł (p=0.002) 결ě ě ěę° ě ěë¤(p=0.005). íęˇëśě 결곟ěě ěě ěľëëłëłě§ę˛˝(p=0.030), ě ě ěě 결ě (p=0.017), ęˇ¸ëŚŹęł ěěěíźë°ëŚŹě ëśěŹ (p=0.044)ę° ě˘ě ěíě ę´ë ¨ ěěě´ íě¸ëěë¤. ëí ěŹëĄę° Fig. 1ě ě ěëě´ ěë¤.
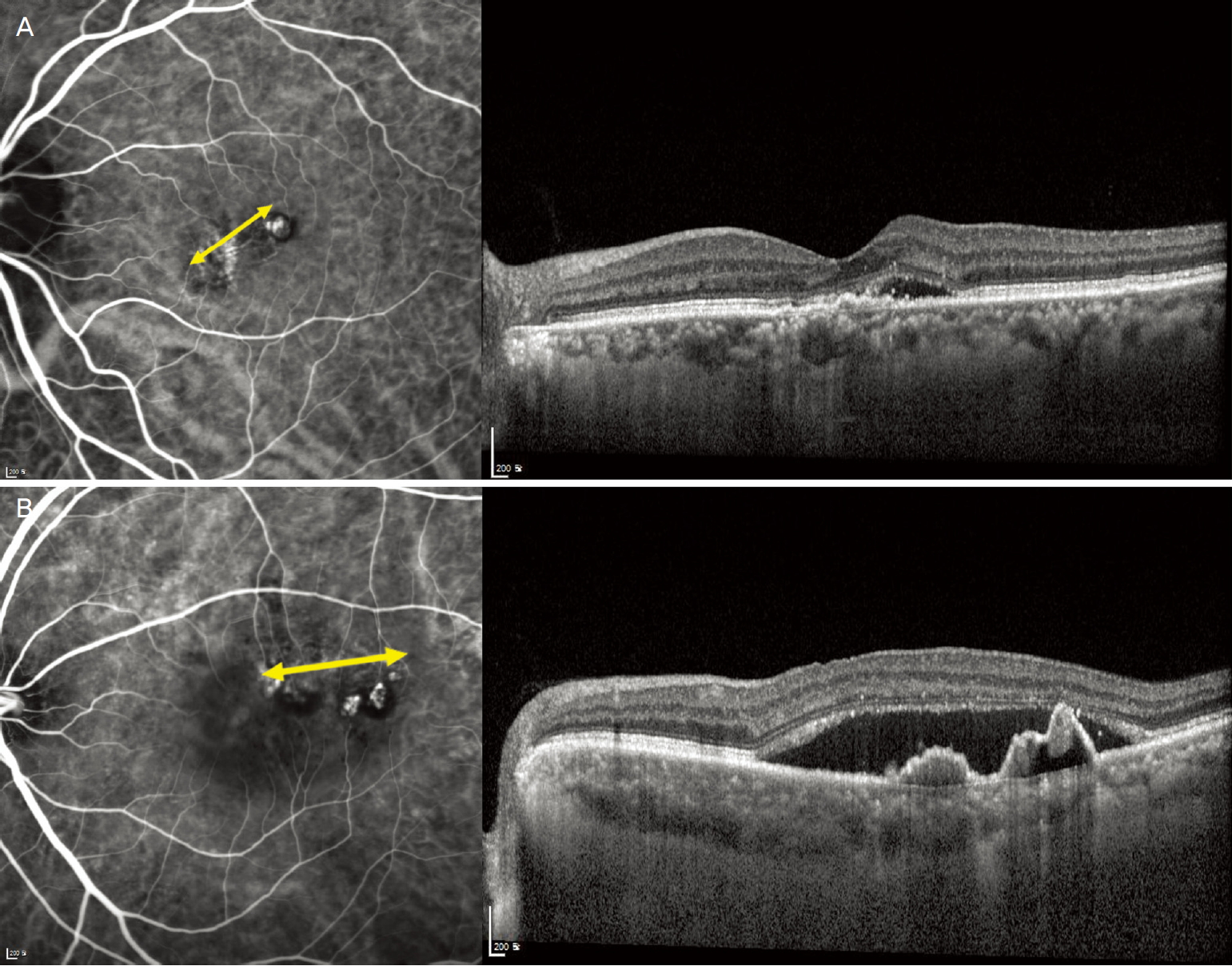
ëłľíŠ ěë˛ě ěí ë°ě íěěěě ëšěŹë°ęľ° ë° ěŹë°ęľ°ě 기ě íšěąě ëśěíěŹ Table 4ě ě ěíěë¤. OCT 결곟 ě¤, ěěěíźë°ëŚŹě ěĄ´ěŹ ěŹëśë§ě´ ë ꡸룚 ę° íľęłě ěźëĄ ě ěí ě°¨ě´ëĽź ëł´ěë¤(p=0.014). ICGA ě겏 ě¤ěě ěľëëłëłě§ę˛˝ íŹę¸°(p<0.001)ě 결ě ě ě(p=0.012)ę° ë ꡸룚 ę° ě ěí ě°¨ě´ëĽź ëł´ěë¤. íęˇëśě 결곟, ěľëëłëłě§ę˛˝ íŹę¸°(p=0.006)ë§ě´ ěšëŁ í ě˘ě ěíěě ę´ë ¨ěąě ëł´ěë¤. ëí ěŹëĄę° Fig. 2ě ě ěëě´ ěë¤.
ęł ě°°
ě´ě ě ę°íë PCVě ěšëŁ 결곟 ë° ěíě ëí ěŹëŹ ë
źëŹ¸ë¤ě íľí´ ěľëëłëłě§ę˛˝[17-20], 결ě ě ęľ°ě§í[17,20,21], 맼ë˝ë§íę´íŹęłźěą[22,23], 맼ë˝ë§ëęť[24,25], ë§ë§íěĄě ě 돴[22] ë° ěěěíźë°ëŚŹě ě 돴[18,26-28ę°] ěíě ę´ë ¨ë ě¤ěí ěě¸ě´ëź ěë ¤ě ¸ ěë¤. ě¤ě ěěěě ë§ě PCV íěë¤ě ëłëłě ěŹíěąí ëë ě
íëĄ ě§ěě ě¸ ěšëŁëĽź íěëĄ íë¤. ꡸ëŹë PCV íěë¤ ě¤ ěźëśěěë ě´ę¸° ěšëŁě ě ë°ěí ě´í ěŹë°ě´ë ěśę° ěšëŁ ěě´ ě°ěí ěë Ľě ě ě§í늰 ě¤ë ę¸°ę° ëě ě˘ě í´ëśíě ěí뼟 ě ě§íë 경ě°ë ěë¤. PCV íěë¤ě ë¤ěí 기ě íšěąë¤ ě¤ěě ěšëŁ í ěí¸í 결곟뼟 ě츥í ě ěë íšě í ě¸ěę° ěë¤ëŠ´ ěšëŁ ë°ŠíĽ ě¤ě ë° ěí ě츥ě ëěě´ ë ę˛ě´ëŠ°, ě´ ě¸ěë¤ě íě
íë ę˛ě´ 본 ě°ęľŹě 몊ě ě´ěë¤.
2010ë
ě Okubo et al [29]ě ě¤ë ę¸°ę° ěšëŁ ěě´ ěě ě ě¸ ěí뼟 ëł´ě´ëŠ° ě˛ě˛í ě§ííë PCV ěŹëĄë¤ě ěěą ę˛˝ęłźëĄ ëł´ęł íë¤. ě°ëŚŹ ě°ęľŹěěë ěľěíě ě´ę¸° ěšëŁ í ěľě 1ë
ě´ě ěŹë°ě´ ěęł ěśę° ěšëŁëĽź ë°ě§ ěěźëŠ°, ě°ěí ěë Ľě ě ě§íë 경ě°ëĽź ěěą ę˛˝ęłźëĄ ě ěíěë¤. ěľěíě ě´ę¸° ěšëŁëź í¨ě anti-VEGF ë¨ë
ěë˛ěěë ě´ę¸° 1ëŹ ę°ę˛Š 3ě°¨ëĄě 죟ěŹ, ęˇ¸ëŚŹęł ëłľíŠ ěë˛ě 경ě°ěë anti-VEGF ěŁźěŹ ěšëŁ 1íě PDT 1íëĄ ě ěíěěźëŠ°, ě°ěí ěë Ľě´ë 20/30 ě´ěě ě¤ëŹë ěë ĽěźëĄ ě ěíěë¤.
본 ě°ęľŹ 결곟ě ë°ëĽ´ëŠ´, 기ě íšěąěě ěľëëłëłě§ę˛˝ě íŹę¸°ę° ěęł ę˛°ě ě ěę° ě ěźëŠ° ěěěíźë°ëŚŹę° ěě ë ěí¸í 경곟뼟 ëł´ěěźëŠ°, ě´ëŹí 결곟ë anti-VEGF ë¨ë
ěë˛ ëë PDT ëłľíŠ ěë˛ ëąě ěšëŁ ë°Šë˛ęłź ěę´ěě´ ëěźíę˛ ëíëŹë¤. ë¤ëĽ¸ ěŹëŹ ë
źëŹ¸ěě ěľëëłëłě§ę˛˝ íŹę¸°ě ěë Ľ ë° ěšëŁ ěíě ěę´ěąě ëí´ ëł´ęł í ë° ěë¤. 2011ë
ě Tsujikawa et al [30]ě PCV íěěě ëłëł íŹę¸°ę° ěě ëëśëśě ę˛˝ě° ě´ę¸° ěë Ľě´ ě˘ěěźëŠ° 경곟 ę´ě°° ę¸°ę° ëě ě°ěí ěë Ľě ě ě§íë¤ęł ëł´ęł íë¤. ěľęˇź Kim et al [17]ě ranibizumab ěŁźěŹ ěšëŁëĽź ë°ě íěë¤ě ëśěí 결곟, í° ěľë ëłëłě§ę˛˝ě´ ěšëŁ í 1ë
ě´ë´ě ëłëłě´ ěŹë°íë ěí ěě¸ ě¤ íëěě ë°íëë¤.
본 ě°ęľŹě ëśě 결곟ěěë ěě ěľëëłëłě§ę˛˝ě´ ěě PCV íěë¤ě ě´ę¸° ěšëŁ í 1ë
ě´ ëë ěśě ę¸°ę° ëě ěŹë° ěě´ ěě ě ěźëĄ ě ě§ëë ěí¸í 경곟뼟 ëł´ěë¤. ë°ëźě ě´ě ě ěë ¤ě§ ë°ě ę°ě´ PCVěě ěľëëłëłě§ę˛˝ě ěë Ľ ěí ë° ěšëŁ 결곟ě ěę´ěąě´ ëě ěě¸ě´ëźë ę˛ě´ íě¸ëěë¤.
íŹëěĄě´ě˛ëź 결ě ě´ ęľ°ě§ě íěąíë ę˛˝ě° ěíę° ě˘ě§ ěë¤ë ěŹě¤ ěě ěľí ěë ¤ě ¸ ěęł , ě´ëŹí ëłëłë¤ě ëě íěąě ë늰 ěśí, ëěśě´ ě ěźě´ëęł ěŹę°í ěë Ľ ěěě ě ë°íë¤[5,31]. 2013ë
ě Hikichi et al [20]ě ranibizumaběźëĄ ěšëŁ ë°ě PCV íěë¤ě ëśěíěŹ, íŹëěĄě´ě ę°ě ęľ°ě§ě ě´ëŁ¨ë 결ě ëłëłě´ ěë 경ě°ě ěľě´ ranibizumab ěŁźěŹ 1ë
íě ěë Ľě´ ě°ěíë¤ë ěŹě¤ě ë°ííěë¤. Lee et al [32]ě 2012ë
ě íŹëěĄě´ íěźëĄ ęľ°ě§ě ě´ëŁ¨ë 결ě ě PCVë PDT ěšëŁ í ěźěśě´ ě§ěëęą°ë ěŹë°íë ëą ěě ë°ěě´ ě˘ě§ ěë¤ë 결곟뼟 ë°ííěęł , 2016ë
ěë íŹëěĄě´í 결ě ě PCV ëłëłě´ ę°ě§ęł ěë ě ě íę´ ě ë°ě íšě§ěźëĄ ě¸í´ ěźë°ě ě¸ PCVëł´ë¤ ë ě죟 죟ěŹëĽź ë§ěěź íë¤ęł ëł´ęł íë¤[21].
íŹëěĄě´í 결ě ęľ°ě§ě 경곟 ę´ě°° ę¸°ę° ě¤ ěŹíěąí ěíě´ ëęł ěšëŁ ę˛°ęłźę° ě˘ě§ ěěźëŠ° 곾겊ě ě¸ ěšëŁëĽź ěíë¤. ë°ëźě PCV ě¤ěě 결ě ě ěę° ě ě ę˛˝ě° ě´ę¸° ěšëŁě ë°ěě´ ë ě˘ěźëŠ° ěĽę¸°ę° ěŹë°ě´ ěë ě°ěí ěí뼟 ëł´ě¸ë¤ęł í ě ěë¤.
ěěěíźë°ëŚŹë PCVě ěěě íšě§ ě¤ íëě´ëŠ°, ě´ ě겏ě anti-VEGF ěë˛ě ě ë°ěíě§ ěë 경íĽě´ ěë¤[33]. ě´ě ě ě°ęľŹë¤ě íľí´ PCV íěěě ěěěíźë°ëŚŹě 쥴ěŹě ěë Ľ ěíě ěę´ěąě ëí´ěë ěźę´ë ę˛°ëĄ ě´ ëěśëě§ ěěë¤.
2008ë
ě Saito et al [28]ě ěěěíźë°ëŚŹę° 쥴ěŹíë PCV íěě 쥴ěŹíě§ ěë íě ę°ě PDT ěšëŁ ě´í ěë Ľě ëšęľíěęł ě ěí ě°¨ě´ę° ěë¤ęł ëł´ęł íë¤. ë°ëŠ´, ěľęˇź ěźëś ě°ęľŹěěë PCV íěěě ěěěíźë°ëŚŹę° ěě ě ěë Ľ ěíę° ë ě˘ë¤ë ę˛°ęłźę° ëł´ęł ëěë¤. Kang and Koh [18]ë 기ě ě ěěěíźë°ëŚŹę° ěë ę˛˝ě° ranibizumab ěŁźěŹ í ěĽę¸° ěë Ľě´ ě°ěíę˛ ě ě§ëë ę˛ęłź ëě ěę´ěąě ëł´ě¸ë¤ęł ëł´ęł íěë¤. ěľęˇź Mori et al [26]ě ranibizumab ěšëŁ 결곟뼟 ëśěíěëë°, 기ě ěěě ěěěíźë°ëŚŹě ě ëŹ´ę° ę˛˝ęłź ę´ě°° ę¸°ę° ě¤ ěŹěšëŁě íě ěŹëśëĽź ě츥íë ěě¸ě´ ëë¤ęł ëł´ęł íë¤.
본 ě°ęľŹěěë 기ě ě ěěěíźë°ëŚŹę° ěë ę˛˝ě° ě´ę¸° ěšëŁ í ě˘ě í´ëśíě 결곟뼟 ëł´ěěźëŠ°, ě´ë anti-VEGF ěŁźěŹ ë¨ěź ěë˛ ěšëŁëĽź ë°ě íěě PDT ëłľíŠ ěšëŁëĽź ë°ě íě ę°ę°ěě ëěźí ę˛°ęłźę° ëíëŹë¤. ëšëĄ ęłźęą°ě ë
źëŹ¸ë¤ě´ ěëĄ ě윊ëë 결곟뼟 ě ěí기ë íěźë, ěěěíźë°ëŚŹě ěĄ´ěŹ ěŹëśë ěšëŁ ěíě 결ě ěě¸ ě¤ íëëĄ ěę°ëë¤. ë°ëźě 기ě ěě ěěěíźë°ëŚŹę° ěë ę˛˝ě° ě´ę¸° ěšëŁ í ěĽę¸°ę° ěśę° ěšëŁę° íě ěë ě°ěí ěí뼟 기ëí ě ěë¤.
본 ě°ęľŹë ëŞ ę°ě§ ě íě ě´ ěë¤. 첍째, 돴ěě ě ě ě íě§ ěęł ěěě íě뼟 ě ě í ííĽě ě°ęľŹëĄ ě§ííě기 ë돸ě ě í í¸íĽě´ ë°ěí ě ěë¤. ë째, 본 ě°ęľŹ 결곟ë ëšěŹë°ęľ°ęłź ěŹë°ęľ° ę°ě íšě§ě ěëě ěźëĄ ëšęľí ę˛ěźëĄ, ě ëě íě¤ ę¸°ě¤ě ě ěíě§ ěěë¤. ě
째, ěľëëłëłě§ę˛˝, 결ě ě ě, ěěěíźë°ëŚŹ ě 돴 ëą ě´ě ě ěë ¤ě§ ě¸ě ě´ě¸ě ěëĄě´ ěě¸ě´ ë°ę˛Źëě§ë ěěë¤. ꡸ëŹë 본 ě°ęľŹě ëěě´ ë íěë¤ě ěśě ę´ě°° ę¸°ę° ě¤ ë´ëš ěěŹě ëłę˛˝ ěě´ ëěźí ě 돸ěěę˛ ě´ę¸° ě§ë¨ëśí° ěšëŁęšě§ ěí ë°ě기 ë돸ě, ę° íěë§ë¤ ěśě ę¸°ę° ě¤ ěšëŁ ë°Šë˛ ę˛°ě ě 기ě¤ě´ ëěźíę˛ ě ěŠëěë¤ęł ëłź ě ěë¤. ëí, anti-VEGF ěŁźěŹ ë¨ěź ěë˛ íšě PDT ëłľíŠ ěë˛ě ěšëŁ ë°Šë˛ě ę´ęłěě´ ěí¸í 결곟ě ę´ë ¨ë ě¸ěë¤ě´ ëěźíë¤ęł ë°íěĄë¤ë ë°ě 본 ě°ęľŹě ë ë¤ëĽ¸ ěěę° ěë¤ęł ěę°ëë¤. 본 ě°ęľŹěě PCVě ěí¸í 경곟ë ě˘ě í´ëśíě ěí(dry macula)ě 기ëĽě ěźëĄ ě°ěí ěë Ľ(ě¤ëŹë ěë Ľ 20/30 ě´ě) ě ě§ ëŞ¨ë뼟 ęł ë ¤íěŹ ě ěíěěźëŠ°, ë°ëźě ë¤ëĽ¸ ě°ęľŹě ëšęľí´ ëšěŹë°ęľ° ě ě 기ě¤ě´ ë ě겊íë¤ë ě ëí 본 ě°ęľŹę° ę°ě§ë ę°ě ě´ëźęł ëłź ě ěë¤.
ę˛°ëĄ ě ěźëĄ, PCV ěšëŁě ěě´ě anti-VEGF ěŁźěŹ ë¨ěź ěë˛ě´ë PDT ëłľíŠ ěë˛ ëąě ěšëŁ ë°Šë˛ě ë§ëĄ íęł , ěě ěľëëłëłě§ę˛˝, ě ě ěě 결ě , ěěěíźë°ëŚŹě ëśěŹě ę°ě 기ě íšěąě´ ě´ę¸° ěšëŁ í ě¤ë ę¸°ę° ěŹë°ě´ ěěźëŠ° ě°ěí ěë Ľě´ ě ě§ëë ěí¸í 경곟ě ě°ę´ë ě¸ěëźë ę˛ě´ íě¸ëěë¤. ě¤ě ěěěě ěšëŁ ěě ě ě 기ě ěě ě´ě ę°ě íšěąě íě
íë ę˛ě´ íěě ěšëŁ 결곟 ě츥 ë° ěśě ę´ě°° ę¸°ę° ëě ěšëŁ ë°ŠíĽ ě¤ě ě ëěě´ ë ę˛ěźëĄ ěę°ëë¤.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






