갑상샘눈병증은 만성적인 자가면역 질환인 그레이브스병 환자에서 가장 흔하게 발생하는 합병증이다.
1 명확한 기전이 밝혀지지 않았으나 갑상샘 항원의 세포 매개 면역 반응으로 인해 안와 결체조직의 염증을 유발하는 것으로 알려져 있으며2 제한된 안와 내부의 다양한 구조물을 침범하여 안구돌출, 눈꺼풀뒤당김, 외안근 비대, 복시, 압박시신경병증 등을 유발한다.
3,4
갑상샘눈병증 환자의 치료는 활동기에서는 고용량 부신피질호르몬제, 면역억제제 등을 우선 고려하게 되며 비활동기에서 6개월 이상 안구돌출을 포함한 안과적 증상이 지속될 경우 안와감압술을 시행할 수 있다.
5,6
내시경적 안와감압술은 1990년 처음 소개된 이후7 흉터가 남지 않으며, 안와첨부의 시야 확보가 용이하다는 점에서 널리 사용되고 있다.
8 현재 갑상샘눈병증 환자에서 안와감압술 후 안구돌출의 교정 정도를 예측하기 위한 정확한 지표는 없으며 이를 예측하기 위한 다양한 지표에 대한 연구가 진행되었다.
9 안와 길이, 안구 길이, 안와 길이와 안구 길이의 비, 안와첨부 각도, 사골동 깊이, 코중격 치우침 등이 안와감압술 후 안구돌출 교정 정도를 예측하기 위한 지표로 제시되었다.
10-12 또한 이전 연구에서 안와 구조 형태를 대표하는 안와 길이, 안구 길이, 안와첨부 각도 등의 지표들에 대해 3차원 얼굴 전산화단층촬영 결과와 2차원 얼굴 전산화단층촬영 결과를 비교했을 때 유의한 상관성을 보여주었다.
10
이에 본 연구에서는 2차원 얼굴 전산화단층촬영 결과를 바탕으로 내시경적 단독 안와내벽감압술을 시행한 갑상샘눈병증 환자에서 수술 전후 안와 구조와 안구돌출 변화의 관계에 대해 알아보고자 한다.
대상과 방법
2017년 2월부터 2021년 3월까지 본 병원 안과에서 갑상샘눈병증을 진단받고 내시경적 단독 안와내벽감압술 시행 후 6개월 이상 추적 관찰된 18명(33안)의 환자를 대상으로 의무기록을 후향적으로 분석하였으며 이전 안와감압술, 외안근수술, 안와골절, 방사선 치료, 안구손상(안구파열 등)이 있는 환자는 대상에서 제외하였다. 본 연구는 헬싱키선언을 준수하였고 본원 임상시험윤리위원회(Institutional Review Board, IRB)의 승인을 받았다(승인번호: INHA 2022-11-036). 모든 내시경적 단독 안와내벽감압술과 임상적인 평가는 단일 술자(S.M.K.)에 의해 이루어졌다.
모든 대상 환자에서 수술 전후 교정시력, 안압, 안구돌출 정도, 임상 활동도 점수(clinical activity score), 수술 전후 안구운동 등을 확인하였고 제1안위에서 측정한 2차원 얼굴 전산화단층촬영을 이용하여 수술 전 안와 길이, 안구 길이, 안구 길이와 안와 길이의 비, 안와첨부 각도, 사골동의 깊이, 안와내벽과 외벽의 길이, 외안근의 단면적, 수술 후 안와내벽의 결손된 길이, 결손된 안와내벽의 가장 후부에서 안와첨부까지의 길이를 확인하여 수술 전후 안와의 구조적인 형태를 파악하였다. 2차원 얼굴 전산화단층촬영의 축영상(axial scan) 중 수정체 음영이 관찰되는 단면에서 안구 길이를 측정하였고, 안와 길이는 상안와열의 하측 경계면에서 안와 입구의 중점까지의 길이를 측정하였다. 시신경관이 보이는 축영상에서 안와내벽과 외벽이 이루는 각도로 안와첨부 각도를 확인하였고10 가장 깊은 사골동의 깊이도 함께 측정하였다. 안와내벽과 외벽의 길이는 시신경관이 보이는 축영상에서 내측과 외측 안와 입구에서 안와첨부 사이 길이를 측정하였다.
11 관상영상(coronal scan)에서 외안근의 단면적이 최대 면적으로 관찰되는 관상영상을 기준으로 외안근의 단면적을 측정하였다. 수술 후 시행한 2차원 얼굴 전산화단층촬영 중 시신경관이 보이는 축영상에서 안와내벽의 결손 길이와 결손된 내벽의 가장 후부에서 안와첨부까지의 길이를 측정하였다(
Fig. 1). 추가로 수술 후 안와내벽의 결손된 길이와 전체 안와내벽 길이의 비를 계산하여 안구돌출 변화의 관계를 분석하였다. 모든 2차원 얼굴 전산화단층촬영 영상 분석 및 측정은 기준에 부합하는 수술 전후 특정 영상 단면으로 확인하였고 INFINITT PACS
® software (INFINITT Healthcare, Seoul, Korea)를 이용하였다.
모든 환자의 안구돌출 정도는 Hertel 안구돌출계로 좌우의 각막돌출 정도를 측정하고 수술 후 6개월 경과한 시점에 교정시력, 안압, 안구돌출 정도를 측정하여 경과를 비교하였다.
모든 환자에서 수술은 전신마취 하에 내시경을 이용하여 코경유 단독 안와내벽감압술로 시행하였다. Oxymetazoline을 적신 거즈를 코 안에 메워 코 안쪽 혈관 수축을 시키고 1:100,000 에피네프린이 섞인 리도카인을 구상돌기(uncinate process)에 주사한 후, 구상돌기절제술(uncinectomy)을 시행하였다.
13-15 최대한 안와첨부까지 안와내벽을 노출시키고 microcurette과 freer elevator를 이용하여 내벽을 분리시킨 뒤, 안와골막이 노출되면 sharp knife를 이용하여 안와골막을 절개하고 안와 연부조직을 사골동으로 탈출시켜 안와감압을 시행하였다(
Fig. 2).
16
통계 분석은 SPSS statistics ver. 18.0 (IBM Corp., Armonk, NY, USA)을 이용하여 안구돌출값의 변화와 각각의 요인에 대해 단변량선형회귀분석을 시행하였고 추가로 연관성을 보일 수 있는 요인들에 대해 다변량선형회귀분석을 시행하였다. p값이 0.05 미만인 경우 통계적으로 유의한 것으로 판단하였다.
결 과
대상 환자는 총 18명으로 남자 2명(11.1%), 여자 16명(88.9%)이었으며 평균 연령 31.3세, 갑상샘 질환의 유병 기간은 평균 4.2년, 수술 전 복시가 관찰된 환자는 1명, 안구 운동장애가 관찰된 환자는 2명이었고(
Table 1), 수술 후 복시가 새로 발생한 환자는 4명, 수술 후 복시가 악화된 환자는 1명, 안구운동장애가 관찰된 환자는 7명이었다(
Table 2). 수술 전 2차원 얼굴 전산화단층촬영에서 평균 안와 길이는 42.08 mm, 평균 안구 길이는 25.05 mm이고 평균 안와내벽 길이는 41.78 mm였다. 수술 후 안와내벽의 결손 길이는 평균 22.78 mm이며 결손된 내벽의 가장 후부에서 안와첨부까지의 길이의 평균 값은 10.27 mm였다. 수술 전후 안구돌 출값은 평균 2.48 mm 감소하였다(
Table 3).
단변량선형회귀분석에서 수술 전 안와내벽 길이(
p=0.032)와 수술 후 결손된 내벽의 가장 후부에서 안와첨부까지의 길이(
p=0.006)가 수술 전후 안구돌출값의 변화와 유의한 연관성이 있는 것으로 분석되었다. 그 외 안와 길이, 안구길이, 외안근의 단면적, 안와내벽 결손 길이는 통계적 유의성을 보이지 않았다(
Fig. 3,
Table 4). 단변량선형회귀분석에서 안구돌출값의 변화와 연관성을 보인 2가지 지표에 대하여 다변량선형회귀분석을 추가로 시행하였고 수술 후 결손된 안와내벽에서 안와첨부까지의 길이(
p=0.019)가 안구돌출값의 변화와 연관된 유의한 지표로 나타났다(
Table 5).
고 찰
갑상샘눈병증 환자에서 안와감압술을 시행할 때 안구돌출값의 변화는 다양한 요인의 영향을 받기 때문에 예측하는 것이 쉽지 않다.
9 안와감압술 후 안구돌출값의 변화는 지방 조직의 강성(stiffness), 외안근의 비대한 정도, 안와 구조 및 안구 크기가 영향을 미칠 수 있다고 알려져 있다.
10,16 이전 연구에서 안와내벽과 외벽의 감압술(balanced orbital decompression)을 시행한 환자에서 안와첨부 각도가 안구돌출값의 변화와 유의한 상관성을 보여주었고
11 Borumandi et al
10에 따르면 안와의 부피가 적거나 안구의 크기가 상대적으로 큰 경우 안와감압술로 인한 안구돌출의 감소 효과가 적을 것이라 예측할 수 있다고 주장하였다. 본 연구에서 측정된 안와 길이, 안구 길이, 안구 길이와 안와 길이의 비, 안와첨부 각도 모두 이전 동양인을 대상으로 시행한 안와 구조의 측정값과 유사하게 측정되었다.
17 단독 안와내벽감압술을 시행한 환자를 대상으로 안와첨부 각도와 안구돌출교정 정도의 연관성을 분석했을 때 통계적으로 유의한 결과를 보이지 않았다(
p=0.165). 2차원 영상 분석으로 안와의 부피를 예측하고자 하는 지표인 안구 길이(
p=0.675), 안와길이(
p=0.905), 안구 길이와 안와 길이의 비(
p=0.905)에서도 안구돌출값의 변화와 연관성이 없었다.
Oeverhaus et al
11에 따르면 외안근의 지름과 안구돌출값의 변화는 통계적으로 연관성이 없었으며 지방조직의 섬유화와 외안근의 부피를 확인하면 안구돌출값의 변화를 예측할 수 있을 것이라고 주장하였다. 외안근의 부피를 대신하여 외안근의 단면적을 통해 안와감압술에 따른 안구돌출의 교정 정도를 분석해보았으나 통계적으로 유의한 결과를 보이지 않았다. Alsuhaibani et al
18은 안와감압술을 시행한 뒤 외직근의 부피가 변화한다고 보고하였으며 Lee et al
17은 안구의 부피, 지방조직의 부피, 내직근의 부피는 실제 술 후 효과를 예측할 때 중요한 지표이나 실제로 모든 환자에서 이를 확인하는 데에는 어려움이 있다고 주장하였다.
본 연구에서는 내시경을 이용하여 코경유 단독 안와내벽감압수술을 시행하였기 때문에 안와내벽과 관련된 지표는 중요한 의미가 있을 것으로 생각된다. 단변량선형회귀분석에서 그중 수술 전 안와내벽의 길이(
p=0.032)와 수술 후 결손된 안와내벽에서 안와첨부까지의 길이(
p=0.006)가 수술 전후 안구돌출값의 변화와 유의한 관련성이 있는 것으로 확인되었다. 안와내벽의 길이는 안와의 부피를 예측할 수 있는 지표들 중 하나이면서 수술 범위와 직접적인 연관이 있는 안와 구조이기 때문일 것으로 추측된다. 단변량선형회귀분석에서 유의한 결과를 보인 지표들로 다변량선형회귀분석을 시행한 결과 수술 후 결손된 안와내벽에서 안와첨부까지의 길이와 안구돌출 감소 효과 사이에 유의한 관련성을 보였다(
p=0.019). 결손된 안와내벽에서 안와첨부까지의 길이가 짧을수록 더 많은 안구돌출 감소 효과를 보였고 이를 통해 안와첨부에 가까운 위치까지 안와내벽을 제거할수록 더 큰 감압 효과를 기대할 수 있을 것으로 생각된다. 하지만 본 연구에서 시신경관이 보이는 축영상에서 측정한 안와내벽 결손 길이와 전체 안와내벽 길이의 비가 평균 0.55로 확인된 점을 고려할 때 충분한 안와내벽의 제거가 이루어져야 효과적인 안와감압술이 가능할 것이다. 갑상샘눈병증 환자에서 안와감압술을 시행한 뒤 뇌척수액 유출, 뇌기종 등이 발생한 경우가 드물게 보고되었다.
19-22 이에 접형동을 유지하면서 후사골동의 안와내벽까지 제거하는 것이 수술 중 합병증을 예방하는 데에 도움이 될 수 있다. 따라서 갑상샘눈병증 환자에서 안와감압술을 시행할 때 안구돌출 교정 정도를 미리 예측하고 적절한 위치와 범위의 안와내벽을 제거해야 하며 교정 정도가 부족할 것으로 예상되면 수술 중 지방조직을 제거하거나 추가적인 안와감압술을 고려할 수 있다.
본 연구는 내시경을 이용하여 코경유 단독 안와내벽감압수술을 시행한 갑상샘눈병증 환자를 대상으로 했기 때문에 대상자의 수가 적다. 또한 2차원 얼굴 전산화단층촬영 결과를 분석하여 안와 구조물의 부피, 안와벽의 만곡도가 반영되지 않았다. 수술 후 안와내벽의 결손 길이는 감압 효과와 통계적인 연관성을 보이지 않은 점도 안와내벽의 결손된 범위를 입체적으로 반영하지 못했기 때문으로 판단된다. 갑상샘눈병증 환자를 대상으로 시행할 수 있는 다른 안와감압술(2 wall decompression, 3 wall decompression)에 대한 분석도 추가 연구가 필요할 것이다. 갑상샘눈병증 환자에서 안구돌출에 영향을 줄 수 있는 요인들은 유전, 면역, 환경 등을 포함하여 다양한 것으로 알려져 있고
23,24 안와감압술 후 안구돌출 감소 효과 역시 안와 구조 외 다양한 요인들이 영향을 줄 수 있을 것으로 생각되지만 본 연구에서는 안와 구조 외 다른 요인들에 대한 분석은 시행하지 않았다.
결론적으로 본 연구를 통해 내시경적 안와감압술을 시행한 갑상샘눈병증 환자에서 2차원 얼굴전산화단층촬영 영상을 통해 분석한 결손된 안와내벽에서 안와첨부까지의 길이는 수술 후 안구돌출 감소와 관련성이 높은 것으로 확인되었다. 따라서 후사골동을 최대한 포함하면서 충분한 범위의 안와내벽을 제거해야 효과적인 내시경적 안와감압술을 시행할 수 있을 것이다.
Figure 1.
Measurement of orbital parameters. (A) Globe length: antero-posterior globe length measured at optical lens level (yellow arrow), cone angle: angle between the medial and lateral orbital wall measured at optic canal level (blue arrows), medial orbital wall length: length from apex to medial orbital boundary measured at optic canal level (orange arrow), lateral orbital wall length: length from apex to lateral orbital boundary measured at optic canal level (red arrow), horizontal depth of ethmoid sinus measured at optic canal level (green arrow). (B) Measurement of orbital length: antero-posterior orbital length between orbital apex and the middle of the anterior orbital boundary line measured at the level of inferior end of superior orbital fissure (yellow arrows). (C) Size of extraocular muscle: maximum cross sectional area of extraocular muscle in coronal view (yellow lines). (D) Medial wall defect length (yellow arrow), distance from apex to medial wall defect measured at optic canal level (red arrow).
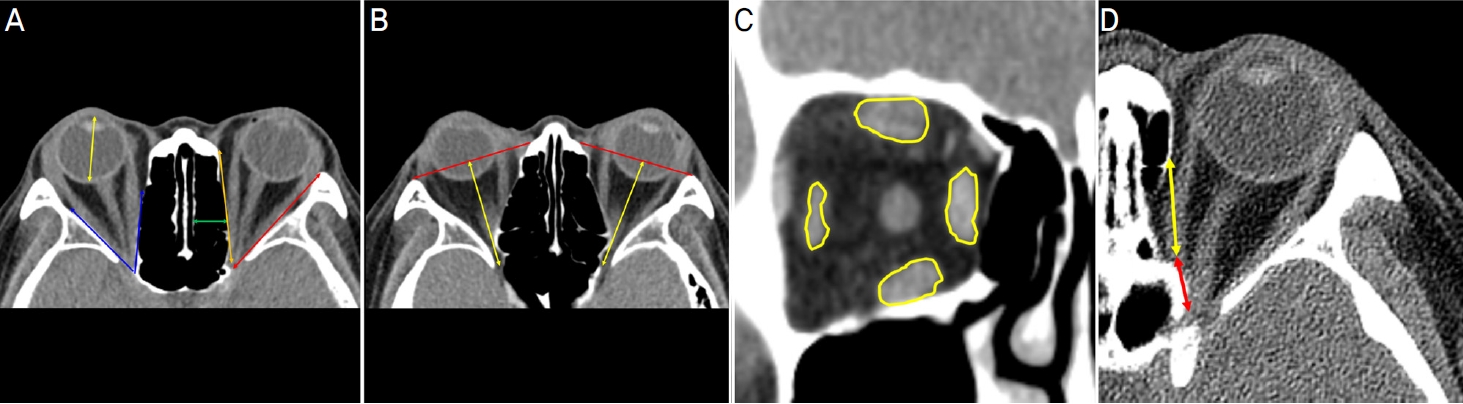
Figure 2.
Surgical procedure of the endoscopic orbital decompression. (A) Incision of the uncinate process. (B) Uncinectomy. (C) Anterior ethmoidectomy. (D) Periorbita after ethmoidectomy. (E) Incision of periorbita. (F) Orbital tissue prolapse into the ethmoid sinus.
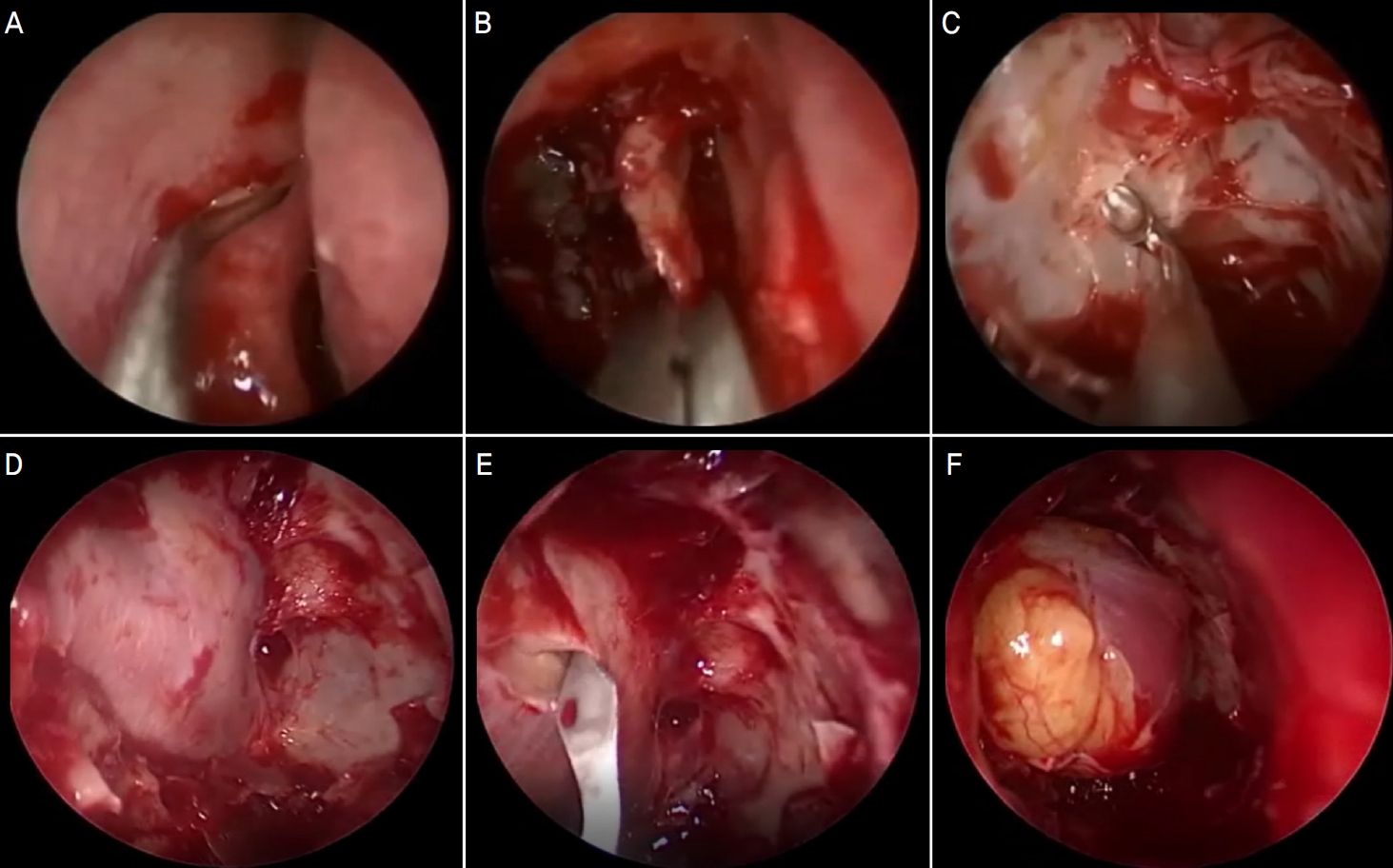
Figure 3.
The relationship between exophthalmos changes and orbital morphology by linear regression analysis. (A) Exophthalmos changes and distance from apex to medial wall defect. (B) Exophthalmos changes and medial wall length.
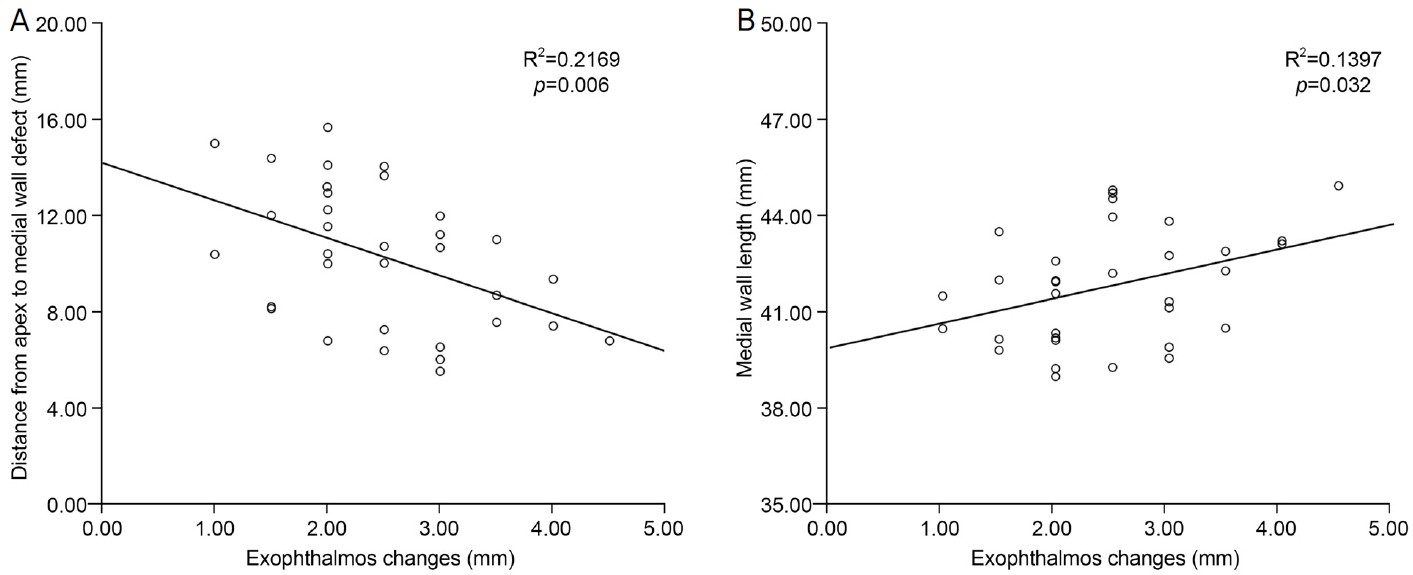
Table 1.
Baseline characteristics of patients
|
Patient characteristics |
n=18 |
|
Age (year) |
31.3 ± 10.3 |
|
Sex |
|
|
Male |
2 (11.1) |
|
Female |
16 (88.9) |
|
CAS (0-7) |
1.06 ± 1.22 |
|
Smoker |
5 (27.8) |
|
Duration of thyroid disease (years) |
4.2 ± 4.3 |
|
Thyroid function test results |
|
|
Free T4 |
1.44 ± 0.33 |
|
T3 |
111.65 ± 13.40 |
|
TSH |
2.14 ± 2.41 |
|
TRAb (IU/L) |
10.34 ± 13.56 |
|
TgAb (IU/mL) |
25.80 ± 18.64 |
|
Diplopia in primary gaze |
1 (5.6) |
|
Eye movement deficit |
2 (11.1) |
Table 2.
Postoperative characteristics of patients
|
Patient characteristics |
n=18 |
|
New onset diplopia in primary gaze |
4 (22.2) |
|
Worsening of preexisting diplopia |
1 (5.6) |
|
Eye movement deficit |
7 (38.9) |
Table 3.
|
Variable |
n=33 |
|
Preoperative measurements |
|
|
OL (mm) |
42.08 ± 2.14 |
|
GL (mm) |
25.05 ± 0.54 |
|
GL/OL ratio |
0.60 ± 0.03 |
|
Cone angle (°) |
48.59 ± 3.15 |
|
Medial wall length (mm) |
41.78 ± 1.77 |
|
Lateral wall length (mm) |
48.03 ± 2.22 |
|
Depth of ethmoidal sinus (mm) |
10.71 ± 1.76 |
|
Size of extraocular muscle (mm2) |
|
|
MR |
29.52 ± 5.87 |
|
LR |
22.88 ± 5.18 |
|
SR |
29.65 ± 9.34 |
|
IR |
28.59 ± 8.45 |
|
Postoperative measurements |
|
|
Medial wall defect length (mm) |
22.78 ± 3.26 |
|
Distance from apex to medial wall defect (mm) |
10.27 ± 2.85 |
|
Ratio of defect length to total medial wall length |
0.55 ± 0.08 |
|
Exophthalmos (mm) |
|
|
Preoperative exophthalmos |
19.74 ± 2.06 |
|
Postoperative exophthalmos |
17.26 ± 1.75 |
|
Exophthalmos changes |
2.48 ± 0.85 |
Table 4.
Univariate linear regression analysis of associations between parameters related orbital morphology and exophthalmos changes
|
Variable |
β |
95% CI |
p-value*
|
|
Preoperative measurements |
|
|
|
|
OL (mm) |
-0.009 |
-0.148 to 0.130 |
0.905 |
|
GL (mm) |
-0.118 |
-0.665 to 0.429 |
0.675 |
|
GL/OL ratio |
-0.623 |
-10.746 to 9.500 |
0.905 |
|
Cone angle (°) |
0.067 |
-0.025 to 0.159 |
0.165 |
|
Medial wall length (mm) |
0.179 |
0.022 to 0.336 |
0.032 |
|
Lateral wall length (mm) |
0.081 |
-0.050 to 0.212 |
0.238 |
|
Depth of ethmoidal sinus (mm) |
0.121 |
-0.044 to 0.286 |
0.159 |
|
Size of extraocular muscle (mm2) |
|
|
|
|
MR |
0.042 |
-0.005 to 0.089 |
0.086 |
|
LR |
0.051 |
-0.004 to 0.106 |
0.079 |
|
SR |
0.005 |
-0.026 to 0.036 |
0.751 |
|
IR |
0.017 |
-0.140 to 0.174 |
0.350 |
|
Postoperative measurements |
|
|
|
|
Medial wall defect length (mm) |
0.067 |
-0.021 to 0.155 |
0.148 |
|
Distance from apex to medial wall defect (mm) |
-0.139 |
-0.231 to -0.047 |
0.006 |
|
Ratio of defect length to total medial wall length |
0.152 |
-2.154 to 5.494 |
0.399 |
Table 5.
Multivariate linear regression analysis of associations between parameters related orbital morphology and exophthalmos changes
|
Variable |
β |
95% CI |
p-value*
|
|
Preoperative measurements |
|
|
|
|
Medial wall length (mm) |
0.13 |
-0.019 to 0.279 |
0.099 |
|
Postoperative measurements |
|
|
|
|
Distance from apex to medial wall defect (mm) |
-0.118 |
-0.212 to -0.024 |
0.019 |
REFERENCES
4) Burch HB, Wartofsky L. Graves’ ophthalmopathy: current concepts regarding pathogenesis and management. Endocr Rev 1993;14:747-93.


7) Kennedy DW, Goodstein ML, Miller NR, Zinreich SJ. Endoscopic transnasal orbital decompression. Arch Otolaryngol Head Neck Surg 1990;116:275-82.
8) Ting JY, Sindwani R. Endoscopic orbital decompression. Oper Tech Otolaryngol Head Neck Surg 2014;25:213-7.
9) Borumandi F, Hammer B, Kamer L, von Arx G. How predictable is exophthalmos reduction in Graves' orbitopathy? A review of the literature. Br J Ophthalmol 2011;95:1625-30.
10) Borumandi F, Hammer B, Noser H, Kamer L. Classification of orbital morphology for decompression surgery in Graves' orbitopathy: two-dimensional versus three-dimensional orbital parameters. Br J Ophthalmol 2013;97:659-62.
12) Schiff BA, McMullen CP, Farinhas J, et al. Use of computed tomography to assess volume change after endoscopic orbital decompression for Graves' ophthalmopathy. Am J Otolaryngol 2015;36:729-35.
13) Kim JE, Kang SM. Factors associated with postoperative strabismus by endoscopic orbital decompression in patients with thyroid-associated ophthalmopathy. J Korean Ophthalmol Soc 2021;62:729-38.

14) Michel O, Oberländer N, Neugebauer P, et al. Follow-up of transnasal orbital decompression in severe Graves' ophthalmopathy. Ophthalmology 2001;108:400-4.
15) Levy J, Puterman M, Lifshitz T, et al. Endoscopic orbital decompression for Graves’ ophthalmopathy. Isr Med Assoc J 2004;6:673-6.
16) Kim JW, Kang SM. Surgical outcomes of endoscopic medial orbital wall decompression. J Craniofac Surg 2020;31:197-200.
17) Lee JS, Lee H, Chang MW, et al. Orbital morphology for decompression surgery in thyroid eye disease using 2-D orbital CT and 4 parameters. J Korean Ophthalmol Soc 2014;55:1267-71.
18) Alsuhaibani AH, Carter KD, Policeni B, Nerad JA. Effect of orbital bony decompression for Graves' orbitopathy on the volume of extraocular muscles. Br J Ophthalmol 2011;95:1255-8.
19) Warren JD, Spector JG, Burde R. Long-term follow-up and recent observations on 305 cases of orbital decompression for dysthyroid orbitopathy. Laryngoscope 1989;99:35-40.
21) Limawararut V, Valenzuela AA, Sullivan TJ, et al. Cerebrospinal fluid leaks in orbital and lacrimal surgery. Surv Ophthalmol 2008;53:274-84.
22) Graham SM, Brown CL, Carter KD, et al. Medial and lateral orbital wall surgery for balanced decompression in thyroid eye disease. Laryngoscope 2003;113:1206-9.
23) Menconi F, Marcocci C, Marinò M. Diagnosis and classification of Graves' disease. Autoimmun Rev 2014;13:398-402.
Biography
이준섭 / Jun Seob Lee
인하대학교 의과대학 안과학교실
Department of Ophthalmology, Inha University School of Medicine



 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






