

ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņןņØĆ ņĢłņĢĢņØ┤ ņĀĢņāü ļ▓öņ£äņØ┤ļ®┤ņä£ ļģ╣ļé┤ņןņØś ĒŖ╣ņ¦ĢņĀüņØĖ ņ¦äĒ¢ēņä▒ ņŗ£ņŗĀĻ▓Į ņåÉņāüĻ│╝ ĻĘĖņŚÉ ļö░ļźĖ ņŗ£ņĢ╝ Ļ▓░ņåÉņØä ļ│┤ņØ┤ļŖö ņ¦łĒÖśņØ┤ļŗż[1,2]. Ļ│ĀņĢłņĢĢļģ╣ļé┤ņןĻ│╝ ļ╣äĻĄÉĒĢśņŚ¼, ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņןņŚÉņä£ļŖö ņĢłņĢĢĻ│╝ Ļ┤ĆļĀ©ļÉ£ ĻĖ░Ļ│äņĀüņØĖ ņåÉņāüļ│┤ļŗżļŖö ĒśłņĢĢ, ņ×ÉĻ░Ćļ®┤ņŚŁ, ņāØņ▓┤ņŚŁĒĢÖņÜöņØĖ(biomechanical factor) ļō▒ņØś ņĀäņŗĀ ņØĖņ×ÉļōżņØ┤ ņŗ£ņŗĀĻ▓Į ņåÉņāüņŚÉ ņżæņÜöĒĢ£ ņŚŁĒĢĀņØä ĒĢĀ Ļ▓āņ£╝ļĪ£ ņĀ£ĻĖ░ļÉśņ¢┤ ņÖöļŗż[3,4]. ĒĢśņ¦Ćļ¦ī ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉņŚÉņä£ļÅä ņĢłņĢĢņØ┤ ļåÆņØäņłśļĪØ ļģ╣ļé┤ņןņØś ļ░£ļ│æ ņ£äĒŚśņØ┤ ļåÆĻ│Ā[5], ņĢłņĢĢĒĢśĻ░Ģ ņ╣śļŻīĻ░Ć ņŗ£ņŗĀĻ▓Į ņåÉņāüņØś ņ¦äĒ¢ē ņ£äĒŚśņØä ļé«ņČöĻĖ░ ļĢīļ¼ĖņŚÉ[6], ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņןņŚÉņä£ļÅä ņĢłņĢĢĻ│╝ Ļ┤ĆļĀ©ļÉ£ ņé¼ņāüĒīÉņØś ĻĖ░Ļ│äņĀüņØĖ ņåÉņāü ļ░Å ļ│ĆĒśĢņØ┤ ņŗ£ņŗĀĻ▓Į ņåÉņāüņØś ļ│æĒā£ņāØļ”¼ņŚÉ ņżæņÜöĒĢ£ ņŚŁĒĢĀņØä ĒĢĀ Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż[4,5].
ņé¼ņāüĒīÉņØĆ Ēæ£ņĖĄņŗĀĻ▓Įņä¼ņ£ĀņĖĄ, ņé¼ņāüĒīÉņĀäņĖĄĻ│╝ ĒĢ©Ļ╗ś ņŗ£ņŗĀĻ▓Įņ£ĀļæÉļź╝ ņØ┤ļŻ©ļŖö ĻĘĖļ¼╝ļ¬©ņ¢æņØś ĻĄÉņøÉņ¦ł ĒīÉņ£╝ļĪ£, ļ¦Øļ¦ē ņŗĀĻ▓ĮņĀł ņäĖĒż(retinal ganglion cell, RGC)ņØś ņČĢņéŁ(axon)ņØ┤ ĒåĄĻ│╝ĒĢśļŖö ĻĄ¼ņĪ░ļ¼╝ņØ┤ļŗż. ņé¼ņāüĒīÉņØś ļ│ĆĒśĢņØĆ ļģ╣ļé┤ņןņä▒ ņŗ£ņŗĀĻ▓Į ņåÉņāüņŚÉ ņżæņÜöĒĢ£ ņŚŁĒĢĀņØä ĒĢĀ Ļ▓āņ£╝ļĪ£ ņČöņĀĢļÉ£ļŗż[7-9]. ņé¼ņāüĒīÉĻ▓Įņ£ĀņĢĢļĀźņ░©(trans-lamina cribrosa pressure difference = intraocular pressure - intracranial pressure) ļ░Å ņé¼ņāüĒīÉņØś Ēāäņä▒ ĒŖ╣ņä▒(elastoplastic property of lamina cribrosa)ņŚÉ ņØśĒĢ┤ Ļ▓░ņĀĢļÉśļŖö ņé¼ņāüĒīÉņØś ĒśĢĒā£ļŖö[10] ļģ╣ļé┤ņן ĒÖśņ×ÉņŚÉņä£ ņĀĢņāüņØĖĻ│╝ ļ╣äĻĄÉĒĢśņŚ¼ Ļ╣Ŗņ¢┤ņ¦äļŗżĻ│Ā ņĢīļĀżņĀĖ ņ׳ļŗż[11]. ņØ┤ļ¤¼ĒĢ£ ņé¼ņāüĒīÉņØś Ļ╣Ŗņ¢┤ņ¦ÉņØĆ ņé¼ņāüĒīÉņØä ņ¦ĆļéśļŖö RGC axonņØś axonal transportļź╝ ņĀĆĒĢ┤ņŗ£ĒéżĻ│Ā, ņä▒ņāüĻĄÉņäĖĒżņŚÉ ņØśĒĢ£ Ļ▓░ĒĢ®ņĪ░ņ¦üņØś ļ│ĆĒśĢ ļō▒ņØś Ļ│╝ņĀĢņØä ĒåĄĒĢ┤ RGCņØś ņåÉņāüņØä ņ┤ēņ¦äņŗ£Ēé┤[12]Ļ│╝ ļÅÖņŗ£ņŚÉ ņé¼ņāüĒīÉ ļé┤ņØś ļ¬©ņäĖĒśłĻ┤ĆņŚÉņä£ ņØĖņĀæĒĢ£ RGC axonņ£╝ļĪ£ņØś ņśüņ¢æļČä ĒÖĢņé░ņØä ļ░®ĒĢ┤ĒĢ©ņ£╝ļĪ£ņŹ©, ļģ╣ļé┤ņןņä▒ ņŗ£ņŗĀĻ▓Į ņåÉņāüņØä ņ£Āļ░£ĒĢśĻ│Ā ņ¦äĒ¢ēņØä ņ┤ēņ¦äņŗ£Ēé¼ Ļ▓āņ£╝ļĪ£ ņČöņĀĢļÉ£ļŗż[7].
Enhanced depth imaging (EDI) ļ░®ļ▓ĢņØä ņØ┤ņÜ®ĒĢ£ ņŖżĒÄÖĒŖĖļ¤╝ ņśüņŚŁ ļ╣øĻ░äņäŁļŗ©ņĖĄņ┤¼ņśü(spectral domain optical coherence tomography, SD-OCT)ņØś ļ░£ļŗ¼ļĪ£ ņé¼ņāüĒīÉ ņĪ░ņ¦üņØś ņäĖļ░ĆĒĢ£ ņśüņāüņØä ņ¢╗ņØä ņłś ņ׳Ļ▓ī ļÉśņ¢┤ ļģ╣ļé┤ņן ĒÖśņ×ÉņŚÉņä£ ņé¼ņāüĒīÉņØś ļ»ĖņäĖ ĻĄ¼ņĪ░ņÖĆ ļģ╣ļé┤ņןņä▒ ņŗ£ņŗĀĻ▓Į ņåÉņāüĻ│╝ņØś Ļ┤ĆļĀ©ņä▒ņŚÉ ļīĆĒĢ£ ņŚ░ĻĄ¼Ļ░Ć Ļ░ĆļŖźĒĢ┤ņĪīļŗż. Ļ│ĀņĢłņĢĢļģ╣ļé┤ņן ļ┐Éļ¦ī ņĢäļŗłļØ╝, ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉņŚÉņä£ļÅä ņĀĢņāüņØĖĻ│╝ ļ╣äĻĄÉĒĢśņŚ¼ ņé¼ņāüĒīÉņØ┤ Ļ╣ŖĻ│Ā[11], ņé¼ņāüĒīÉņØś ļ│ĆĒśĢņØ┤ ļģ╣ļé┤ņןņØś ļ░£ņāØĻ│╝ Ļ┤ĆļĀ©ņØ┤ ņ׳ņ¢┤, ņ╣śļŻī ņĀä ņĢłņĢĢņØ┤ ņĀĢņāü ļ▓öņ£äņØĖ ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉņŚÉņä£ļÅä ņé¼ņāüĒīÉņØś ĒśĢĒā£ĒĢÖņĀü ļ│ĆĒśĢņØ┤ ņŗ£ņŗĀĻ▓Į ņåÉņāüņØś ļ│æĒā£ņāØļ”¼ņŚÉ ņżæņÜöĒĢ£ ņŚŁĒĢĀņØä ĒĢĀ Ļ▓āņ×äņØ┤ ņĀ£ĻĖ░ļÉśņŚłļŗż[5]. ĒĢśņ¦Ćļ¦ī Ēśäņ×¼Ļ╣īņ¦Ć ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×Éļź╝ ļīĆņāüņ£╝ļĪ£ ņé¼ņāüĒīÉņØś ĒśĢĒā£ņÖĆ ļģ╣ļé┤ņן ņżæļō▒ļÅäņÖĆņØś ņāüĻ┤Ćņä▒ņØä ĒÖĢņØĖĒĢ£ ņŚ░ĻĄ¼ļŖö ņŚåņŚłļŗż.
Ļ│ĀņĢłņĢĢļģ╣ļé┤ņןĻ│╝ ļ╣äĻĄÉĒĢśņŚ¼, ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉņØś ņŗ£ņŗĀĻ▓Į ņåÉņāüņŚÉļŖö ņĀäņŗĀ ĒśłņĢĢ(ĒŖ╣Ē׳, ņĢ╝Ļ░ä ņĀĆĒśłņĢĢ) ļō▒ņØś ņĀäņŗĀ ņ£äĒŚśņØĖņ×ÉĻ░Ć ņżæņÜöĒĢ£ ņŚŁĒĢĀņØä ĒĢĀ Ļ▓āņ£╝ļĪ£ ņČöņĀĢļÉ£ļŗż[13,14]. ļśÉĒĢ£ ļ╣äņŖĘĒĢ£ ņŗ£ņŗĀĻ▓Į ņåÉņāüņØä Ļ░Ćņ¦ä ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉņŚÉņä£ļÅä ņé¼ņāüĒīÉņØś ļ│ĆĒśĢ ņĀĢļÅä ļ░Å ņĀäņŗĀ ņØĖņ×ÉņØś ĒŖ╣ņä▒ņØ┤ ļŗżļź┤ļŗż[15]. ņØ┤ļ¤¼ĒĢ£ ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ļź╝ Ļ│ĀļĀżĒĢĀ ļĢī, ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉņØś ņŗ£ņŗĀĻ▓Į ņåÉņāüĻ│╝ Ļ┤ĆļĀ©ļÉ£ ņĢłņØĖņ×É ļČäņäØņŚÉņä£ļŖö ĒÖśņ×É Ļ░£ļ│äņØś ĒŖ╣ņä▒ ļ░Å ņĀäņŗĀ ņ£äĒŚśņØĖņ×ÉņØś ļ│┤ņĀĢņØ┤ ņżæņÜöĒĢśņ¦Ćļ¦ī, ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉļōżņØś Ļ░£ņØĖĻ░ä ļ╣äĻĄÉ ņŚ░ĻĄ¼ņŚÉņä£ ņØ┤ļ¤¼ĒĢ£ ņĀäņŗĀ ņØĖņ×É ļ│┤ņĀĢņØĆ ĒśäņŗżņĀüņ£╝ļĪ£ ņĀ£ĒĢ£ņĀüņØ╝ ņłśļ░¢ņŚÉ ņŚåļŗż. ņØ┤ļ¤¼ĒĢ£ ņĖĪļ®┤ņŚÉņä£ ņ¢æņĢłņØś ņŗ£ņŗĀĻ▓Į ņåÉņāüņØś ņĀĢļÅäĻ░Ć ļŗżļźĖ ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉņŚÉņä£ Ļ░£ņØĖ ļé┤ ņ¢æņĢł ļ╣äĻĄÉļź╝ ĒåĄĒĢ┤ ļģ╣ļé┤ņןņØś ņżæļō▒ļÅäņÖĆ Ļ┤ĆļĀ©ļÉ£ ņĢłņØĖņ×Éļź╝ ļ╣äĻĄÉ ļČäņäØ ĒĢśļŖö Ļ▓āņØĆ ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņןņØś ļ│æņØĖĻ│╝ Ļ┤ĆļĀ©ļÉ£ ņĀäņŗĀ ņØĖņ×ÉĻ░Ć ļ│┤ņĀĢļÉśļŖö ņĖĪļ®┤ņŚÉņä£ ņןņĀÉņØ┤ ņ׳ļŗż. ņØ┤ņŚÉ ļ│Ė ņŚ░ĻĄ¼ļŖö ņŗ£ņŗĀĻ▓Į ņåÉņāüņØś ņĀĢļÅäĻ░Ć ļŗżļźĖ ņ¢æņĢł ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉņŚÉņä£ ņ¢æņĢłņØś ņé¼ņāüĒīÉ Ļ╣ŖņØ┤(lamina cribrosa depth, LCD)ļź╝ ļ╣äĻĄÉĒĢśĻ│Ā, ņŗ£ņŗĀĻ▓Į ņåÉņāüņØś ņĀĢļÅäņÖĆ LCDņÖĆņØś ņŚ░Ļ┤Ćņä▒ņØä ņĢīņĢäļ│┤Ļ│Āņ×É ĒĢśņśĆļŗż.
ļīĆņāüĻ│╝ ļ░®ļ▓Ģ
2021ļģä 9ņøöļČĆĒä░ 2022ļģä 2ņøöĻ╣īņ¦Ć ļ│ĖņøÉ ņĢłĻ│╝ņŚÉ ļé┤ņøÉĒĢ£ ņ¢æņĢł ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×É ņżæņŚÉ, ņ¢æņĢłņØś ņŗ£ņŗĀĻ▓Į ņåÉņāüņØś ņżæļō▒ļÅäĻ░Ć ļŗżļźĖ ĒÖśņ×ÉļōżņØä ļīĆņāüņ£╝ļĪ£ SD-OCTļź╝ ņØ┤ņÜ®ĒĢ£ horizontal optic nerve head (ONH) B-scan ļ░Å ņØśļ¼┤ĻĖ░ļĪØņØä ĒøäĒ¢źņĀüņ£╝ļĪ£ ļČäņäØĒĢśņśĆļŗż. ļ│Ė ņŚ░ĻĄ¼ļŖö Ļ░ĢņøÉļīĆĒĢÖĻĄÉ ņŚ░ĻĄ¼ņ£żļ”¼ņŗ¼ņØśņ£äņøÉĒÜī(Institutional Review Board, IRB)ļĪ£ļČĆĒä░ ņŖ╣ņØĖ ļ▓łĒśĖ 2021-11-005ļĪ£ ņŗ¼ņØś ņŖ╣ņØĖņØä ļ░øņĢśņ£╝ļ®░, ĒŚ¼ņŗ▒ĒéżņäĀņ¢Ė(Declaration of Helsinki)ņŚÉ ņØśĻ▒░ĒĢśņŚ¼ ņŚ░ĻĄ¼ļź╝ ņŗ£Ē¢ēĒĢśņśĆļŗż.
ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņןņØĆ ņĢłņĢĢņØ┤ 21 mmHg ņØ┤ĒĢśņØ┤ļ®┤ņä£ ņĀäļ░®Ļ░üņØĆ ņŚ┤ļĀż ņ׳Ļ│Ā, ļģ╣ļé┤ņןņä▒ ņŗ£ņŗĀĻ▓Į ņåÉņāüĻ│╝ ņØ┤ņŚÉ ļö░ļźĖ ņŗ£ņĢ╝Ļ▓░ņåÉņØ┤ ļÅÖļ░śļÉ£ Ļ▓ĮņÜ░ļĪ£ ņĀĢņØśĒĢśņśĆļŗż. ļģ╣ļé┤ņןņØś ņżæņ”ØļÅäļŖö ņŗ£ņĢ╝Ļ▓Ćņé¼ņØś mean deviation (MD)Ļ░ÆņØä ĻĖ░ņżĆņ£╝ļĪ£, 1) ņ┤łĻĖ░(MD > -6 dB), 2) ņżæĻĖ░(-6 dB Ōēź MD Ōēź -12 dB), 3) ļ¦ÉĻĖ░(MD < -12 dB)ņØś ņäĖ ļŗ©Ļ│äļĪ£ ņĀĢņØśĒĢśņśĆļŗż[16-18]. ņ¢æņĢłņØś ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×É ņżæ ņ¢æņĢł ņŗ£ņĢ╝Ļ▓░ņåÉņØś ņżæļō▒ļÅäĻ░Ć ņä£ļĪ£ ļŗżļź┤ļ®┤ņä£ ņ¢æņĢłņØś MD ņ░©ņØ┤Ļ░Ć 3 ņØ┤ņāüņØĖ ĒÖśņ×ÉļōżņØä ņŚ░ĻĄ¼ņŚÉ ĒżĒĢ©ņŗ£ņ╝░ļŗż[19].
ņŗ£ņĢ╝Ļ▓Ćņé¼ļŖö ĒŚśĒöäļ”¼ ņ×ÉļÅÖņŗ£ņĢ╝Ļ│ä(Humphrey┬« visual field analyzer 740i, Carl Zeiss Meditec Inc., Dublin, CA, USA)ņØś Central 24-2 SITA-standard strategyļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ ļæÉ ļ▓ł ņØ┤ņāü ņŗ£Ē¢ēĒĢśņśĆļŗż. Ļ░Ćņ¢æņä▒ 15%, Ļ░ĆņØīņä▒ 15%, ņŻ╝ņŗ£ ņāüņŗż 20%ļź╝ ņ┤łĻ│╝ĒĢśļŖö Ļ▓ĮņÜ░ ĒĢ┤ļŗ╣ ņŗ£ņĢ╝Ļ▓Ćņé¼ņØś Ļ▓░Ļ│╝ļŖö ļČäņäØņŚÉņä£ ņĀ£ņÖĖĒĢśņśĆļŗż. ļģ╣ļé┤ņןņä▒ ņŗ£ņĢ╝ Ļ▓░ņåÉņØĆ 1) pattern deviation plotņŚÉņä£ ĻČüņāü ņśüņŚŁņŚÉ ņ׳ļŖö 3Ļ░£ ņØ┤ņāüņØś ņĀÉņØś ņŚŁņ╣ś(mean sensitivity)Ļ░Ć ņĀĢņāüņØś 5% ļ»Ėļ¦īņ£╝ļĪ£ ļéśĒāĆļéśĻ│Ā ĻĘĖņżæ ĒĢ£ ņĀÉņØ┤ 1% ļ»Ėļ¦īņØ╝ ļĢī, ļśÉļŖö 2) glaucoma hemifield testņŚÉņä£ outside normal limitsĻ░Ć ļæÉ ļ▓ł ņŚ░ņåŹņ£╝ļĪ£ ļéśĒāĆļéĀ ļĢī, ļśÉļŖö 3) corrected pattern standard deviation (PSD)ņØ┤ ņĀĢņāüņØś 5% ļ»Ėļ¦īņ£╝ļĪ£ ļéśĒāĆļéĀ ļĢīļĪ£ ņĀĢņØśĒĢśņśĆļŗż[20-22]. ņĢłņĢĢņØ┤ 21 mmHgļ│┤ļŗż ļåÆĻ▒░ļéś, ĒÅÉņćäĻ░üļģ╣ļé┤ņן ļ░Å ņØ┤ņ░©ļģ╣ļé┤ņן, ņŗ£ņŗĀĻ▓ĮņŚ╝ņØ┤ļéś ĻĖ░ĒāĆ ļ╣äļģ╣ļé┤ņןņä▒ ņŗ£ņŗĀĻ▓Įļ│æņ”Ø, ņŗ£ņĢ╝ ņØ┤ņāüņØä ņØ╝ņ£╝Ēé¼ ņłś ņ׳ļŖö ļŗżļźĖ ļ│æļ│ĆņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░, ņĢłņĢĢ ņĖĪņĀĢņŚÉ ņśüĒ¢źņØä ņżä ņłś ņ׳ļŖö Ļ░üļ¦ēņ¦łĒÖśņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ ņŚ░ĻĄ¼ ļīĆņāüņŚÉņä£ ņĀ£ņÖĖĒĢśņśĆļŗż.
ĻĖ░ņĀĆņĢłņĢĢņØĆ ņ╣śļŻīļź╝ ņŗ£ņ×æĒĢśĻĖ░ ņĀäņØś ņĢłņĢĢņ£╝ļĪ£ ņĀĢņØśĒĢśņśĆļŗż. ņ┤łņ¦ä ņŗ£ ņĢłņĢĢĒĢśĻ░ĢņĀ£ļź╝ ņé¼ņÜ®ĒĢśĻ│Ā ņ׳ļŖö ĒÖśņ×ÉņØś Ļ▓ĮņÜ░, ņåīĻ▓¼ņä£ ņāü ņĢĮļ¼╝ņ╣śļŻī ņĀä ņĢłņĢĢņØ┤ ļ¬ģņŗ£ļÉśņ¢┤ ņ׳ļŖö Ļ▓ĮņÜ░ļ¦īņØä ļČäņäØņŚÉ ĒżĒĢ©ĒĢśņśĆļŗż[23]. OCT Ļ▓Ćņé¼ ņŗ£ ņĢłņĢĢņØĆ SD-OCTļź╝ ņØ┤ņÜ®ĒĢ£ horizontal ONH B-scanņØä ņŗ£Ē¢ēĒĢśļŖö ļéĀĻ│╝ ļÅÖņØ╝ĒĢ£ ļéĀņŚÉ ņĖĪņĀĢĒĢ£ ņĢłņĢĢņ£╝ļĪ£ ņĀĢņØśĒĢśņśĆļŗż.
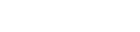
LCDļŖö ļæÉ ļ¬ģņØś ņłÖļĀ©ļÉ£ ņŚ░ĻĄ¼ņ×ÉĻ░Ć ĒÖśņ×ÉļōżņØś ņ×äņāü ņĀĢļ│┤ļź╝ ļ¬©ļź┤ļŖö ņāüĒā£ņŚÉņä£, Heidelberg Eye Explorer ņåīĒöäĒŖĖņø©ņ¢┤ (version 1.5.12.0)ņŚÉ ļé┤ņןļÉ£ caliper tool (draw region)ņØä ņØ┤ņÜ®ĒĢśņŚ¼ ņĖĪņĀĢĒĢśņśĆļŗż. ONH horizontal B-scan ņśüņāüņØĆ ņłÖļĀ©ļÉ£ Ļ▓Ćņé¼ņ×ÉļōżņØ┤ ņŖżĒÄÖĒŖĖļ¤╝ņśüņŚŁ ļ╣øĻ░äņäŁļŗ©ņĖĄņ┤¼ņśü(Heidelberg Engineering, Heidelberg, Germany)ņØś EDI ļ░®ļ▓ĢņØä ņØ┤ņÜ®ĒĢśņŚ¼ ņ¢╗ņŚłļŗż[24]. ONHņØś ņłśņ¦ü Ļ▒░ļ”¼Ļ░Ć ļÅÖņØ╝ĒĢ£ 3Ļ░£ņØś ņ£äņ╣ś(plane 1ļČĆĒä░ 3Ļ╣īņ¦Ć)ņŚÉņä£ ņ¢╗ņØĆ 3Ļ░£ņØś horizontal B-scan ņśüņāüņŚÉņä£ LCDļź╝ ņĖĪņĀĢĒĢśņśĆļŗż. LCDļŖö BruchŌĆÖs membrane opening (BMO)ņØś Ļ░Ćņןņ×Éļ”¼ļź╝ ņŚ░Ļ▓░ĒĢśļŖö ĻĖ░ņżĆņäĀņŚÉņä£ ņé¼ņāüĒīÉņØś ņĢ×ņ¬Į Ēæ£ļ®┤Ļ╣īņ¦ĆņØś ņĄ£ļīĆ ņłśņ¦ü Ļ▒░ļ”¼ļĪ£ ņĀĢņØśĒĢśņśĆļŗż(Fig. 1) [5,25]. ņé¼ņāüĒīÉņØś ņĢ×ņ¬Į Ēæ£ļ®┤ņØ┤ ļ¬ģĒÖĢĒĢśĻ▓ī ļ│┤ņØ┤ņ¦Ć ņĢŖļŖö Ļ▓ĮņÜ░ņŚÉļŖö 30-35 ╬╝m ņĀĢļÅä ņ░©ņØ┤ ļéśļŖö ĻĘĖ ļŗżņØī ļŗ©ļ®┤ņØä ņØ┤ņÜ®ĒĢśņŚ¼ ņĖĪņĀĢĒĢśņśĆļŗż. OCT ņØ┤ļ»Ėņ¦ĆņØś quality scoreĻ░Ć 15ļź╝ ļäśļŖö Ļ▓ĮņÜ░ļ¦ī ĒżĒĢ©ĒĢśņśĆĻ│Ā, BMOļéś ņé¼ņāüĒīÉņØś ņĢ×ņ¬Į Ēæ£ļ®┤ņØ┤ ļ¬ģĒÖĢĒĢśĻ▓ī ĻĄ¼ļČäļÉśņ¦Ć ņĢŖļŖö Ļ▓ĮņÜ░ļŖö ļČäņäØņŚÉņä£ ņĀ£ņÖĖĒĢśņśĆļŗż. ĒÅēĻĘĀ LCDļŖö plane 1-3ņŚÉņä£ ņĖĪņĀĢĒĢ£ Ļ░ÆņØś ĒÅēĻĘĀĻ░Æņ£╝ļĪ£ ņĀĢņØśĒĢśņśĆĻ│Ā, ļæÉ ļ¬ģņØś ņŚ░ĻĄ¼ņ×ÉĻ░Ć ņĖĪņĀĢĒĢ£ Ļ░ÆņØś ĒÅēĻĘĀĻ░ÆņØä ļČäņäØņŚÉ ņØ┤ņÜ®ĒĢśņśĆļŗż. ļæÉ ņŚ░ĻĄ¼ņ×É Ļ░äņØś ņĖĪņĀĢ ņØ╝ņ╣śļÅäļź╝ ĒÅēĻ░ĆĒĢśĻĖ░ ņ£äĒĢ┤ 95% Bland-Altman limits of agreementļź╝ ņØ┤ņÜ®ĒĢśņśĆļŗż[5,25].
ļ¬©ļōĀ ņ×ÉļŻīļōżņØĆ ĒÅēĻĘĀĻ░Æ ┬▒ Ēæ£ņżĆĒÄĖņ░©ļĪ£ Ēæ£ĻĖ░ĒĢśņśĆļŗż. ņ¢æņĢłņØś ņĢłņØĖņ×É(ocular factor) ļ╣äĻĄÉ ļČäņäØņØĆ paired t-testļź╝ ņØ┤ņÜ®ĒĢśņśĆļŗż. ņĪ░Ļ▒┤ļČĆ ļĪ£ņ¦ĆņŖżĒŗ▒ ĒÜīĻĘĆļČäņäØ(conditional logistic regression)ņØä ņØ┤ņÜ®ĒĢśņŚ¼ ļģ╣ļé┤ņן ņżæļō▒ļÅäņÖĆ Ļ┤ĆļĀ©ļÉ£ ņØĖņ×Éļź╝ ļČäņäØĒĢśņśĆļŗż. ņåÉņāüņØ┤ ņŗ¼ĒĢ£ ļłł ĻĘĖļŻ╣Ļ│╝ ļ░śļīĆ ļłł ĻĘĖļŻ╣ņŚÉņä£ LCDņÖĆ Ļ┤ĆļĀ© ņØĖņ×Éļź╝ ļČäņäØĒĢśĻĖ░ ņ£äĒĢ┤ ņäĀĒśĢĒÜīĻĘĆļČäņäØ(linear regression analysis)ņØä ņØ┤ņÜ®ĒĢśņśĆļŗż. ļŗżņżæļ╣äĻĄÉņŚÉ ņØśĒĢ£ ņ£äļ░£Ļ▓¼ņ£©(false discovery rate)ņØś ļ│┤ņĀĢņØĆ Benjamini-Hochberg ļ░®ļ▓ĢņØä ņØ┤ņÜ®ĒĢśņśĆņ£╝ļ®░, ļÅģļ”Įļ│Ćņłśļōż Ļ░äņØś ļŗżņżæĻ│ĄņäĀņä▒ ĒÖĢņØĖņØä ņ£äĒĢ┤ ļČäņé░ĒīĮņ░ĮĻ│äņłś(variance inflation factor)ļź╝ ņØ┤ņÜ®ĒĢśņśĆļŗż. ļŗ©ļ│Ćļ¤ē ļČäņäØņŚÉņä£ ļ│Ćņłś ņżæ pĻ░ÆņØ┤ 0.1 ņØ┤ĒĢśņØĖ ļ│ĆņłśļōżļĪ£ ļŗżļ│Ćļ¤ē ļČäņäØņØä ņŗ£Ē¢ēĒĢśņśĆļŗż. ĒåĄĻ│äņĀü ļČäņäØņØĆ SPSS IBM┬« version 22.0 (IBM Corp., Armonk, NY, USA)ļź╝ ņé¼ņÜ®ĒĢśņśĆņ£╝ļ®░, ĒåĄĻ│äĒĢÖņĀü ņ£ĀņØś ņłśņżĆņØĆ 0.05 ļ»Ėļ¦īņ£╝ļĪ£ ĒĢśņśĆļŗż.
Ļ▓░ Ļ│╝
ņ┤Ø 52ļ¬ģņØś ņ¢æņĢł ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉĻ░Ć ļ│Ė ņŚ░ĻĄ¼ņŚÉ ĒżĒĢ©ļÉśņŚłļŗż(Table 1). ĒÖśņ×ÉļōżņØś ĒÅēĻĘĀ ļéśņØ┤ļŖö 66.0 ┬▒ 15.0ņäĖ(30-86ņäĖ)ņśĆĻ│Ā, ļé©ņ×ÉļŖö 31ļ¬ģ(59.6%)ņØ┤ņŚłļŗż. ĻĖ░ņĀĆņĢłņĢĢņØĆ ņŗ£ņĢ╝Ļ▓░ņåÉņØ┤ ņŗ¼ĒĢ£ ļłłĻ│╝ ļ░śļīĆ ļłł Ļ░üĻ░ü 15.3 ┬▒ 3.5 mmHg (9-21 mmHg), 13.8 ┬▒ 3.2 mmHg (8-20 mmHg)ņ£╝ļĪ£ ņŗ£ņĢ╝Ļ▓░ņåÉņØ┤ ņŗ¼ĒĢ£ ļłłņØ┤ ļŹö ļåÆņĢśļŗż(p<0.001). ĒĢśņ¦Ćļ¦ī, OCT Ļ▓Ćņé¼ ņŗ£ ņĖĪņĀĢĒĢ£ ņĢłņĢĢņØĆ ņŗ£ņĢ╝ Ļ▓░ņåÉņØ┤ ņŗ¼ĒĢ£ ļłłĻ│╝ ļ░śļīĆ ļłł Ļ░üĻ░ü 13.1 ┬▒ 3.3 mmHg (8-19 mmHg), 13.0 ┬▒ 2.8 mmHg (7-20 mmHg)ņ£╝ļĪ£ ļæÉ ļłłņØś ņ░©ņØ┤ļŖö ņŚåņŚłļŗż (p=0.769). ļæÉ ĻĄ░ņØś ņżæņŗ¼Ļ░üļ¦ēļæÉĻ╗ś, ĻĄ¼ļ®┤ļīĆņØæņłśņ╣ś ļ░Å ņĢłņČĢņן ĻĖĖņØ┤ņØś ņ░©ņØ┤ļŖö ņŚåņŚłļŗż(p>0.10). ļæÉ ĻĄ░ņØś ņŗ£ņĢ╝Ļ▓Ćņé¼ MD ņ░©ņØ┤ļŖö 14.41 ┬▒ 5.16 dBļĪ£, ņŗ£ņŗĀĻ▓Į ņåÉņāüņØ┤ ņŗ¼ĒĢ£ ļłłņØ┤ ļ░śļīĆ ļłłĻ│╝ ļ╣äĻĄÉĒĢśņŚ¼ ņŗ£ņĢ╝Ļ▓Ćņé¼ņØś MD Ļ░ÆņØ┤ ļé«Ļ│Ā(-10.68 ┬▒ 6.55 vs. -3.67 ┬▒ 4.05 dB, p<0.001), PSD Ļ░ÆņØĆ ņ╗ĖĻ│Ā(8.26 ┬▒ 3.75 vs. 3.76 ┬▒ 3.04 dB, p<0.001), ļ¦Øļ¦ēņŗĀĻ▓Įņä¼ņ£ĀņĖĄ ļæÉĻ╗śļÅä ņ¢ćņĢśļŗż(65.4 ┬▒ 15.2 vs. 82.5 ┬▒ 15.7 ╬╝m, p<0.001).
LCD ņĖĪņĀĢņŚÉņä£ ļæÉ ņĖĪņĀĢņ×É Ļ░äņØś Bland-Altman 95% ņØ╝ņ╣śļÅä ļ▓öņ£äļŖö -14.7 to 21.1 ╬╝mņśĆļŗż. ĒÅēĻĘĀ LCDļŖö ņŗ£ņŗĀĻ▓Į ņåÉņāüņØ┤ ņŗ¼ĒĢ£ ļłłņØ┤ ļ░śļīĆ ļłłļ│┤ļŗż ņ╗Ėļŗż(529.4 ┬▒ 116.7 vs. 482.9 ┬▒ 107.5 ╬╝m, p<0.001, Fig. 2A). ņśüņŚŁļ│ä ļ╣äĻĄÉņŚÉņä£ļÅä 3Ļ░£ņØś ņĖĪņĀĢ ņ£äņ╣ś ļ¬©ļæÉņŚÉņä£ ņåÉņāüņØ┤ ņŗ¼ĒĢ£ ļłłņØś LCDĻ░Ć ļ░śļīĆ ļłłļ│┤ļŗż ņ╗Ėļŗż(Fig. 2B, Table 2, p<0.002). LCDĻ│╝ Ļ┤ĆļĀ©ļÉ£ ņØĖņ×É ļČäņäØņŚÉņä£ ņŗ£ņŗĀĻ▓Į ņåÉņāüņØ┤ ņŗ¼ĒĢ£ ļłł ĻĘĖļŻ╣Ļ│╝ ļ░śļīĆ ļłł ĻĘĖļŻ╣ ļ¬©ļæÉņŚÉņä£ ĒåĄĻ│äņĀüņ£╝ļĪ£ ņ£ĀņØśĒĢ£ ņĢłņØĖņ×ÉļŖö ņŚåņŚłļŗż(Table 3).
ļŗ©ļ│Ćļ¤ē ņĪ░Ļ▒┤ļČĆ ļĪ£ņ¦ĆņŖżĒŗ▒ ĒÜīĻĘĆļČäņäØņŚÉņä£ LCDĻ░Ć Ēü┤ņłśļĪØ (odds ratio [OR] 1.023, 95% confidence interval [CI] 1.009-1.03, p=0.001), ĻĖ░ņĀĆņĢłņĢĢņØ┤ ļåÆņØäņłśļĪØ(OR 1.752, 95% CI 1.230-2.496, p=0.002) ļģ╣ļé┤ņןņØ┤ ņŗ¼ĒĢĀ ņ£äĒŚśņØ┤ ļåÆņĢśļŗż. ļŗżļ│Ćļ¤ē ņĪ░Ļ▒┤ļČĆ ļĪ£ņ¦ĆņŖżĒŗ▒ ĒÜīĻĘĆļČäņäØņŚÉņä£ļÅä ĻĖ░ņĀĆņĢłņĢĢņØ┤ ļåÆņØäņłśļĪØ(OR 1.758, 95% CI 1.178-2.624, p=0.006), LCDĻ░Ć Ēü┤ņłśļĪØ(OR 1.028, 95% CI 1.009-1.047, p=0.003) ļģ╣ļé┤ņןņØ┤ ņŗ¼ĒĢĀ ņ£äĒŚśņØ┤ ļåÆņĢśļŗż(Table 4). Fig. 3ņØĆ ņ¢æņĢł ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉņŚÉņä£ ņŗ£ņŗĀĻ▓Į ņåÉņāüņØ┤ ņŗ¼ĒĢ£ ļłłņØ┤ ļ░śļīĆ ļłłĻ│╝ ļ╣äĻĄÉĒĢśņŚ¼ LCDĻ░Ć ļŹö Ēü░ Ļ▓āņØä ļ│┤ņŚ¼ņŻ╝ļŖö ļīĆĒæ£ņĀüņØĖ ņ”ØļĪĆņØ┤ļŗż.
Ļ│Ā ņ░░
ņŗ£ņŗĀĻ▓Į ņåÉņāüņØś ņĀĢļÅäĻ░Ć ļŗżļźĖ ņ¢æņĢł ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉņŚÉņä£ ņŗ£ņŗĀĻ▓Į ņåÉņāüņØ┤ ļŹö ņŗ¼ĒĢ£ ļłłņØ┤ ļ░śļīĆ ļłłĻ│╝ ļ╣äĻĄÉĒĢśņŚ¼ LCDĻ░Ć ņ╗Ėļŗż. ļśÉĒĢ£, ļÅÖņØ╝ĒĢ£ ņĀäņŗĀ ņØĖņ×Éļź╝ Ļ░Ćņ¦ä Ļ░£ņØĖ ļé┤ņŚÉņä£ ĻĖ░ņĀĆņĢłņĢĢņØ┤ ļåÆņØäņłśļĪØ, LCDĻ░Ć Ēü┤ņłśļĪØ ņŗ£ņŗĀĻ▓Į ņåÉņāüņØ┤ ļŹö ņŗ¼ĒĢĀ ņ£äĒŚśņØ┤ ļåÆņĢśļŗż. ņØ┤ļŖö ņĢłņĢĢņØ┤ ņĀĢņāü ļ▓öņ£äņØĖ ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņןņŚÉņä£ļÅä ņĢłņĢĢ ļ░Å ņé¼ņāüĒīÉņØś ļ│ĆĒśĢņØ┤ ļģ╣ļé┤ņןņä▒ ņŗ£ņŗĀĻ▓Į ņåÉņāüĻ│╝ Ļ┤ĆļĀ©ņØ┤ ņ׳Ļ│Ā, ļ╣äņŖĘĒĢ£ ņĀäņŗĀ ņĪ░Ļ▒┤ņŚÉņä£ ņĢłņĢĢņØ┤ ļåÆņØäņłśļĪØ, LCDĻ░Ć Ēü┤ņłśļĪØ ņŗ£ņŗĀĻ▓Į ņåÉņāüņØ┤ ļŹö ņŗ¼ĒĢĀ ņ£äĒŚśņØ┤ ļåÆņØä Ļ▓āņ×äņØä ņŗ£ņé¼ĒĢ£ļŗż.
ļ│Ė ņŚ░ĻĄ¼ļŖö ņ¢æņĢłņØś ņżæļō▒ļÅäĻ░Ć ļŗżļźĖ ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉņØś Ļ░£ņØĖ ļé┤ ņ¢æņĢł ļ╣äĻĄÉļź╝ ĒåĄĒĢ┤ ļģ╣ļé┤ņן ņżæļō▒ļÅäņÖĆ Ļ┤ĆļĀ©ļÉ£ ņĢłņØĖņ×Éļź╝ ļČäņäØĒĢśņśĆĻ│Ā ņØ┤ļŖö ļ╣äĻĄÉ ĻĄ░ Ļ░äņØś ņĀäņŗĀ ņØĖņ×Éļź╝ ļ│┤ņĀĢĒĢśņśĆļŗżļŖö ņĖĪļ®┤ņŚÉņä£ Ļ░ĢņĀÉņØ┤ ņ׳ļŗż. Ļ│ĀņĢłņĢĢ ļģ╣ļé┤ņןĻ│╝ ļ╣äĻĄÉĒĢśņŚ¼ ņĢłņĢĢņØ┤ ņĀĢņāü ļ▓öņ£äņŚÉņä£ļÅä ņŗ£ņŗĀĻ▓Į ņåÉņāüņØ┤ ļ░£ņāØĒĢśļŖö ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņןņØĆ ņĀäņŗĀ ĒśłņĢĢ ļ░Å ņŗ£ņŗĀĻ▓ĮņØś ĻĄŁņåī Ļ┤Ćļźś ļČĆņĀä ļō▒ņØś ņŗ£ņŗĀĻ▓ĮņØś ĒŚłĒśłņä▒ ņåÉņāüņØ┤ ļ│æļ”¼ ĻĖ░ņĀäņŚÉ ņżæņÜöĒĢ£ ņŚŁĒĢĀņØä ĒĢĀ Ļ▓āņ£╝ļĪ£ ņČöņĀĢļÉ£ļŗż[5]. ļŗ©ņĢłņØś ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉņŚÉņä£ ļģ╣ļé┤ņן ņĢłņØś ņŗ£ņŗĀĻ▓Įņ£ĀļæÉ ņŻ╝ņ£ä ļ»ĖņäĖ Ļ┤Ćļźś ļČĆņĀäņØś ļ╣łļÅäĻ░Ć ļåÆĻ│Ā, ņŗ£ņŗĀĻ▓Įņ£ĀļæÉ ņŻ╝ņ£ä ņ£äņČĢ(beta zone parapapillary atrophy)ņØ┤ ļŹö ļäōņ£╝ļ®░, ņŗ£ņŗĀĻ▓Įņ£ĀļæÉ ņŻ╝ņ£ä ļ¦źļØĮļ¦ēļæÉĻ╗śļÅä ņ¢ćņĢśļŗż[26]. Lee et al. [15]ņØĆ ņŗ£ņŗĀĻ▓Į ņåÉņāüņØś ņĀĢļÅäĻ░Ć ļ╣äņŖĘĒĢ£ ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉņŚÉņä£ļÅä Ļ░£ļ│äņØś ņé¼ņāüĒīÉ ļ│ĆĒśĢ ļ░Å ņĀäņŗĀ ņ£äĒŚśņØĖņ×ÉĻ░Ć ļŗżņ¢æĒĢ£ ĒŖ╣ņä▒ņØä ļ│┤Ļ│ĀĒĢśņśĆļŗż. ņé¼ņāüĒīÉņØś ļ│ĆĒśĢņØ┤ ļÜ£ļĀĘĒĢśņ¦Ć ņĢŖņØĆ ļģ╣ļé┤ņן ĒÖśņ×ÉļŖö ļ│ĆĒśĢņØ┤ ņŗ¼ĒĢ£ ĒÖśņ×ÉņÖĆ ļ╣äĻĄÉĒĢśņŚ¼ ņ╣śļŻī ņĀä ņĢłņĢĢĻ│╝ ņĀäņŗĀ ĒśłņĢĢņØ┤ ļé«Ļ│Ā, ņŗ£ņŗĀĻ▓Įņ£ĀļæÉ ņŻ╝ņ£ä ņ£äņČĢ ļ░Å ļ»ĖņäĖ Ļ┤Ćļźś ļČĆņĀäņØä ļ│┤ņØ┤Ļ│Ā, ņŗ£ņŗĀĻ▓Į ņ£ĀļæÉ ņŻ╝ņ£ä ļ¦źļØĮļ¦ēļæÉĻ╗śĻ░Ć ņ¢ćņØĆ ĒŖ╣ņä▒ņØä ļ│┤ņśĆļŗż. ņØ┤ļŖö ļ╣äņŖĘĒĢ£ ņŗ£ņŗĀĻ▓Į ņåÉņāüņØä ļ│┤ņØ┤ļŖö ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉņŚÉņä£ļÅä ņŗ£ņŗĀĻ▓Į ņåÉņāüņØ┤ ļ░£ņāØĒĢśļŖö ĻĖ░ņĀäņØ┤ ļŗżļź┤Ļ│Ā, ņé¼ņāüĒīÉņØś ļ│ĆĒśĢ ņĀĢļÅä ņŚŁņŗ£ ļŗżņ¢æĒĢ©ņØä ņŗ£ņé¼ĒĢśĻ│Ā, ņé¼ņāüĒīÉņØś ļ│ĆĒśĢņØ┤ ļŗ©ņł£Ē׳ ļģ╣ļé┤ņןņä▒ ņŗ£ņŗĀĻ▓Į ņåÉņāüņØś Ļ▓░Ļ│╝ļŖö ņĢäļŗÉ Ļ▓āņ×äņØä ņŗ£ņé¼ĒĢ£ļŗż. ņØ┤ļ¤¼ĒĢ£ Ļ┤ĆņĀÉņŚÉņä£ ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉņØś ņŗ£ņŗĀĻ▓Į ņåÉņāüņØś ņ£äĒŚś ņØĖņ×Éļź╝ ļČäņäØĒĢśĻĖ░ ņ£äĒĢ£ Ļ░£ņØĖ Ļ░ä ļ╣äĻĄÉļź╝ ĒåĄĒĢ£ ņŚ░ĻĄ¼ļŖö ĒśłņĢĢ ļō▒ņØś ņĀäņŗĀ ņ£äĒŚśņØĖņ×Éļź╝ ļ│┤ņĀĢĒĢ┤ņĢ╝ ĒĢśņ¦Ćļ¦ī, Ļ░£ļ│ä ĒÖśņ×ÉņØś ļ╣äĻĄÉļŖö ĒśäņŗżņĀüņ£╝ļĪ£ ņĀäņŗĀ ņ£äĒŚśņØĖņ×É ļ│┤ņĀĢņŚÉ ĒĢ£Ļ│äĻ░Ć ņ׳ņØä ņłśļ░¢ņŚÉ ņŚåļŗż.
LCDļŖö ņĢłņĢĢņŚÉ ņØĖĒĢ£ ņé¼ņāüĒīÉņØś ĻĖ░Ļ│äņĀüņØĖ ņåÉņāü ļ░Å ņØ┤ļĪ£ ņØĖĒĢ£ ļ│ĆĒśĢņØä ļ░śņśüĒĢśļŖö ņ¦ĆĒæ£ļĪ£, ļ¦ÄņØĆ ņŚ░ĻĄ¼ļōżņŚÉņä£ LCDņÖĆ ļģ╣ļé┤ņןĻ│╝ņØś ņāüĻ┤Ćņä▒ņØä ĒÖĢņØĖĒĢśņśĆļŗż. Park et al. [17]ņØĆ Ļ│ĀņĢłņĢĢļģ╣ļé┤ņןņØä ĒżĒĢ©ĒĢ£ Ļ░£ļ░®Ļ░üļģ╣ļé┤ņן ĒÖśņ×Éļź╝ ļīĆņāüņ£╝ļĪ£ ļČäņäØĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ ņä▒ļ│äĻ│╝ ņŚ░ļĀ╣ņØ┤ ļÅÖņØ╝ĒĢ£ ļČäĒżļź╝ Ļ░Ćņ¦ä Ļ░£ļ░®Ļ░üļģ╣ļé┤ņן ĒÖśņ×É ĻĘĖļŻ╣ņŚÉņä£ ņŗ£ņŗĀĻ▓Į ņåÉņāüņØ┤ ļŹö ņŗ¼ĒĢ£ ĒÖśņ×ÉņØś LCDĻ░Ć ļŹö Ēü¼ļŗżĻ│Ā ĒĢśņśĆļŗż. Kim et al. [27]ņØĆ ļŗ©ņĢłņØś Ļ░£ļ░®Ļ░üļģ╣ļé┤ņן ĒÖśņ×ÉņŚÉņä£ ņŗ£ņĢ╝Ļ▓░ņåÉņØ┤ ņ׳ļŖö ļłł ļ┐Éļ¦ī ņĢäļŗłļØ╝ ļ░śļīĆņĢłņŚÉņä£ļÅä LCDĻ░Ć ņĀĢņāüņØĖĻ│╝ ļ╣äĻĄÉĒĢśņŚ¼ Ēü¼ļŗżĻ│Ā ĒĢśņśĆļŗż. ļ│Ė ņŚ░ĻĄ¼ļŖö ņ╣śļŻī ņĀä ņĢłņĢĢņØ┤ ņĀĢņāü ļ▓öņ£äņØĖ ņ¢æņĢł ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉņŚÉņä£ ņŗ£ņŗĀĻ▓Į ņåÉņāüņØś ņżæļō▒ļÅäņŚÉ ļö░ļØ╝ ļæÉ ĻĄ░ņ£╝ļĪ£ ļéśļłäņ¢┤ Ļ░£ņØĖ ļé┤ ņ¢æņĢłņØś LCDļź╝ ļ╣äĻĄÉĒĢśņśĆļŗż. ļ│Ė ņŚ░ĻĄ¼ņŚÉ ĒżĒĢ©ļÉ£ ĒÖśņ×ÉļōżņØś LCDļŖö ņŗ£ņŗĀĻ▓Į ņåÉņāüņØ┤ ļŹö ņŗ¼ĒĢ£ ļłł(529.4 ┬▒ 116.7 ╬╝m)Ļ│╝ ļ░śļīĆ ļłł(482.9 ┬▒ 107.5 ╬╝m) ļ¬©ļæÉ Ļ▒┤Ļ░ĢĒĢ£ ĒĢ£ĻĄŁ ņä▒ņØĖņØś LCD (402.06 ┬▒ 101.46 ╬╝m) [25]ļ│┤ļŗż Ēü░ Ļ▓ĮĒ¢źņØä ļ│┤ņśĆĻ│Ā, ļģ╣ļé┤ņןņØ┤ ņŗ¼ĒĢ£ ļłłņØś LCDĻ░Ć ļ░śļīĆ ļłłĻ│╝ ļ╣äĻĄÉĒĢśņŚ¼ ļŹö ņ╗Ėļŗż. ņØ┤ļŖö ļŗ©ņĢłņØś ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉņŚÉņä£ ļģ╣ļé┤ņןņĢłņØś LCDĻ░Ć ņĀĢņāüņĢłņØś LCDļ│┤ļŗż ļŹö ņ╗ĖļŹś ĻĖ░ņĪ┤ ņŚ░ĻĄ¼[5]ņØś Ļ▓░Ļ│╝ņÖĆļÅä ņāüņØæĒĢśļ®░, Ļ│ĀņĢłņĢĢ ļģ╣ļé┤ņן ļ┐Éļ¦ī ņĢäļŗłļØ╝ ņĢłņĢĢņØ┤ ņĀĢņāü ļ▓öņ£äņØĖ ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉņŚÉņä£ļÅä ņé¼ņāüĒīÉņØś ļ│ĆĒśĢņØ┤ ņŗ£ņŗĀĻ▓Į ņåÉņāüĻ│╝ Ļ┤ĆļĀ©ņØ┤ ņ׳ņØä Ļ▓āņ×äņØä ņŗ£ņé¼ĒĢ£ļŗż.
Ļ│ĀņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×Éļź╝ ĒżĒĢ©ĒĢ£ Ļ░£ļ░®Ļ░üļģ╣ļé┤ņן ĒÖśņ×É(ņĢłņĢĢ ļ▓öņ£ä 12-55 mmHg)ņŚÉņä£ ņĢłņĢĢĻ│╝ LCDļŖö ņ¢æņØś ņāüĻ┤Ćņä▒ņØä ļ│┤ņśĆĻ│Ā[28], ņłśņłĀņĀü ņ╣śļŻīļź╝ ĒåĄĒĢ┤ ņä▒Ļ│ĄņĀüņ£╝ļĪ£ ņĢłņĢĢņØ┤ ĒĢśĻ░ĢļÉ£ ĒÖśņ×É(ņłśņłĀ ņĀä ņĢłņĢĢ 27.4 ┬▒ 9.0 mmHg, ņłśņłĀ 6Ļ░£ņøö Ēøä ņĢłņĢĢ 9.7 ┬▒ 3.1 mmHg)ņŚÉņä£ ņłśņłĀ Ēøä LCDņØś Ļ░Éņåīļź╝ ĒÖĢņØĖĒĢĀ ņłś ņ׳ņŚłņ£╝ļ®░, LCD Ļ░ÉņåīļŖö ņĢłņĢĢĒĢśĻ░Ģ ņĀĢļÅäņÖĆ ņ¢æņØś ņāüĻ┤Ćņä▒ņØä ļ│┤ņśĆļŗż[29]. ĻĘĖļ¤¼ļéś ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉņŚÉņä£ļŖö ņĢłņĢĢĒĢśĻ░Ģ ņĀĢļÅäņÖĆ ņé¼ņāüĒīÉņØś ļ│ĆĒśĢ ņĀĢļÅäļŖö ņ£ĀņØśĒĢ£ ņāüĻ┤Ćņä▒ņØ┤ ņŚåņŚłļŗż[30]. ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ļÅä Ļ│ĀņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉņÖĆ ļŗ¼ļ”¼, ņĢłņĢĢĻ│╝ LCD Ļ░äņØś ņāüĻ┤Ćņä▒ņØĆ ĒÖĢņØĖļÉśņ¦Ć ņĢŖņĢśļŗż. ņØ┤ļŖö ļ│Ė ņŚ░ĻĄ¼Ļ░Ć ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×Éļ¦īņØä ļīĆņāüņ£╝ļĪ£ ļČäņäØĒĢśņśĆĻĖ░ ļĢīļ¼ĖņŚÉ, ĒżĒĢ©ļÉ£ ĒÖśņ×ÉļōżņØś ņĢłņĢĢ ļ▓öņ£äĻ░Ć ņóüņĢäņä£ ņĢłņĢĢĻ│╝ LCD ņé¼ņØ┤ņŚÉ ņ£ĀņØśĒĢ£ ņāüĻ┤ĆņØ┤ ĒÖĢņØĖļÉśņ¦Ć ņĢŖņØĆ Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż.
ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ ļæÉ ļłł ņżæņŚÉ LCDĻ░Ć Ēü¼Ļ│Ā, ĻĖ░ņĀĆņĢłņĢĢņØ┤ ļåÆņØĆ ļłłņŚÉņä£ ļģ╣ļé┤ņןņØ┤ ņŗ¼ĒĢĀ ņ£äĒŚśņØ┤ ļåÆņĢśļŗż. ņØ┤ļŖö ļŗ©ņĢł ņĀĢņāüņĢłņĢĢ ļģ╣ļé┤ņן ĒÖśņ×ÉņŚÉņä£ ņé¼ņāüĒīÉ ļ│ĆĒśĢņØ┤ Ēü░ ļłłņŚÉņä£ ļģ╣ļé┤ņן ļ░£ļ│æņØś ņ£äĒŚśņØ┤ ļåÆņĢśļŹś ĻĖ░ņĪ┤ ņŚ░ĻĄ¼ņÖĆ ņāüņØæĒĢśļŖö Ļ▓░Ļ│╝ļĪ£[5], ņĢłņĢĢņØ┤ ņĀĢņāü ļ▓öņ£äņØĖ ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņןņŚÉņä£ļÅä ņé¼ņāüĒīÉņØś Ēøäļ░® ļ│ĆĒśĢņØ┤ ļģ╣ļé┤ņןņä▒ ņŗ£ņŗĀĻ▓Į ņåÉņāüĻ│╝ Ļ┤ĆļĀ©ņØ┤ ņ׳ņØīņØä ņŗ£ņé¼ĒĢ£ļŗż.
ļ│Ė ņŚ░ĻĄ¼ļŖö ļŗ©ļ®┤ ņŚ░ĻĄ¼ļĪ£, ņé¼ņāüĒīÉņØś ĒśĢĒā£ņÖĆ ņŗ£ņŗĀĻ▓Į ņåÉņāüņØś ļ¬ģĒÖĢĒĢ£ ņØĖĻ│╝Ļ┤ĆĻ│ä ĻĘ£ļ¬ģņŚÉļŖö ĒĢ£Ļ│äĻ░Ć ņ׳ņ¦Ćļ¦ī, ļŗżņØīĻ│╝ Ļ░ÖņØ┤ ņé¼ņāüĒīÉņØś ĒśĢĒā£ņÖĆ ļģ╣ļé┤ņןņä▒ ņŗ£ņŗĀĻ▓Į ņåÉņāüņØś ņāüĻ┤Ćņä▒ņØä ņČöņĀĢĒĢ┤ ļ│╝ ņłś ņ׳ņØä Ļ▓āņØ┤ļŗż. ņ▓½ ļ▓łņ¦Ė, ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņןņŚÉņä£ LCDĻ░Ć Ēü┤ņłśļĪØ ņśłĒøäĻ░Ć ļéśņüĀ Ļ▓āņØ┤ļØ╝ļŖö Ļ░ĆņäżņØ┤ļŗż. ļæÉ ļ▓łņ¦ĖļŖö ņé¼ņāüĒīÉņØś Ēøäļ░® ļ│ĆĒśĢņØ┤ ļģ╣ļé┤ņןņä▒ ņŗ£ņŗĀĻ▓Į ņåÉņāüņŚÉ ļö░ļźĖ ņØ┤ņ░©ņĀüņØĖ ļ│ĆĒÖöļØ╝ļŖö Ļ▓āņØ┤ļŗż. ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ LCDļŖö ņŗ£ņŗĀĻ▓Į ņåÉņāüņØ┤ ņŗ¼ĒĢ£ ļłłņŚÉņä£ ļŹö ņ╗Ėņ¦Ćļ¦ī, ņŗ£ņŗĀĻ▓Į ņåÉņāüņØ┤ ņŗ¼ĒĢ£ ļłł ĻĘĖļŻ╣Ļ│╝ ļ░śļīĆ ļłł ĻĘĖļŻ╣ ļé┤ņŚÉņä£ LCDņÖĆ ņŗ£ņŗĀĻ▓Į ņåÉņāüņØś ņĀĢļÅä(retinal nerve fiber layer [RNFL] thickness and visual field indices) Ļ░äņØś ņāüĻ┤Ćņä▒ņØĆ Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśļŗż. ņØ┤ļŖö ļŗ©ņł£Ē׳ RNFL ņåÉņŗżņØ┤ ņé¼ņāüĒīÉņØś ļ│ĆĒśĢņØä ņ£Āļ░£Ē¢łņØä Ļ░ĆļŖźņä▒ņØĆ ļé«ļŗżļŖö Ļ▓āņØä ņäżļ¬ģĒĢśļŖö Ļ▓░Ļ│╝ņØ┤ļŗż. ĻĖ░ņĪ┤ņØś ļģ╣ļé┤ņן ļÅÖļ¼╝ ņŗżĒŚś ļ¬©ļŹĖņŚÉņä£ ņé¼ņāüĒīÉņØś ļ│ĆĒśĢņØ┤ RNFL ņåÉņŗżļ│┤ļŗż ļ©╝ņĀĆ ļ░£ņāØĒĢśĻ│Ā[31], ļ╣äļģ╣ļé┤ņןņä▒ ņŗ£ņŗĀĻ▓Įļ│æņ”Ø ĒÖśņ×ÉņØś ņé¼ņāüĒīÉņØ┤ ņĀĢņāüņØĖĻ│╝ ļ╣äĻĄÉĒĢśņŚ¼ ĒśĢĒā£ĒĢÖņĀü ņ░©ņØ┤Ļ░Ć ņŚåņŚłļŹś ņŚ░ĻĄ¼ Ļ▓░Ļ│╝[32-34] ņŚŁņŗ£ ņé¼ņāüĒīÉņØś ļ│ĆĒśĢņØ┤ ņŗ£ņŗĀĻ▓Į ņåÉņāüņŚÉ ļö░ļźĖ ņØ┤ņ░©ņĀüņØĖ Ļ▓░Ļ│╝ļØ╝ļŖö Ļ▓āņŚÉļŖö ĒĢ£Ļ│äĻ░Ć ņ׳ņØīņØä ņŗ£ņé¼ĒĢ£ļŗż. ĒĢśņ¦Ćļ¦ī ļ│Ė ņŚ░ĻĄ¼ļŖö ļŗ©ļ®┤ ņŚ░ĻĄ¼ņØ┤ĻĖ░ ļĢīļ¼ĖņŚÉ ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉņŚÉņä£ ņŗ£ņŗĀĻ▓Į ņåÉņāüĻ│╝ ņé¼ņāüĒīÉ ļ│ĆĒśĢņØś ņØĖĻ│╝Ļ┤ĆĻ│äļź╝ ĻĘ£ļ¬ģĒĢśĻĖ░ ņ£äĒĢ┤ņä£ļŖö ņןĻĖ░ņĀüņØĖ ņŚ░ĻĄ¼Ļ░Ć ĒĢäņÜöĒĢĀ Ļ▓āņ£╝ļĪ£ ņé¼ļŻīļÉ£ļŗż.
ļ│Ė ņŚ░ĻĄ¼ļŖö ļŗżņØīĻ│╝ Ļ░ÖņØĆ ĒĢ£Ļ│äņĀÉņØ┤ ņ׳ļŗż. ņ▓½ ļ▓łņ¦ĖļĪ£ ĒÖśņ×ÉļōżņØś ņØśļ¼┤ĻĖ░ļĪØņØä ĒøäĒ¢źņĀüņ£╝ļĪ£ ļČäņäØĒĢ£ ļŗ©ļ®┤ ņŚ░ĻĄ¼ļĪ£ LCDĻ░Ć Ēü░ ļłłņØ┤ ļģ╣ļé┤ņןņä▒ ņŗ£ņŗĀĻ▓Į ņåÉņāüņŚÉ ļŹö ņĘ©ņĢĮĒĢ£ Ļ▓āņØĖņ¦Ć, ļģ╣ļé┤ņןņä▒ ņŗ£ņŗĀĻ▓Į ņåÉņāüņØ┤ ļŹö Ēü░ ļłłņŚÉņä£ ņØ┤ņ░©ņĀüņ£╝ļĪ£ LCDĻ░Ć ņ╗żņ¦ä Ļ▓āņØĖņ¦Ć ņØĖĻ│╝Ļ┤ĆĻ│äļź╝ ļ¬ģĒÖĢĒ׳ ĻĘ£ļ¬ģĒĢśĻĖ░ ņ¢┤ļĀĄļŗż. ņØ┤ļ¤¼ĒĢ£ ĒĢ£Ļ│äņĀÉņØä ĻĘ╣ļ│ĄĒĢśĻĖ░ ņ£äĒĢ┤ņä£ļŖö ņČöĒøä ņןĻĖ░ņĀüņØĖ ņČöņĀü Ļ┤Ćņ░░ņØä ĒåĄĒĢ£ ņØĖĻ│╝Ļ┤ĆĻ│äņØś ĒÖĢņØĖņØ┤ ĒĢäņÜöĒĢĀ Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż. ļæÉ ļ▓łņ¦ĖļĪ£ ļ╣øĻ░äņäŁļŗ©ņĖĄņ┤¼ņśüņłĀ ĻĖ░Ļ│äņŚÉļŖö ņĢäņ¦ü LCDļź╝ ņ×ÉļÅÖņ£╝ļĪ£ ņĖĪņĀĢĒĢśļŖö ņåīĒöäĒŖĖņø©ņ¢┤Ļ░Ć Ēāæņ×¼ļÉśņ¢┤ ņ׳ņ¦Ć ņĢŖņĢä ņłśļÅÖņ£╝ļĪ£ ņĖĪņĀĢĒĢ┤ņĢ╝ ĒĢśļ»ĆļĪ£, ņĖĪņĀĢņ×ÉņŚÉ ļö░ļźĖ ņśżņ░©Ļ░Ć ļ░£ņāØĒĢĀ ņłś ņ׳ļŗż. ĻĘĖļ¤¼ļéś ļ│Ė ņŚ░ĻĄ¼ņØś ņĖĪņĀĢņ×É Ļ░ä Bland-Altman ņØ╝ņ╣śļÅä ļČäņäØ Ļ▓░Ļ│╝ņŚÉņä£ 95% ņØ╝ņ╣śļÅä ļ▓öņ£äļŖö -14.7 to 21.1 ╬╝mļĪ£ ļåÆņØĆ ņØ╝ņ╣śņ£©ņØä ļ│┤ņśĆĻ│Ā, ņåÉņāüņØ┤ ņŗ¼ĒĢ£ ļłłĻ│╝ ļ░śļīĆ ļłłņØś LCDņØś ņ░©ņØ┤(46.0 ┬▒ 63.0 ╬╝m)ļŖö ņĖĪņĀĢ ņśżņ░©ļź╝ ļäśĻĖ░ ļĢīļ¼ĖņŚÉ, ņĖĪņĀĢ ņśżņ░©Ļ░Ć ļ│Ė ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ņŚÉ Ēü░ ņśüĒ¢źņØä ļ»Ėņ╣śņ¦Ć ņĢŖņĢśņØä Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż. ļ¦łņ¦Ćļ¦ēņ£╝ļĪ£, ļ│Ė ņŚ░ĻĄ¼ļŖö ņĢłņĢĢĒĢśĻ░Ģ ņ╣śļŻī ņżæņØĖ ĒÖśņ×ÉĻ░Ć ĒżĒĢ©ļÉśņŚłĻĖ░ ļĢīļ¼ĖņŚÉ, LCDĻ░Ć ņĢłņĢĢĒĢśĻ░Ģ ņ╣śļŻīļĪ£ Ļ░ÉņåīļÉśņŚłņØä Ļ░ĆļŖźņä▒ņØ┤ ņ׳ļŗż[30,35]. ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ ņŗ£ņŗĀĻ▓Į ņåÉņāüņØ┤ ņŗ¼ĒĢ£ ļłłņØ┤ ļ░śļīĆ ļłłļ│┤ļŗż, LCDĻ░Ć ļŹö Ēü¼Ļ│Ā, ņĢłņĢĢĒĢśĻ░Ģ ņĀĢļÅäļÅä ļŹö ņ╗Ėļŗż. ņØ┤ļŖö ņ╣śļŻī ņĀä LCD ņŚŁņŗ£, ļģ╣ļé┤ņןņØ┤ ņŗ¼ĒĢ£ ļłłņØ┤ ļ░śļīĆ ļłłĻ│╝ ļ╣äĻĄÉĒĢ┤ņä£ ļŹö ņ╗ĖņØä Ļ▓āņ£╝ļĪ£ ņČöņĀĢĒĢĀ ņłś ņ׳ĻĖ░ņŚÉ, ņĢłņĢĢĒĢśĻ░Ģ ņ╣śļŻīĻ░Ć ļ│Ė ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ņŚÉ Ēü░ ņśüĒ¢źņØä ļ»Ėņ│żņØä Ļ░ĆļŖźņä▒ņØĆ ņĀüņØä Ļ▓āņØ┤ļŗż.
Ļ▓░ļĪĀņĀüņ£╝ļĪ£, ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņ¢æņĢł ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņן ĒÖśņ×ÉņŚÉņä£ ļģ╣ļé┤ņןņä▒ ņŗ£ņŗĀĻ▓Į ņåÉņāüņØ┤ ļŹö ņŗ¼ĒĢ£ ļłłņØ┤ ļ░śļīĆ ļłłĻ│╝ ļ╣äĻĄÉĒĢśņŚ¼ LCDĻ░Ć ļŹö ņ╗ĖĻ│Ā, LCDĻ░Ć Ēü░ ļłłņØ┤ ļ░śļīĆ ļłłĻ│╝ ļ╣äĻĄÉĒĢśņŚ¼ ņŗ£ņŗĀĻ▓Į ņåÉņāüņØ┤ ņŗ¼ĒĢĀ ņ£äĒŚśņØ┤ ļåÆņĢśļŗż. ņØ┤ļŖö ĻĖ░ņĀĆņĢłņĢĢņØ┤ ņĀĢņāü ļ▓öņ£äņØĖ ņĀĢņāüņĢłņĢĢļģ╣ļé┤ņןņŚÉņä£ļÅä ņé¼ņāüĒīÉņØś ļ│ĆĒśĢņØ┤ ņŗ£ņŗĀĻ▓Į ņåÉņāüĻ│╝ Ļ┤ĆļĀ©ņØ┤ ņ׳ņØīņØä ņŗ£ņé¼ĒĢ£ļŗż.



 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






