

실리콘기름은 생체 내에서 흡수되거나 분해되지 않아 오랜 기간 동안 유리체강 내 충전물을 유지해야 할 필요성이 있는 유리체절제술에서 유용하다고 알려져 있다. 최근 미세수술의 기술적 혁신과 더불어 실리콘기름은 증식유리체망막병증과 거대열공을 동반한 복잡한 열공망막박리의 수술에 이용된다[1-3]. 투명도가 있는 광학적 특성으로 인해 오랜 시간 동안 안구 내 충전물로 유지할 수 있고, 수술 후 안구 내 상태를 파악하는 것도 가능하다. 그러나 실리콘기름은 백내장, 각막병증, 망막전막, 안압상승과 관련된 이차녹내장 등 몇몇 합병증과도 관련이 있다[4-8]. 게다가, 합병증 없이 성공적으로 유리체절제술을 시행하였음에도 불구하고 안내 실리콘기름 충전물과 관련되어 수술 후 시력예후가 나빴던 증례도 있다[9-11]. 내망막층 두께의 의미 있는 감소는 황반부 신경세포의 손실을 의미하고, 실리콘기름충전술이 심각한 시력손실과 연관성이 있는 것으로 발표된 연구도 있다[12,13]. 다른 보고에서는, 열공망막박리에서 안내 실리콘기름충전술로 재유착된 망막의 망막신경섬유층이 대조군으로 설정한 반대안에 비해 의미 있게 두꺼웠다는 연구도 있었다[14].
실리콘기름이 망막층의 두께 및 시력 등에 미치는 영향을 알아보기 위하여, 본 연구에서는 유리체 충전물로써 실리콘기름 주입 후 1주, 2주, 2개월 및 실리콘기름 제거 후 2개월째 망막층의 두께 변화를 파장가변광원 빛간섭단층촬영 영상을 사용하여 분석하였다.
대상과 방법
본 연구는 울산대학교병원 기관생명윤리위원회(Institutional Review Board, IRB)에서 검토 및 승인을 받았으며(승인 번호: UUH 2020-10-009), 헬싱키선언(Declaration of Helsinki)의 윤리 지침을 준수하였다. 또한 2016년 1월 1일부터 2017년 3월 31일까지 울산대학교병원 안과에서 열공망막박리로 수술 치료를 받은 24명의 24안과 안내이물로 수술 치료를 받은 4명 4안에 대한 후향적 연구이다. 최근 발병한 열공망막박리 및 안내이물 환자에서 단일 수술(유리체절제술 및 실리콘기름충전술)로 합병증 없이 성공적으로 치료된 환자들만 연구 대상으로 선정되었다. 이전에 백내장수술이나, 망막전막, 황반원공, 열공망막박리 등으로 인한 망막수술 등 안과적 수술을 받은 환자들은 연구 대상에서 제외되었다. 또한 안축장이 26.5 mm 이상인 고도근시나, 기존 시력에 영향을 미치는 것으로 알려져 있는 녹내장, 포도막염, 망막혈관질환, 심각한 매체혼탁 등의 안구질환이 있는 환자들 또한 연구 대상에서 제외했다. 그리고 실리콘기름주입술 후 경과 관찰 도중 망막전막, 낭포황반부종 등이 생긴 환자들도 연구 대상에서 제외하였다. 모든 환자는 EVA 유리체절제술 기구(DORC Dutch Ophthalmic Research Center International BV, Zuidland, The Netherlands)를 이용하여, 표준적인 3개의 투관침을 이용한 25게이지 유리체절제술을 시행 받았다. 액체공기교환술 후 실리콘기름(Arciolane 5500, Arcadophta, Toulouse, France)을 주입하였으며 공막절개부를 봉합하였다. 또한 모든 환자에서 수정체유화술 및 후방인공수정체삽입술을 시행하였다. 실리콘기름 제거 시행 시 추가적으로 시행한 수술은 없었다. 모든 수술은 한 명의 망막 수술의가 집도하였다.
의무 기록을 통해 모든 환자들의 수술 전후의 최대교정시력과 안압을 확인하였으며, 수술 후 1주, 2주, 2개월 및 실리콘기름 제거 후 2개월 시점 및 정상 반대안의 파장가변 빛간섭단층촬영(DRI OCT-1, Atlantis; Topcon Corp., Tokyo, Japan) 삼차원 광각 촬영 영상을 이용하여 Early treatment Diabetic Retinopathy Study (ETDRS) subfield에 서 망막전층, 망막신경섬유층 및 신경절세포-내망상층의 두께를 측정하였다. 망막의 각 층별 구분은 내장된 프로그램에서 자동으로 시행하였다[15]. 모든 빛간섭단층촬영 영상은 한 명의 망막 전문의가 분석하였으며, 망막층의 구분이 적절하게 나누어지고 영상이 적합한 해상도와 품질을 가지고 있는지 검토하였다. 망막층 구분이 적절하게 이루어지지 않은 경우 오류를 교정하기 위해 반자동 분석을 추가로 시행하였다(Fig. 1).
통계 분석은 SPSS 통계 소프트웨어 프로그램(version 18 for Windows, IBM Corp., Armonk, NY, USA)으로 시행했다. Friedman test 및 Wilcoxon signed rank test을 사용하여 실리콘기름 충전 기간에 따른 변화와 제거 전후 정량적인 수치 차이를 비교하였으며, Mann-Whitney U test을 이용하여 실리콘기름 제거 2주 후의 망막층 두께와 반대안의 망막층 두께를 비교하였다. 연속적인 변수는 평균 ± 표준편차로 나타내었다. p값의 유의 수준은 0.05 미만으로 하였다.
결 과
총 28명의 연구 대상자(남성 24명, 여성 4명)가 본 연구에 포함되었으며 이들의 평균 연령은 50.1 ± 10.3세였다. 열공망막박리 환자 24안 중 8안에서는 망막박리가 황반부를 침범하지 않았고 16안에서는 침범하였다. 4안의 안구 내 이물 환자 모두에서 ETDRS subfield 안에서 황반부 손상은 없었다. 환자군의 수술 전 평균 최대교정시력(logarithm of minimal angle of resolution, logMAR)은 0.74 ± 0.71이었고, 실리콘기름 제거 후 2개월 시점에서 0.21 ± 0.26으로 유의하게 증가하였다(p<0.001). 초진 시 측정한 반대안의 최대교정시력은 0.05 ± 0.10이었다. 안압은 수술 이전에 16.3 ± 2.3 mmHg였으며 실리콘기름 제거 후 2개월 시점에서 16.5 ± 2.0 mmHg로 통계적으로 유의한 차이는 보이지 않았다. 실리콘기름 충전물이 삽입되어 있던 평균 기간은 2.43 ± 0.57개월이었다(Table 1).
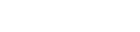
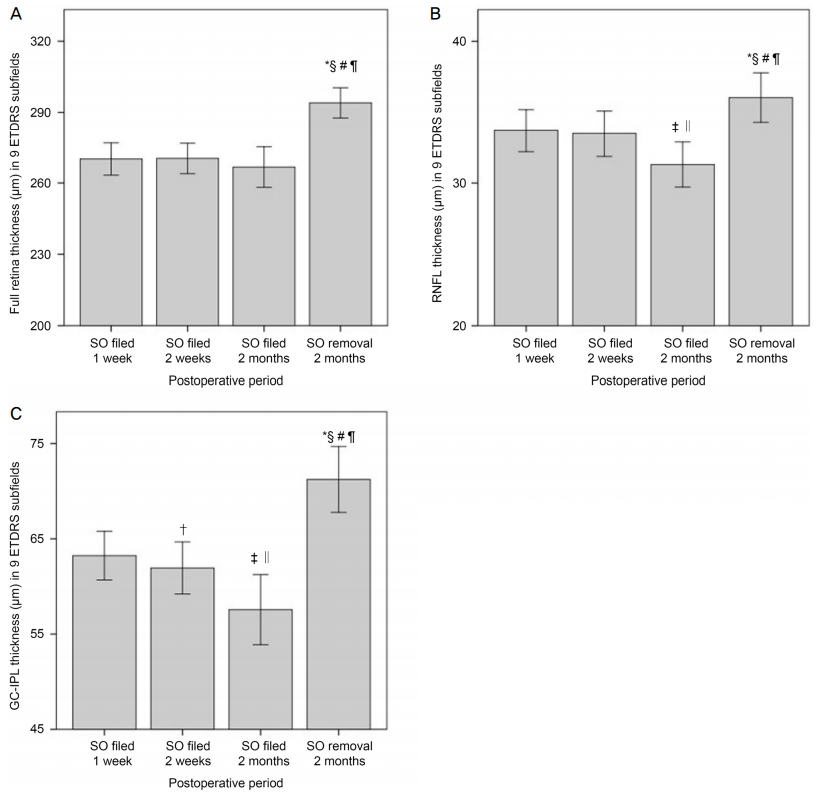
ETDRS subfields에서의 평균 망막전층 두께는 실리콘기름 충전 기간 1주, 2주 및 2개월 시점에서 통계적으로 유의한 차이를 보이지 않았다. 그러나 망막신경섬유층에서는 실리콘기름 충전 기간 2개월째에서 1주 및 2주 시점과 비교 시 유의한 두께 감소를 보였다. 또한 신경절세포-내망상층의 경우는 실리콘기름 충전이 기간이 증가함에 따라 1주와 비교 시 2주 및 1, 2주 모두에 비하여 2개월 시점에서 유의한 두께 감소를 보였다. 실리콘기름 제거 후 2개월 시점에서 시행한 빛간섭단층촬영검사에서 망막전층, 망막신경섬유층 및 망막신경절세포-내망상층 모두 실리콘기름 충전 중과 비교 시 유의하게 두께 증가가 관찰되었다(Table 2, Fig. 2).
대조군으로는 대상자들의 정상 반대안(26명 26안)을 사용하여 망막층의 두께를 측정하여 비교 분석하였다. 반대안에 망막전막이 있는 1명과 추적 관찰 기간 동안 반대안의 빛간섭단층촬영 영상이 없는 1명은 제외하였다(Table 3).
고 찰
실리콘기름은 유리체, 망막수술에서 안내 충전물로 많이 쓰이는 물질 중 하나이다. 안내충전물은 합병증이 동반된 열공망막박리에서 성공적인 수술을 위해 필수적이다. 그러나 실리콘기름의 중요한 역할에도 불구하고, 실리콘기름충전물로 인하여 발생한, 설명되지 않는 시력손실이 보고된 바 있다[9-12]. Christensen and la Cour [12]은 실리콘기름충전술을 시행한 눈(8안)과 가스 충전술을 시행한 눈(7안)의 망막층 두께 감소를 측정하였고, 망막층의 얇아짐과 시력감소가 어느 정도 상관관계가 있다는 것을 밝혀냈다. 그러나 망막층의 각 층별 두께를 분석하지 못했고 표본 수가 적어서 개인의 망막층에서 두께 변화가 어떻게 일어나는지 정확하게 측정하지 못하였다. Caramoy et al [16]은 실리콘기름충전술을 시행한 눈과 정상 반대안을 비교하였지만, 실리콘기름충전술을 시행한 눈에서 실리콘기름을 제거한 후의 망막층 두께 변화를 측정하지 않았다[16]. Zoric Geber et al [14]은 열공망막박리 환자에서 망막박리가 없는 반대안의 시신경유두 주변부의 시신경섬유층이 실리콘기름 충전물이 삽입된 눈보다 더 두껍다는 것을 보고하였다[14]. Lo et al [17]은 실리콘기름 충전물이 삽입되어 있는 동안 황반부두께가 전체적으로 얇아지지만, 이는 실리콘기름 충전물을 제거한 뒤 회복됨을 보고하였다.
실리콘기름은 실리콘기름 방울 자체의 기계적 부하와 망막층, 망막색소상피층에 대한 독성 반응 등의 기전으로 망막손상을 일으킬 수 있는 것으로 알려져 있다[14-17]. Wickham et al [18]은 실리콘기름 충전물이 들어있는 눈을 적출하였을 때, 실리콘기름 방울이 망막을 포함한 안구 조직 내로 침범하여 대식세포에 의해 매개되는 염증반응을 일으킬 수 있음을 발표했다. 실리콘기름충전술을 시행한 눈에서 망막두께가 얇아지는 것은 충전물이 망막에 기계적인 압력을 주기 때문인 것이라는 가설이 있다[17]. 빛간섭단층촬영을 이용한 연구들은 실리콘기름충전술을 시행 받은 안구에서 시력손실이 망막층 두께가 얇아지고, 망막중심오목무혈관부위(foveal avascular zone) 변화와 관련이 있다고 보고한 바 있다[19].
본 연구의 결과에서도 실리콘기름이 충전되었을 때가 제거한 때보다 망막전층의 두께가 얇아진 것을 확인할 수 있으며, 특히 신경절세포-내망상층의 두께 변화 폭이 큰 것을 확인하였다. 본 연구에서는 실리콘기름을 제거한 후 망막층의 두께가 다시 회복하는 것을 확인할 수 있었고, 따라서 실리콘기름에 의해 감소된 망막두께는 가역적인 것으로 생각된다. 수술안의 망막층 두께를 수술 전에 측정한 결과가 있다면 보다 직접적인 비교가 가능했겠으나, 황반부를 침범한 망막박리 환자에서는 망막두께의 정확한 측정이 어렵기 때문에 정상 반대안의 망막층 두께 평균을 측정해 비교하였으며, 정상 반대안 망막층의 층별 두께와 실리콘기름 제거 후 2개월 시점에서의 망막층별 두께는 유의한 차이가 없었다(Table 3). 또한 실리콘기름 제거 후 최대교정시력 또한 회복되는 것을 확인할 수 있었는데, 이는 실리콘기름제거 후에 실리콘기름으로 인한 굴절력 차이가 사라지며 시력상승에 영향을 주었을 가능성도 있다. 수술 전 대상자의 백내장을 평가한 기록은 없지만, 대상자의 평균 연령이 50.1세이며, 기존에 수술안의 안질환은 가지고 있지 않았으며, 반대안의 평균 최대교정시력(logMAR)이 0.05로 좋은 시력을 가지고 있었음을 미루어 볼 때 수술안의 백내장수술에 의한 시력향상은 미미할 것으로 생각된다. 빛간섭단층촬영을 이용한 기존 연구들에서도 실리콘기름을 충전한 눈에서 설명되지 않는 황반부두께 감소나 황반부종이 발생하는 경우 실리콘기름을 제거하는 것으로 이러한 미세구조가 복구될 수 있다고 보고한 바도 있다[17,20]. 그러나 본 연구에서 망막신경섬유층 및 망막신경절세포-내망상층에서와 같이 실리콘기름 충전 기간이 지속될수록 두께 감소가 진행되는 것을 보아, 3개월 이상의 장기적인 실리콘기름의 충전으로 인해 망막층 두께의 변화폭이 계속해서 더 커지거나, 비가역적인 손상으로 이행되는지에 대한 여부는 추가적인 연구가 더 필요할 것으로 생각된다.
본 연구의 제한점으로는 단일기관 내의 연구로 연구 대상이 단일 병원에 내원한 환자군에 한정되었으며, 환자군의 분석을 후향적으로 시행한 점이 있다. 열공망막박리 환자의 경우 황반을 침범한 안과 침범하지 않은 안이 함께 분석에 포함되었으며, 특히 황반을 침범한 열공망막박리 환자군은 수술 전 시력이 이미 많이 저하되어 있는 상황으로, 실리콘기름을 제거하고 나서 시력호전이 유의하게 일어났는지 정확한 평가를 내리기 어려운 면도 있었다. 또한 수술 전 망막층의 두께를 측정할 수 없어 수술 전 시점과 실리콘기름 제거 후 시점의 직접적인 비교를 시행하지 못하였으며, 대조군인 정상 반대안의 망막층의 두께를 측정해 간접적으로 비교하였다. 그리고 망막층의 두께 변화가 망막박리로 인한 변화인지 실리콘기름에 의한 변화인지에 대해 추후 추가적인 연구도 필요할 것으로 생각된다. 실리콘기름의 경우 본 연구에서는 5,500 cs 단위의 실리콘기름만을 사용하였다. 따라서 낮은 점도의 실리콘기름 경우는 다른 결과를 보일 수 있어 본 연구 결과 해석에 주의가 필요할 수 있다.
결론적으로, 본 연구에서는 실리콘기름 충전 후 1주 및 2개월의 시점에서 망막전층의 두께는 유의하게 감소하지는 않았으나, 망막신경섬유층 및 망막신경절세포-내망상층에서의 두께가 유의하게 감소함을 확인하였다. 실리콘기름충전 기간 동안 특징적으로 내망막층의 두께가 감소하였으나, 약 3개월 기간 내에 실리콘기름을 제거한 경우 감소한 내망막층의 두께는 회복 가능함을 보여주고 있다. 실리콘기름충전술을 시행 받은 환자에서, 실리콘기름을 언제 제거하는 것이 시력저하 및 망막 구조 회복에 가장 좋은 결과를 보여주는지에 대해서는 아직까지 명확하게 정립되어 있지 않은 상태이다. 따라서, 향후 실리콘기름 충전 기간에 따른 망막두께 변화 및 시력 변화 간의 상관관계에 대한 추가적인 연구가 뒷받침된다면 실리콘기름이 안구 내에 충전되어 있는 기간에 따른 망막층별 두께의 변화가 실리콘기름을 제거하기 적절한 시기를 판단할 수 있는 지표 중 하나로 고려될 수 있을 것으로 생각된다.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






